The relationship between attention deficit hyperactivity disorder (ADHD) and bipolar disorder is unclear. Studies examining the rates of ADHD in bipolar patients consistently show higher than expected rates.
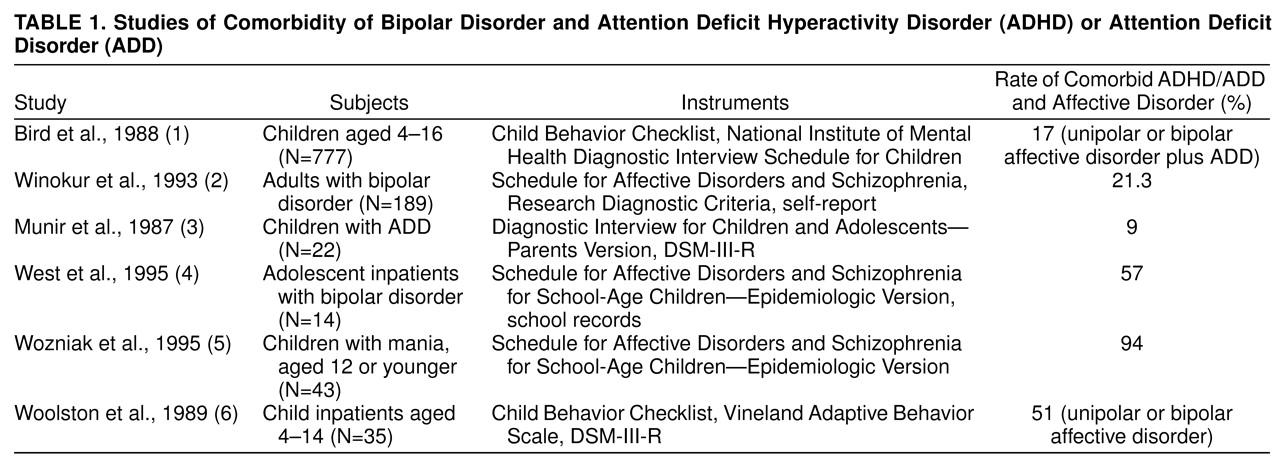
Table 1 lists studies
(1–
6) examining the rates of comorbidity for ADHD and bipolar disorder. The methods used in these studies varied, and the comorbidity rates ranged from 9% to 94%.
Four testable hypotheses might explain the high rates of comorbidity of mania and ADHD: 1) comorbidity is a chance phenomenon, 2) comorbidity is an artifact of overlapping criteria, 3) comorbidity is due to a common diathesis that leaves patients vulnerable to separate illnesses, 4) symptoms of ADHD that precede the onset of bipolar disorder represent a prepubertal expression of illness antecedent to the development of a full affective episode.
Wozniak et al.
(5) found that among 262 children referred to a pediatric psychopharmacology clinic, 94% of the children meeting the criteria for mania also met the criteria for ADHD.
Studies suggest that the relationship is unlikely to be accounted for by symptom overlap or diagnostic uncertainty. Fristad et al.
(7) reported that items assessing “classic” manic symptoms (e.g., elevated mood, increased sexual interest, pressured speech, racing thoughts) from the Young Mania Rating Scale effectively discriminated between mania and ADHD in two groups of adolescents.
If childhood ADHD is an expression of the early onset of affective illness, the age at onset of bipolar illness should be earlier in subjects with comorbid ADHD than in subjects without ADHD.
METHOD
The Massachusetts General Hospital Bipolar Mood Disorder Program enrolled 120 patients with bipolar disorder into a naturalistic study from 1992 to 1994. Consenting participants in the naturalistic study were assessed by blinded research psychiatrists using a version of the Structured Clinical Interview for DSM-III-R
(8). Childhood psychopathology was assessed by using sections from the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Epidemiologic Version (K-SADS-E)
(9) and the Diagnostic Interview for Children and Adolescents—Revised
(10).
The subjects were classified as having late-onset bipolar disorder or early-onset bipolar disorder on the basis of age at onset of the first episode of depression, mania, or hypomania. Designation of early-onset bipolar disorder required consensus on the occurrence of the first affective episode before age 19 years, and late-onset bipolar disorder was defined as occurrence of the first affective episode after the 19th birthday.
For study purposes, the study group (N=56) was first divided into two subgroups according to whether the K-SADS-E interview indicated a history of ADHD. For comparison purposes, the eight subjects with bipolar disorder and a history of childhood ADHD were then age and sex matched with eight bipolar subjects without a history of childhood ADHD.
Statistical methods included paired t tests using the Statview statistical program for Macintosh.
RESULTS
Each of the two groups of subjects with bipolar disorder (with and without a history of childhood ADHD) consisted of seven subjects with bipolar type I and one with bipolar type II disorder. At the time of evaluation, the groups did not differ significantly in age (history of childhood ADHD: mean=38.0 years, SD=5.3; subjects without childhood ADHD: mean=37.7, SD=6.7) (unpaired t test, t=0.08, df=14, p=0.94).
The mean age at onset of the first affective episode was significantly lower for the subjects with a history of childhood ADHD (mean=12.1 years, SD=4.6) than for the subjects without childhood ADHD (mean=20.0 years, SD=11.3) (paired t test, t=–3.57, df=7, p<0.01).
Analysis of the matched subjects with bipolar disorder (N=16) revealed a ratio of early to late onsets similar to that observed in the overall naturalistic sample—81% (N=13) were categorized as having had early onsets, and 19% (N=3) had had late onsets. Among the subjects with early-onset bipolar disorder in this subgroup, 62% (eight of 13) met the criteria for ADHD, whereas none of those with late-onset bipolar disorder had ADHD (Fisher’s exact test, p=0.20, N=16). Thus, all of the observed cases of ADHD in our study group were found in the subjects with early onset of bipolar illness.
DISCUSSION
In our study group the mean age at onset of affective illness in the subjects with bipolar disorder and a history of childhood ADHD was significantly lower than in the subjects with bipolar disorder who did not have a history of childhood ADHD. In addition, all of the observed cases of childhood ADHD were found in the subjects with early-onset bipolar disorder. We analyzed the incidence of ADHD in the subjects with late-onset bipolar disorder in the overall study group (N=56) and found that none of them had a history of ADHD. Our findings are consistent with the hypothesized association between ADHD and earlier onset of affective illness in patients with a history of bipolar disorder.
Prior studies
(11–
14) suggest that early onset occurs in families with high loading for affective illness. Early-onset bipolar disorder may be a subtype with greater genetic loading and therefore increased vulnerability to the development of both early affective and nonaffective psychopathology.
The results from this preliminary study should be viewed with caution given the small number of subjects, and replication with a larger study group is required.
Our results raise methodological questions. Is the retrospective collection of data about childhood symptoms from adult subjects valid? Could early onset of bipolar illness be ADHD, or vice versa? We cannot eliminate the possibility of misdiagnosis; however, we used validated structured diagnostic instruments, decreasing potential clinician biases and inconsistencies in clinical assessment. It is hard to imagine our methods would systematically misassign diagnosis only in the patients with early onset of bipolar disorder.
The earlier onset of affective illness in patients with bipolar disorder and a history of ADHD suggests that ADHD in children of people with bipolar disorder might identify children at highest risk for development of bipolar disorder.