Enrollees and health plans
This study was part of larger study designed to examine access, service use, and outcomes over time for a group of at-risk drinkers. Details of sampling, screening, recruitment, and follow-up have been described previously (
14,
15). List-assisted random-digit dialing was used to create a probability-based random sample of telephone numbers from Alabama, Arkansas, Georgia, Louisiana, Mississippi, and Tennessee. To generate a sample of approximately equal numbers of rural and urban residents, the sampling frame was stratified to oversample rural residents—that is, those not residing in a Metropolitan Statistical Area.
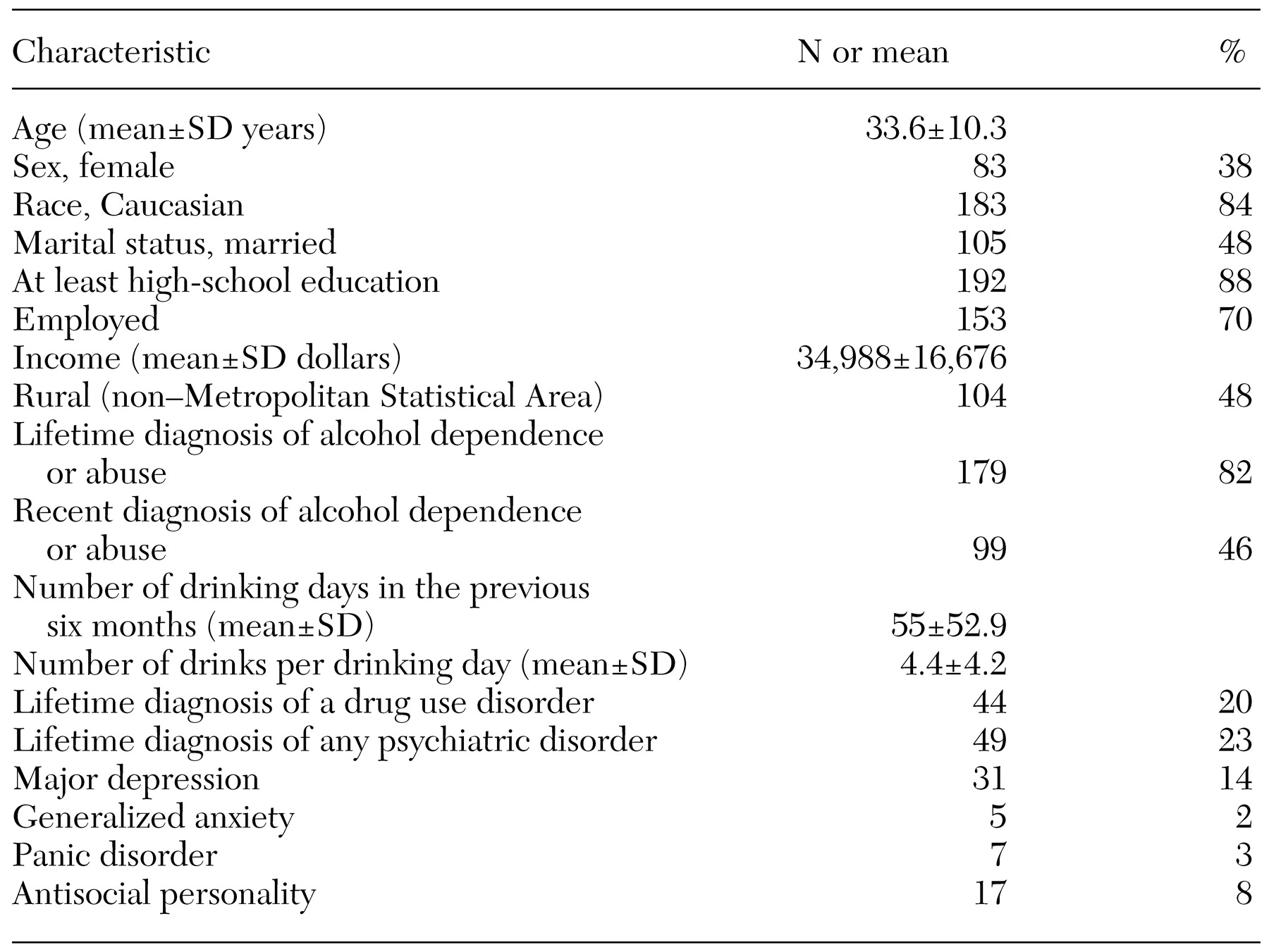
A brief screening instrument for at-risk drinking was administered by telephone to 12,348 adults, 960 (8 percent) of whom screened positive. The instrument defined at-risk drinking as meeting at least one lifetime DSM-IV criteria for alcohol abuse or dependence and at least one of several criteria in the previous 12 months: any abuse or dependence criteria; significant binge drinking, defined as at least 12 drinks on one occasion for men and eight drinks for women; or frequent heavy drinking, defined as at least five drinks for men and at least three drinks for women in a typical drinking day (at least once a week in the past 12 months or on at least 21 out of the previous 28 days).
A total of 733 (76 percent) of the respondents who screened positive for at-risk drinking were successfully recruited into the four-wave longitudinal study (baseline interview and six-month, 12-month, and 18-month follow-up interviews). Participants did not significantly differ from nonparticipants in demographic and clinical characteristics (
16). Follow-up rates exceeded 90 percent at each wave, resulting in 573 participants (78 percent) who completed the 18-month interviews, which were administered between March 1997 and March 1998. Participants who did not complete the interviews were more likely than those who did complete the interviews to be Caucasian, male, and to live in a rural area but were not significantly different on the other dimensions examined (
15).
At the completion of the 18-month interview, participants were asked to provide written consent to the collection of insurance records by the research team and to provide the names, addresses, and policy numbers of all insurers for the previous six months of the study period. The protocol and consent form were approved by the institutional review board of the University of Arkansas for Medical Sciences.
Written consent was provided by 442 (77 percent) of the study participants. Those who provided written consent were not significantly different in clinical or demographic characteristics than those who did not. Of those who provided consent, 142 (32 percent) reported that they were not insured or reported incorrectly that they had health insurance. Attempts were made to contact all the health plans listed by the insured study participants (N=300) in order to administer a telephone survey about the participants' benefits and coverage dates. Complete health plan survey data were collected for 217 (72 percent) of the insured participants. Those with complete health plan data were not significantly different from those who did not have complete health plan data in terms of clinical or demographic characteristics.
Research assistants contacted personnel from the customer service, claims, and provider services departments of the health plans to administer the survey. The research assistant verified that the enrollee's name corresponded with the policy number and that the coverage dates overlapped the study window. If a health plan reported that enrollees needed to get authorization from a carve-out specialty behavioral health organization to see a behavioral health specialist, the name and telephone number of the behavioral health plan was obtained. Survey items that pertained to behavioral health coverage were then administered by telephone to a representative of the specialty behavioral health organization. We successfully administered the behavioral health plan survey to 38 (70 percent) of the carve-outs. For the remaining 16 carve-outs (30 percent), we used responses about behavioral health coverage from the main health plan. The health plan information that was collected pertained to the date that the health plan survey was administered (January 1998 through June 1998), and all surveys were conducted after the Federal Mental Health Parity Act of 1996 went into effect (January 1998).
Benefit measurement
The survey asked about the type of health plan in which the at-risk drinker was enrolled: indemnity, health maintenance organization (HMO), preferred-provider organization (PPO), point-of-service (POS) plan, or other. Questions about outpatient mental health and substance abuse coverage, gatekeeping (including carve-outs), restrictions on choice of provider, deductibles, limits, coinsurance, and copayments were also included in the survey. Questions about utilization review were not asked because of measurement difficulties. The survey was designed to measure capitation at the health plan level, but the item was dropped from the analysis because 29 percent of the respondents could not answer the question.
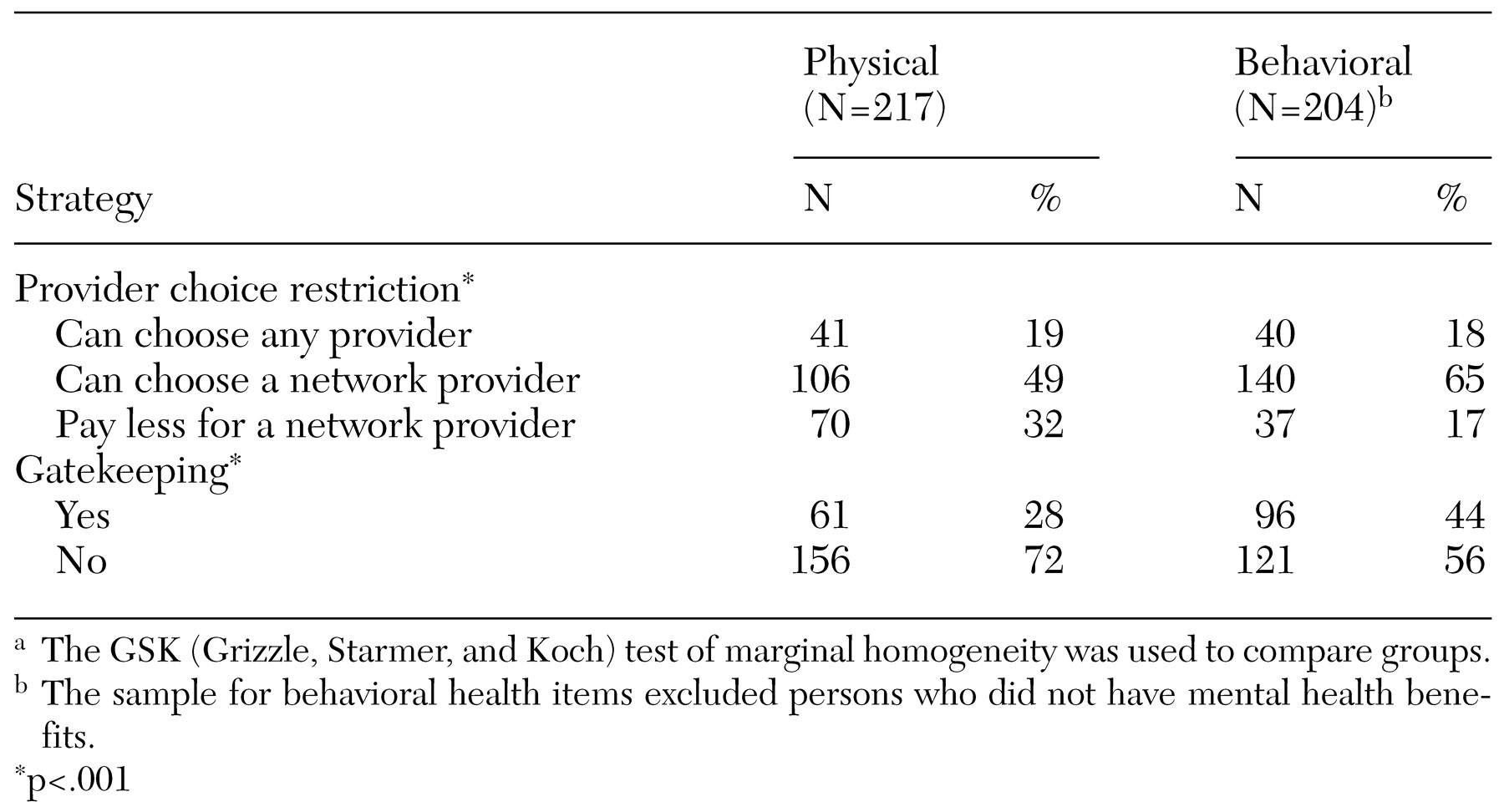
Gatekeeping for physical health services was assessed by asking "Do enrollees have to get authorization from a primary care provider to see a medical specialist?" Gatekeeping for behavioral health services was assessed with the question "Do enrollees have to get authorization from any of the following to see a mental health or substance abuse specialist?" Respondents were asked to check all the responses that applied, including primary care physician, specialty behavioral health company, employee assistance program, health plan representative, and other/please specify.
From the perspective of an enrollee who must get authorization from a behavioral health organization, the carve-out functions as a gatekeeper to the specialty behavioral health sector. If enrollees receive care in the specialty sector, behavioral health organizations typically use additional strategies to contain costs and promote high-quality care. For enrollees who were required to get authorization from a carve-out to visit a behavioral health specialist, the additional cost-containment strategies used by behavioral health organizations—for example, provider choice restrictions, deductibles, coinsurance, copayments, and limits—were captured by separate survey items.
Provider choice restrictions for physical health services were assessed by asking "For physical health problems, are enrollees required to choose from a list of approved providers, allowed to choose any provider they want, or allowed to choose any provider but have to pay more if they don't choose from the list?" Provider choice restrictions for behavioral health services were assessed with the question "For mental health and substance abuse problems, are enrollees required to choose from a list of approved specialists, allowed to choose any specialist they want, or allowed to choose any specialist but have to pay more if they don't choose from the list?"
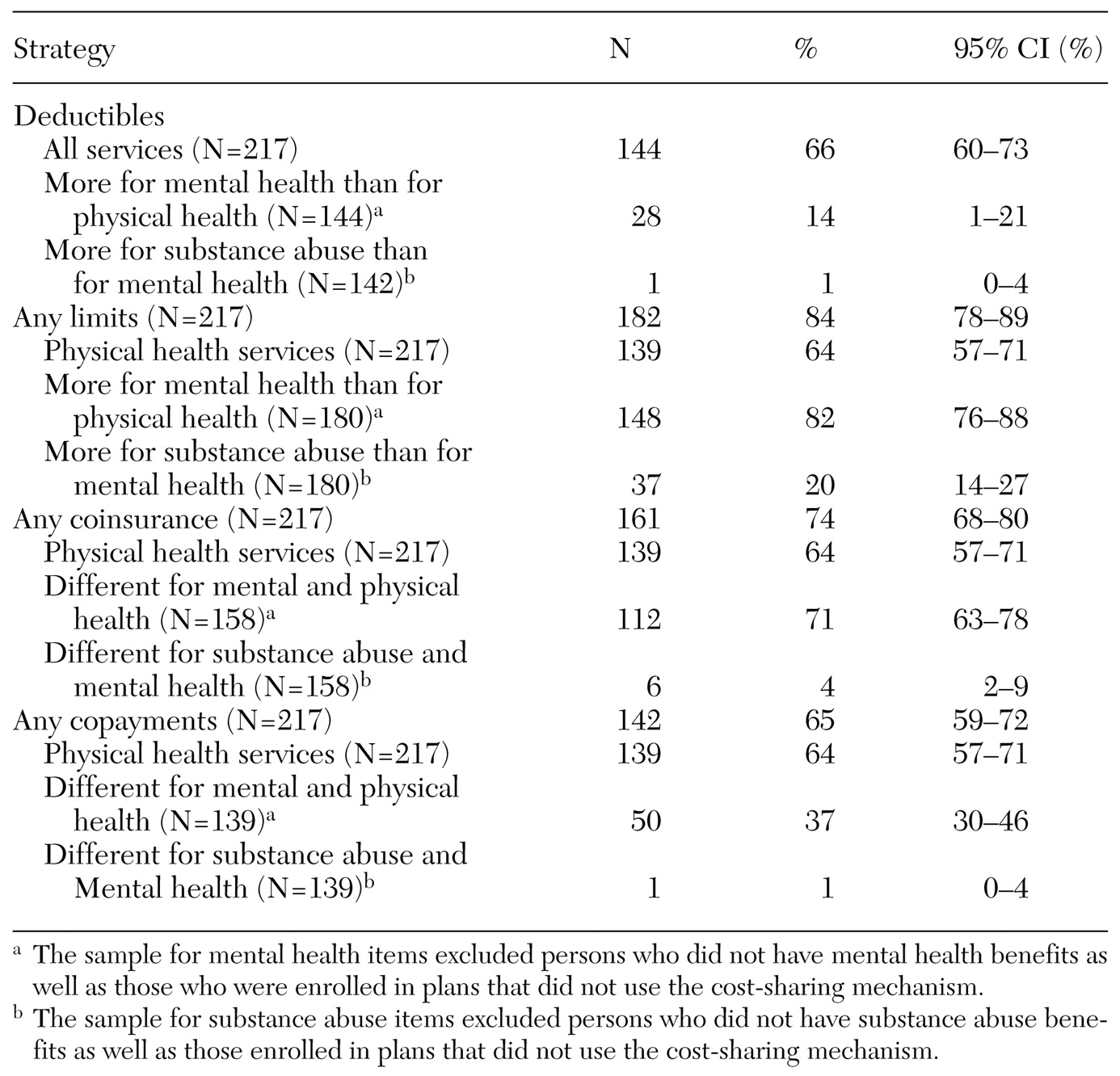
In responding to the survey items that were designed to gauge the four demand-side cost-sharing mechanisms—deductibles, limits, coinsurance, and copayments—respondents first indicated whether the cost-sharing mechanism was used. If an affirmative response was given, respondents were asked to indicate whether the mechanism was applied to physical health services. The survey then asked about "additional" deductibles and limits or "different" coinsurance and copayment levels for mental health services compared with physical health services and for substance abuse services compared with mental health services.
Because health plans use different combinations of mechanisms to increase cost-sharing for behavioral health, it is difficult to compare the total level of cost-sharing for physical health and behavioral health by examining each mechanism separately (
10). Therefore, we created a behavioral health benefit generosity index for each health plan policy, which combines the impact of each cost-sharing mechanism into a single measure. For each health plan policy, the benefit generosity index measures the average annual out-of-pocket costs a behavioral health service user would incur for outpatient behavioral health services. The generosity index is calculated for each health plan on the basis of deductibles, coinsurance, copayments, and limits for mental health and substance abuse. Rather than specifying a standardized service use pattern based on expert opinion or treatment guidelines, we chose to base the generosity index on the actual behavioral health services used by study participants.
Annual service use data were generated for 26 users of behavioral health services by abstracting the study participants' medical and billing records to identify behavioral health diagnoses and charges. (The 17 study participants for whom psychotropic medications were prescribed but who did not receive a behavioral health diagnosis were not included in the calculation of the generosity index.) The 26 behavioral health service users differed from the nonusers in age (p<.05), sex (p<.01), employment status (p<.01), and recent alcohol disorder (p<.05). On the basis of the assumption that the 26 users of behavioral health services would have used the same amount and type of services regardless of the health plans that covered them, hypothetical annual out-of-pocket costs were calculated for each of the 26 services users as if he or she were enrolled in each of the health plans represented in the sample. This assumption would be violated if enrollees modified their service use pattern in accordance with the benefit design of their health plan in order to minimize out-of pocket costs. If the assumption were violated, the generosity index would be biased toward zero (more generous) for the selected study participant's health plan and other similar health plans.
For each health plan, the out-of-pocket costs were averaged across the 26 service users to generate the benefit generosity index. In addition, for each plan, we calculated what the out-of-pocket costs would have been if cost-sharing for behavioral health was the same as cost-sharing for physical health—that is, full parity. The difference in the generosity indexes for behavioral health and physical health represents the level of mental health parity. Because enrollees would be likely to use more behavioral health services if their behavioral health benefits were the same as their physical health benefits, this index does not represent the expected out-of-pocket costs under full parity.