Major depression is a recurrent disorder of complex etiology. While both short-term environmental adversities such as stressful life events
(1) and long-term diatheses such as genetic risk factors
(2–
4) are important causal factors in major depression
(5), we know little about how these factors act over time. A leading hypothesis, first articulated by Kraepelin
(6), is that psychosocial stressors play a greater role in the initial than in subsequent episodes of depressive disorders. Over the course of illness, the onset of depressive episodes may become increasingly autonomous and less related to environmental adversities. More recently, this pattern has been hypothesized to result from a sensitization process to the state of depression
(7). Analogous to animal electrophysiologic models, this has been termed “the kindling hypothesis.” This hypothesis can also be expressed in mental language
(8):
However, these studies need to be interpreted in the context of five methodological issues. First, they all studied clinical samples, thereby introducing the possible confounding effect of help-seeking behavior. For example, a bias might arise if individuals with recurrent versus first episodes of depression were more willing to present for treatment in the absence of a major life stressor. Second, these studies all compared the proportion of affected individuals who reported a major stressful life event that preceded their onset of major depression or the average number of individual events. This approach is valid only if there are no changes in the base rate of stressful life events with repeated episodes of major depression, a questionable assumption. In statistical terms, the kindling hypothesis may be more appropriately evaluated as an interaction between the number of previous depressive episodes and stressful life events in the prediction of risk for an onset of major depression. Third, most studies divided their sample into only two groups (usually one versus two or more episodes [
9,
10,
12,
13,
15]), although two studies examined three
(11) and five groups
(14), respectively. None had a sufficient sample size to explore the “dose-response curve” of number of previous depressive episodes and depressogenic effect of stressful life events. For example, does the impact of stressful life events on risk for major depression decline linearly with increasing number of previous depressive episodes or does the “kindling effect” maximize out at some number of previous depressive episodes? Fourth, stressful life events vary both in their depressogenic potential and their independence of the respondent’s behavior
(16). An analysis of the relationship among previous depressive episodes, stressful life events, and risk for major depression should consider both the severity and independence of stressful life events. Fifth, these studies were all cross-sectional, comparing different patients in their first versus recurrent episodes. These studies cannot therefore determine whether the difference in the association between stressful life events and major depression in those with no versus multiple previous episodes is due to an effect of previous depressive episodes or to stable individual differences in event sensitivity in those with low versus high risk for major depression. Since those with recurrent major depression have a higher familial liability to illness than those with single episodes
(3,
17–
21), this difference might be mediated genetically. Therefore, one approach to this problem would be to control for interindividual differences in the level of familial risk to major depression. The most powerful approach, however, would be to follow individuals over time and examine whether, within individuals, the magnitude of the association between stressful life events and major depression changes as they accumulate more episodes of depressive illness.
In this study, we reexamine, addressing these methodological issues, the relationship among episode onset for major depression, number of previous depressive episodes, and stressful life events in a population-based sample of female twins followed longitudinally over four waves of personal interviews.
Results
Our analyses began with a total of 104,106 person-months of observation. In the basic model, one or more data points were missing in 156 person-months, and 2,994 person-months were censored because the individual was in an episode of major depression during that month. This left us with a total of 100,956 person-months that contained 1,419 onsets of major depression. In analyses that required information about the lifetime history of major depression in the co-twin, our sample consisted of 97,515 person-months with 1,380 depressive onsets.
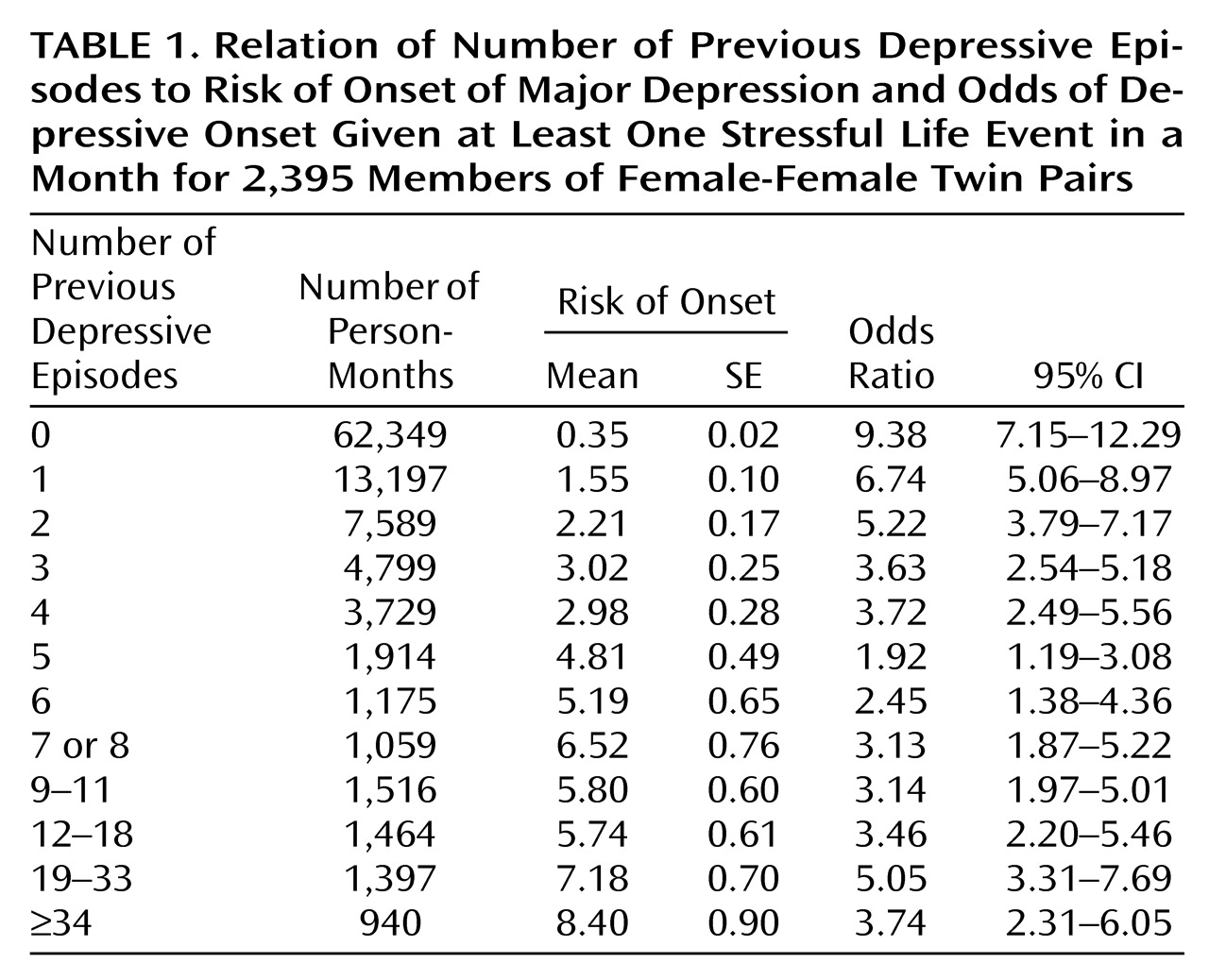
Before formal analysis, we explored the shape of the relationship between the number of previous depressive episodes and risk for depressive episodes. To do so, we divided person-months into 12 groups as a function of number of previous depressive episodes. As seen in
Table 1, each of these groups, except the last, contained at least 1,000 person-months. We then calculated the rate of depressive onsets in each group of person-months, and this varied from 220/62,349=0.35% for those with no previous depressive episodes to 79/940=8.40% for those with 34 or more previous depressive episodes. As seen in
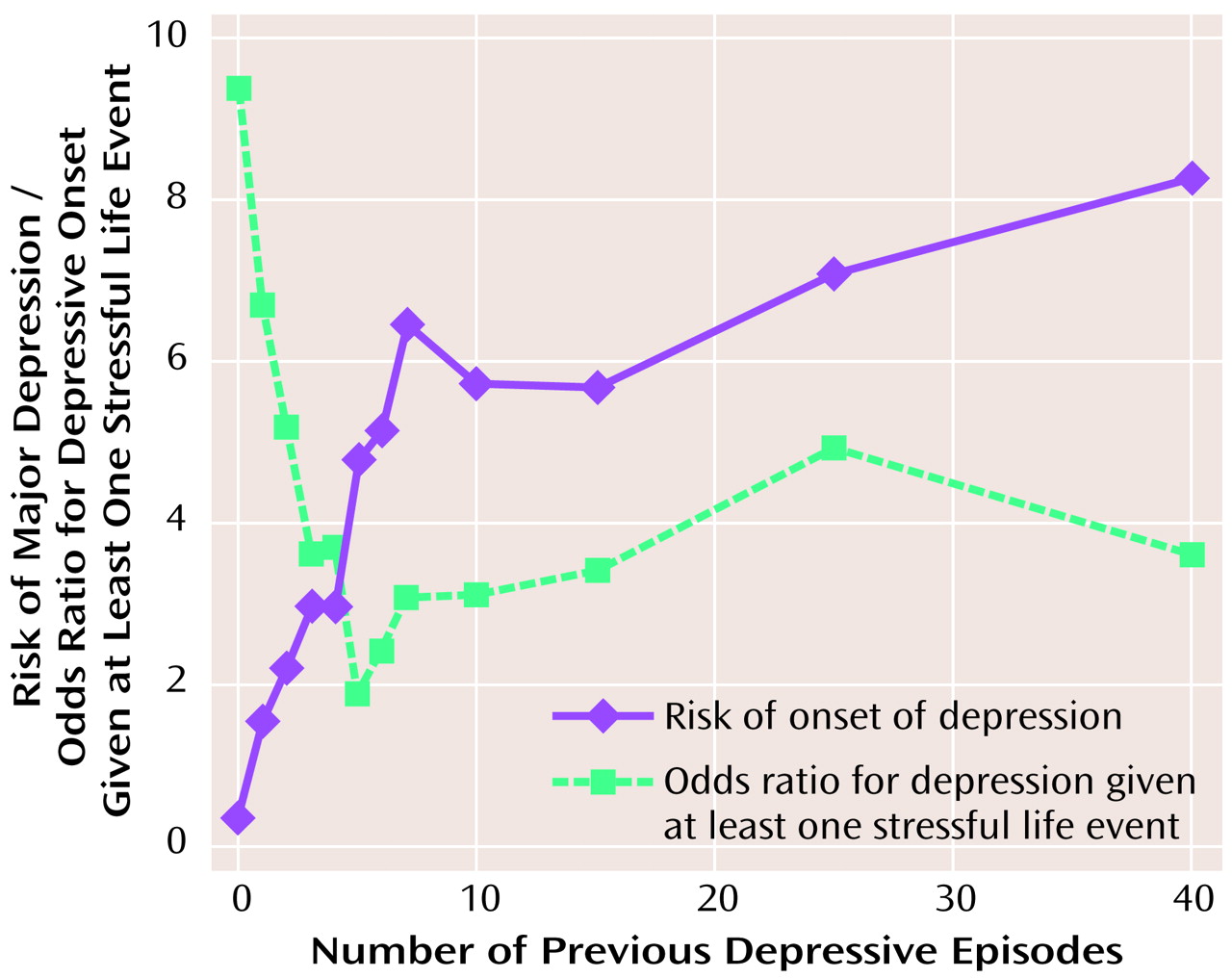
Figure 1 and
Table 1, the relationship was biphasic: the risk for a depressive episode rose steeply as the number of previous depressive episodes increased from none to approximately eight or nine. As the number of previous depressive episodes increased beyond this point, the risk for major depression dipped slightly and then rose again but at a much slower rate.
Discrete-Time Survival Models
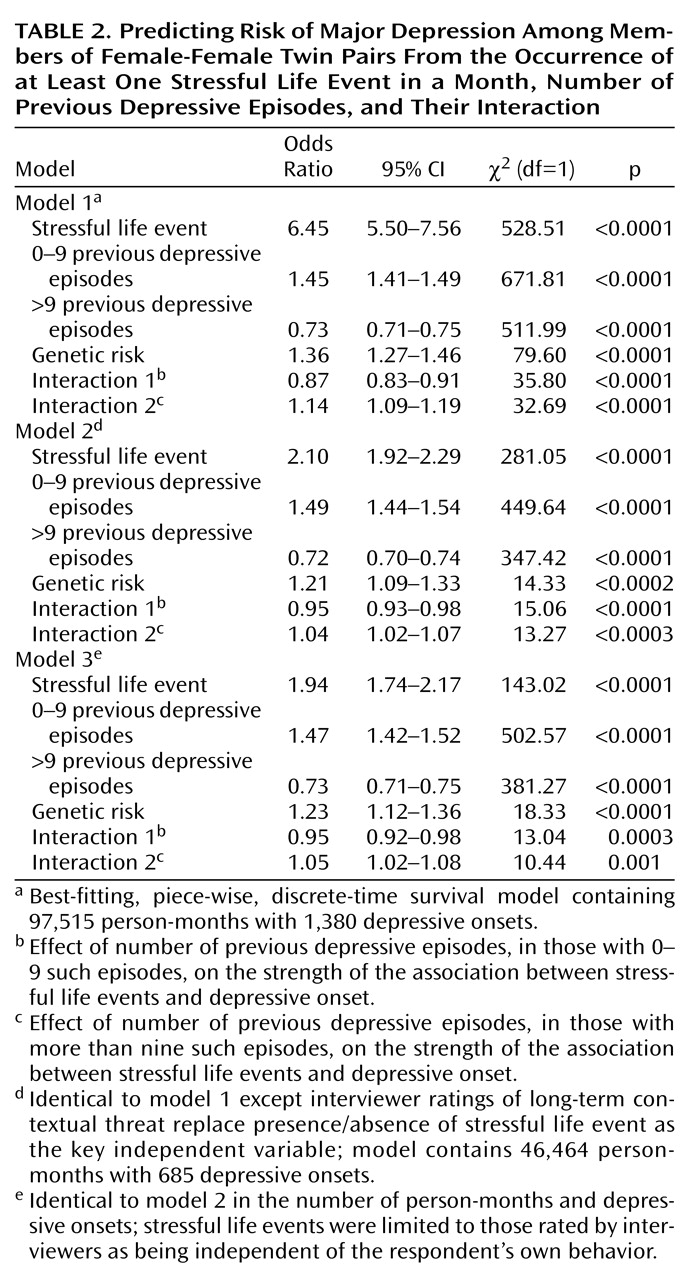
We present in detail results for the models in which we attempted to predict, for each month, the risk of a depressive onset from the occurrence of one or more stressful life events (coded as a dichotomous variable), the number of previous depressive episodes, and their interaction. Given the shape of the relationship revealed in
Figure 1, we fitted model 1 with two linear components (i.e., a piece-wise regression), determining the optimal inflection point by testing sequentially each point from one to 12 previous depressive episodes. For this and all subsequent models, the best model likelihood was seen for an inflection point at nine previous depressive episodes. Only 5,299 person-months (5.2% of the total) had nine or more previous depressive episodes, so our analyses will focus on the first linear component, which contains most of our data.
As seen in
Table 2, the occurrence of one or more stressful life events, with an odds ratio of 6.45, had a strong impact on the risk for a depressive onset. The impact of the number of previous episodes was divided into two regression lines of differing slope. From zero to nine, the number of previous depressive episodes strongly predicted an increasing risk for a depressive episode with an odds ratio of 1.45. For more than nine previous episodes, the odds ratio was 0.73 × 1.45=1.06. Once an individual had accumulated at least nine previous depressive episodes, the increased risk associated with each additional episode was modest, although statistically significant. Also, as expected, the rate of depressive onsets was significantly predicted by level of genetic risk.
Our key hypothesis predicted an interaction in the prediction of risk for major depression between the number of previous depressive episodes and stressful life events. Specifically, we predicted that with an increasing number of previous depressive episodes, the strength of the association between stressful life events and depressive onsets would diminish. For those person-months in individuals with zero to nine previous depressive episodes, we saw exactly this kind of interaction (χ2=35.80, df=1, p<0.0001; odds ratio=0.87). This odds ratio means that for each additional previous depressive episode from zero to nine, the strength of the association between stressful life events and depressive onsets declined approximately 13%. There was also a significant interaction between number of previous depressive episodes and stressful life events in predicting major depression for those with nine or more previous episodes (χ2=32.69, df=1, p<0.0001; odds ratio=0.87 × 1.14=0.99). As the number of previous depressive episodes increased beyond nine, the strength of the association between stressful life events and depression continued to decline but at a much slower rate (approximately 1% per episode).
To illustrate these results, we calculated, from the raw data, the odds ratio between major depression and one or more stressful life events as a function of the number of previous depressive episodes (
Table 1 and
Figure 1). The interaction between stressful life events and previous depressive episodes from zero to nine in the prediction of depressive onsets is clearly seen. For individuals with no previous depressive episodes, life event occurrence and the onset of major depression is strongly associated (odds ratio=9.38). The odds ratio, however, drops swiftly to the range of 2 to 3 as the number of previous depressive episodes increases to five through eight. The interaction between stressful life events and nine or more previous depressive episodes in the prediction of major depression cannot be clearly seen with this raw data, since there appears to be no overall change in the strength of the association between stressful life event and major depression as the number of previous depressive episodes further increases.
In the last two waves of personal interviews, we collected information on long-term contextual threat and dependence for each individual stressful life event. Including data from subjects who reported a lifetime history of major depression in the co-twin provided 46,464 person-months of exposure and 685 onsets of major depression. Model 2 was identical to model 1 except that we used the long-term contextual threat ratings assigned by the interviewers as the key independent measure. That is, instead of predicting onsets of major depression from the presence or absence of a stressful life event in a given month, we now predicted depressive onsets from a 5-point scale ranging from no event to an event of maximal long-term contextual threat. The best-fit model was qualitatively very similar to that seen with model 1 (
Table 2). We found strong main effects for the impact of genetic factors, stressful life events, both components of the regression line for number of previous depressive episodes, and strong evidence in favor of the kindling effects in that both interactions between previous depressive episodes and stressful life events were highly significant.
Our two previous models had included all stressful life events including those likely to be a result of the respondent’s own actions. Therefore, our final model was restricted only to those life events rated by interviewers as probably or definitely independent of the respondent’s own behavior. Although the number of person-months with stressful life events declined, the overall pattern of findings was remarkably similar. The significance of the main effect of stressful life events declined due to the reduced number of events. However, both the main effects of the number of previous depressive episodes as well as the interactions between the number of previous depressive episodes and stressful life events were similar to that seen with the previous models (
Table 2).
Within-Person Analyses
The final question we sought to answer was whether the change in sensitivity to the effects of stressful life events over episodes varied within as well as across individuals.
To address this question, we used a fixed-effects partial likelihood Cox proportional hazards model
(33) with the addition of multiple time-dependent failures and time-dependent covariates. Because of limited power, we only examined the first linear component of the relationship between previous depressive episodes and risk for major depression (i.e., between zero and nine previous depressive episodes). We began by fitting this model to the entire data set, estimating a single underlying hazard function. The parameter estimates of this model were quite similar to those found with our discrete-time survival analyses (
Table 1). In particular, we found a highly significant interaction between number of previous depressive episodes and the occurrence of one or more stressful life events (b=–0.13, χ
2=33.85, df=1, p<0.0001; odds ratio=0.88). Next, we stratified by individual, assuming a separate hazard function for each person in the sample. The magnitude of the interaction between previous depressive episodes and stressful life events was essentially unchanged (b=–0.12, χ
2=11.74, df=1, p=0.0006, odds ratio=0.89). These results indicate that the observed decline in the association between stressful life events and depressive onsets with increasing numbers of previous depressive episodes is a true within-individual phenomenon and cannot be explained by systematic differences between the kind of individuals who have a low versus high number of previous depressive episodes.
Discussion
The goal of this study was to clarify the impact of the number of previous depressive episodes on the association between the occurrence of stressful life events and the risk for depressive episodes. Consistent with the kindling hypothesis, previous research had suggested that the strength of the relationship between stressful life events and major depression declined with an increasing number of previous depressive episodes
(9–
15). However, these previous studies had at least several potential methodological limitations that we were able to address in our analyses. We first review our results and then interpret them in the light of these potential methodological issues.
In examining the raw data on previous depressive episodes, stressful life events, and depressive onsets in our sample of over 100,000 person-months of exposure, two facts became clear. First, the number of previous depressive episodes had a strong effect on the association between stressful life events and depressive onsets. Second, the shape of this relationship was biphasic. An increase in previous depressive episodes impacted much more strongly on the relationship between stressful life events and major depression when the number of previous depressive episodes was less than 10.
We modeled this biphasic relationship by using discrete-time survival analysis and piece-wise regression. Across all models, the best fit was found when the point of inflection in the biphasic regression curve was set at nine previous depressive episodes. We then presented the parameters of a series of best-fit models. Qualitatively, the models all told the same story. As shown by numerous previous investigators (e.g., references
34–
38), stressful life events were strong risk factors for the onset of major depression. The main effect of previous depressive episodes was divided into two portions. When the number of previous depressive episodes was nine or fewer, each additional previous depressive episode conveyed a large increased risk for a depressive onset. After nine previous depressive episodes, each additional episode conveyed a much smaller increased risk.
Our real interest, however, was in testing whether, as predicted by the kindling model, we would observe an interaction between previous depressive episodes and stressful life events in the prediction of risk for major depression. Indeed, we found strong and consistent evidence for a negative interaction. That is, with each new previous depressive episode, the association between stressful life events and onsets of major depression became progressively weaker. This effect was striking between zero and six to eight previous depressive episodes. These results are consistent with prediction of the kindling hypothesis.
Given the nonexperimental nature of these results, a careful review of possible sources of biases is warranted. First, because our twins were selected from a birth-certificate-based twin registry, these results cannot plausibly result from the confounding effect of help-seeking behavior. Second, by testing the kindling hypothesis as an interaction between stressful life events and previous depressive episodes, we ensured that our results could not be influenced by changes in the base rate of stressful life events with increasing number of previous depressive episodes, which was indeed seen in our data. Third, the severity of stressful life events was positively and significantly correlated with the number of previous depressive episodes. That is, individuals with large numbers of previous depressive episodes on average had more severe kinds of stressful life events. In the last two waves of our sample, on the basis of information provided by the respondent, interviewers rated each individual stressful life event on a measure of severity (long-term contextual threat
[27]). Controlling for the severity of stressful life events produced no substantial change in the pattern of results.
Fourth, the greatest interpretational difficulty with previous studies of the kindling hypothesis is the problem of clarifying the causal relationship between previous depressive episodes and the association between stressful life events and major depression. While the pattern of results from these cross-sectional studies could result from a causal impact of previous depressive episodes on event sensitivity, a noncausal explanation is also plausible. Assume that we could divide individuals into two groups, the first of which has a low liability to major depression so that depressive episodes only occur in the setting of severe stressful life events. The second group, which has high liability to major depression, frequently has episodes without substantial environmental stress. In a cross-sectional study of depressed patients, the mixture of these two groups would produce an apparent association between number of previous depressive episodes and the stressful life event-major depression relationship. This would occur because the first group would predominate in those with no previous depressive episodes (where the association between stressful life events and major depression would be strong) and the second group would be more common in those with recurrent episodes (where the association between stressful life events and major depression association would be weak).
We proposed two ways to address this critical interpretational difficulty. Because of the twin structure of our data, we controlled for the level of genetic risk to major depression in all of our analyses. Because of the longitudinal nature of our data, we could also examine within-individual changes in event sensitivity with increasing previous depressive episodes. For example, imagine an individual twin whom we interviewed over all four waves and who therefore had 52 person-months of observations in our data. Assume that she had her first depressive episode in months 9 to 11 and a second episode in months 40 to 44. We could compare the strength of the association between the occurrence of stressful life events and the risk for major depression in months 1–9 (when she had no previous depressive episodes), 12–40 (when she had one previous depressive episode) and 45–52 (when she had two previous depressive episodes). (She would be censored from analysis for months 10 and 11 and 41–44 when she was in a depressive episode.) Controlling for interindividual differences in liability to major depression, these analyses strongly supported a causal interpretation of the kindling effect because they showed a substantial reduction in the strength of the association between stressful life events and major depression within individuals as they accumulated more previous depressive episodes over time.
These results should be interpreted in the context of six potential methodological limitations. First, the study group was entirely female, and it cannot be assumed that the same relationship between previous depressive episodes, stressful life events, and major depression would be seen in male subjects. Second, all participants were twins. However, twins have rates of psychiatric symptoms
(39) and disorders
(40) similar to the general population. Because the subjects came from twin pairs, nonindependence of observations from members of a pair is a potential concern. We have previously examined the correlation in twin pairs for the key dependent variable (month of occurrence of a depressive onset) in this group, and it was too low (kappa=0.01) to be of practical concern
(26). To further examine the possible magnitude of this problem, we re-ran model 1 by using general estimating equations
(41) to correct for the correlations in twin pairs. The parameter estimates changed trivially.
Third, as in most such studies, stressful life events and the onset of major depression were rated retrospectively over the 1-year period before interview. Although stressful life events were assessed in a separate and earlier section of the interview than major depression, part of the observed association could be spurious and result from biased recollection.
Fourth, the reliability of the assessment of lifetime major depression in community samples is modest
(42,
43). As the 1-year periods of assessment in our longitudinal sample were not contiguous, the accuracy of our assessments of depressive episodes in the intervening periods is likely to be of only moderate accuracy. Also, among those who report a lifetime history of major depression, the number of reported previous depressive episodes is also of only moderate reliability. In this study, short-term test-retest for number of previous depressive episodes, as assessed by a Spearman rank correlation was 0.48 (N=192; p<0.0001), similar to that found previously
(44,
45).
Fifth, these analyses included 18 twins with a lifetime diagnosis of mania or hypomania
(46). Since the kindling process may differ in bipolar and unipolar illness, we reran model 1 excluding these twins. The results did not change substantially.
Finally, we assumed that when a stressful life event and depressive onset occurred in the same month, the stressful life event came first. In a section of the interview separate from that which evaluated stressful life events, respondents with a depressive syndrome in the last year were asked, “Did something happen to make you feel that way or did the feeling just come on you ‘out of the blue?’ ” We have examined, in two separate waves of our data, twins who reported a stressful life event and a depressive onset occurring in the same month, and who answered this question in sufficient detail to examine. We found that 84%
(25) and 85%
(26) responded with the stressful life event they had previously reported as occurring in the same month. In none of the remaining cases did the interview indicate that the stressful life event occurred as a result of the onset of a depressive episode.