Although kleptomania was described at the end of the 19th century
(1–
3), it remains a poorly understood behavioral disturbance. The exact prevalence is not known since this disorder is probably rare and because social stigma discourages patients from seeking treatment. Nevertheless, kleptomania is thought to be more frequent in females
(4). Impulsivity, a major psychopathological construct, is a key feature of several psychiatric disorders, including kleptomania
(5). Thus, pathological theft was included in the impulse-control disorder categories of DSM-IV and ICD-10. This discrete condition has been hypothesized to belong to several distinct clinical spectrums, including obsessive-compulsive, affective, and addictive disorders
(6–
8). These categorizations are supported not only by specific clinical and phenomenological features but also by the high rate of comorbidity of kleptomania with the major disorders in each spectrum. For example, kleptomania has been considered an antidepressive behavior because of its high rate of comorbidity with depression
(9). In that view, kleptomania can be seen as a subject’s misadaptation to a depressive mood state and, as such, the disorder could be context dependent. This phenomenological explanation has been advocated since the beginning of the 20th century
(10) and supported by more recent observations of distinct behavioral disturbances (e.g., kleptomania, compulsive buying, sexual compulsion) alternating with depression in the same subjects, with onset of the behavioral disturbance associated with relief of the mood state and cessation of the behavior associated with recurrence of depression
(11). Most of the published reports have been based on single cases. Only three studies included groups of patients, and the number of patients in each study was small. Using a semistandardized interview designed specifically for their study, Presta et al.
(12) found a high rate of mood disorders in 20 patients with kleptomania. Using a standardized structured interview, McElroy et al.
(13) had previously found a similarly high rate of mood disorders in the same number of subjects. Sarasalo et al.
(14) studied personality traits and found high sensation-seeking scores in 34 patients with kleptomania. However, to our knowledge, no controlled psychopathological study has been conducted, and impulsivity has never been specifically assessed in kleptomania. Therefore, we assessed impulsivity, sensation seeking, and mood in patients with kleptomania, compared to psychiatric patients without an impulse-control disorder or substance-related disorder and to patients with alcohol abuse or dependence. We hypothesized that patients with kleptomania would score higher on impulsivity than the other patients, independently of mood. A second aim was to explore the clinical features of kleptomania comorbidity, especially with mood, impulse-control, and substance-related disorders.
Results
Of the 11 patients with kleptomania, one did not complete the self-report questionnaires. Twenty-nine psychiatric patients without impulse-control or substance-related disorders and 60 patients with alcohol abuse or dependence were included.
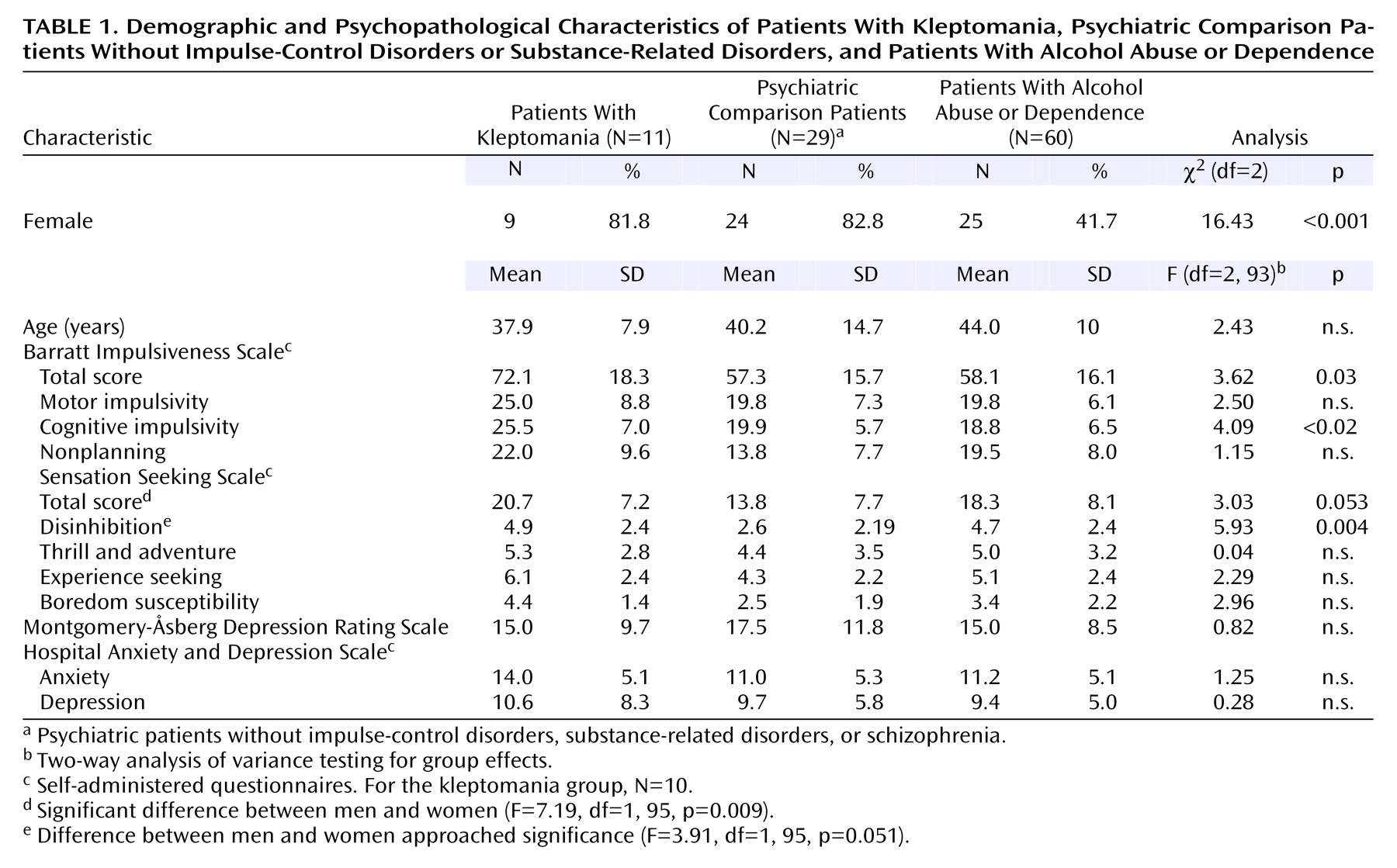
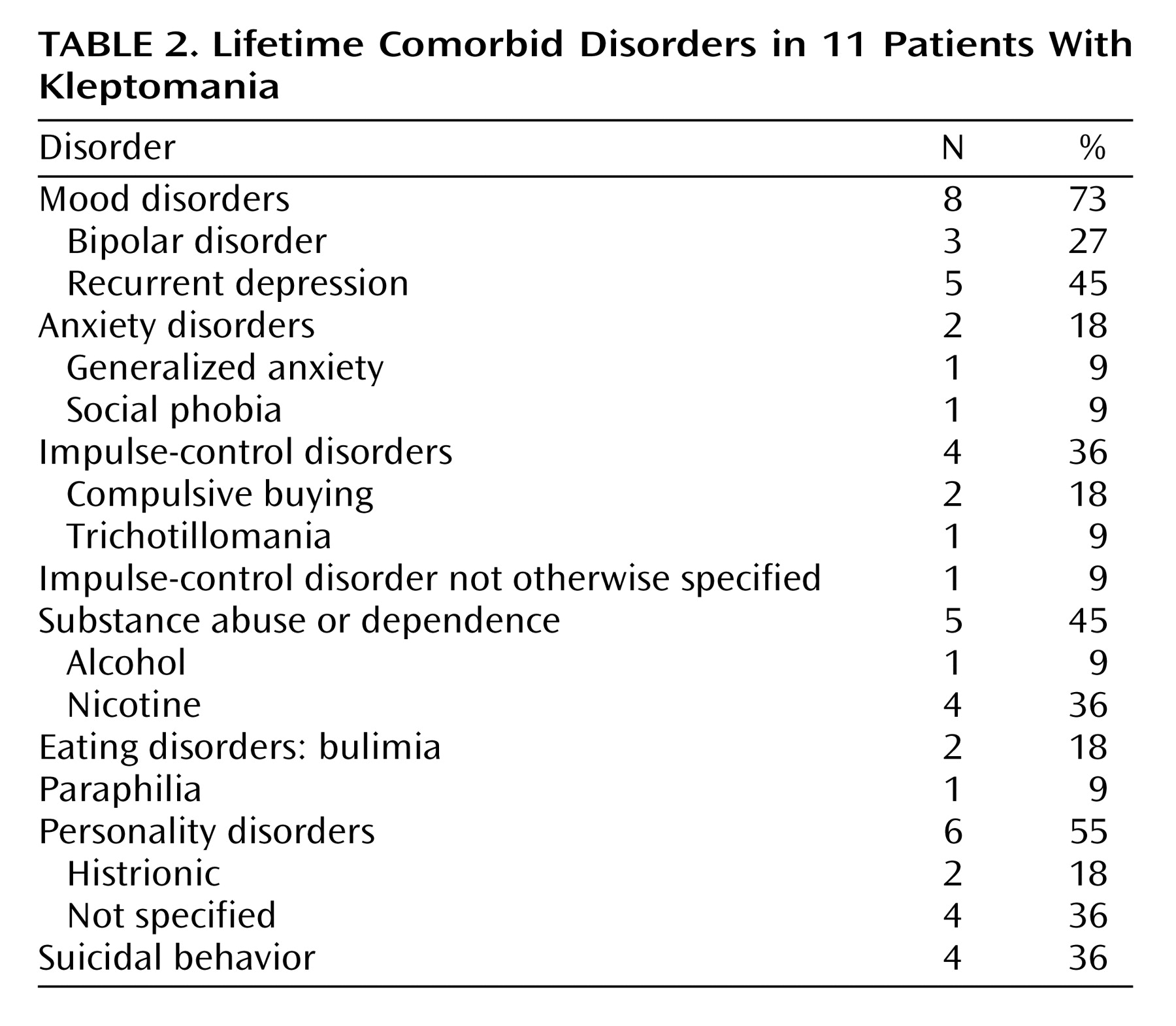
Table 1 summarizes the demographic and clinical characteristics of the three groups. Most patients with kleptomania were female (82%). The three groups did not differ in mean age (F=2.43, df=2, 93, p>0.09), age did not differ by gender (F=0.70, df=1, 93, p>0.40), and the interaction of age and gender had no significant effects (F=0.23, df=2, 93, p>0.80). For the patients with kleptomania, the mean age at onset of the disorder was 30.3 years (SD=11.8), and the average duration of illness was 6.1 years (SD=9.8). IQ (available for four patients with kleptomania) was normal, and all the patients had reached a university academic level. Neurological examinations of the patients with kleptomania were normal, and none had organic brain syndrome or encephalopathy. CT brain scan and EEG results (available for four patients with kleptomania) showed no significant abnormalities. There was a high rate of comorbidity of kleptomania with mood disorders, other impulse-control disorders, and substance abuse or dependence (mainly nicotine addiction). Only one patient with kleptomania also had a major substance (alcohol) abuse or dependence disorder (
Table 2). No specific pattern of onset of the impulse-control disorders could be established. Kleptomania started 1 year after the onset of bulimia for the two patients with that eating disorder and several years after the onset of compulsive buying for the two patients with that disorder. A retrospective chart review showed that kleptomania and mood disorder clearly alternated over time in five patients and probably alternated in one patient. All patients with kleptomania but one were given medications: two received a mood stabilizer (carbamazepine for one patient and valproic acid for the other), five received an antidepressant, and three received both an antidepressant and a mood stabilizer (an antidepressant and lithium for two patients and an antidepressant and valproic acid for one patient). At discharge, the treatment response of 10 patients was evaluated, and after 1 year, the treatment response of five patients was evaluated. In the short term, kleptomania as well as depression improved in all patients. No differences in response to treatment were observed between those who received a mood stabilizer only and those who received an antidepressant only. Of the five patients seen after 1 year, one remained free of symptoms, two had had a relapse of depression, one had had a relapse of kleptomania, and one had had a relapse of both depression and kleptomania.
We found a significant group effect but no gender effect for the Barratt Impulsiveness Scale total and cognitive impulsivity scores (
Table 1). The mean total scores showed that the patients with kleptomania were more impulsive than the psychiatric comparison patients (t=2.45, df=37, p<0.02) and the patients with alcohol abuse or dependence (t=2.49, df=68, p<0.02). The patients with kleptomania had higher cognitive impulsivity scores than the psychiatric comparison patients (t=2.53, df=37, p<0.02) and the patients with alcohol abuse or dependence (t=3.01, df=68, p<0.004). There were no significant differences between the latter two groups for either score. A significant difference among the three groups was found for the Sensation Seeking Scale disinhibition score. For the Sensation Seeking Scale total score, the difference among groups approached significance and the gender difference was significant (
Table 1). The patients with kleptomania and the patients with alcohol abuse or dependence had similar Sensation Seeking Scale total and disinhibition scores. The scores for both groups were significantly different from those for the psychiatric comparison patients (total score: t=2.46, df=37, p<0.02, and t=2.49, df=87, p<0.02, respectively, and disinhibition score: t=2.76, df=37, p<0.009, and t=4.03, df=87, p<0.001, respectively). Although the difference among groups was not significant, the patients with kleptomania had higher scores than the psychiatric comparison patients for experience seeking (t=2.21, df=37, p<0.04) and boredom susceptibility (t=2.85, df=37, p<0.007) but not for thrill and adventure seeking. No significant group effect and no differences between specific groups were found for the mood and anxiety measures.
Discussion
As in earlier studies of patients with kleptomania, we found a high rate of comorbidity, especially with mood disorders. No significant differences were found between groups on anxiety and mood measures. The rates of comorbid substance abuse and dependence and impulse-control disorders in patients with kleptomania were high, but lower than those for mood disorders. No lifetime obsessive-compulsive disorder and related disorders such as nail biting, psychogenic excoriation, and tics were found in the patients with kleptomania in our study
(22). The comorbid disorders that were found in the patients with kleptomania share common clinical features and to some extent a common phenomenology. Our data support the inclusion of kleptomania in the affective disorders spectrum. We found that the treatment response to antidepressants or mood stabilizers in both mood disorder and kleptomania was better in the short term and worsened with time. No specific effect of treatment on the theft behavior can be pointed out, because the pathological conditions were mixed. It is interesting to note that one patient took successively four distinct selective serotonin reuptake inhibitor medications. Because she could not see enough improvement, she successively stopped the medication and asked for more. With each drug, her kleptomaniac behavior was similarly decreased without being completely eradicated. Moreover, she did not have symptoms of a comorbid mood disorder.
Unlike the comorbidity rate of mood disorders, the comorbidity rate of substance-related disorders was low in patients with kleptomania, especially if nicotine dependence was considered to be of minor importance compared with alcohol dependence.
Furthermore, measures of impulsivity were higher in the patients with kleptomania than in the psychiatric comparison patients and the patients with alcohol abuse or dependence. The Barratt Impulsiveness Scale cognitive impulsivity score was significantly higher in patients with kleptomania, either reflecting a specific thinking process in those patients or a sampling bias because of the high proportion of female subjects in the group with kleptomania. Indeed, cognitive impulsivity scores have been found to be higher and less age-dependent in female subjects
(17), but the gender difference in these scores was not significant in the current study. According to the clinical definition of kleptomania, impulsivity distinguishes patients with the disorder from those with other psychiatric disorders, including alcohol dependence. In addition, the patients with kleptomania and those with alcohol abuse or dependence in this study had higher Sensation Seeking Scale scores than the psychiatric comparison patients. This specific psychopathological profile does not support the inclusion of kleptomania in a general addictive spectrum in which behavioral disturbances (mostly impulse-control disorders) are included. It is interesting to note that the Sensation Seeking Scale disinhibition score of the patients with kleptomania was significantly higher than that of the psychiatric comparison patients and was comparable to that of the patients with alcohol abuse or dependence. The items that make up the disinhibition measure are related mainly to substance use and abuse, and the patients with kleptomania in this study did not have a high rate of major substance-related disorders. Even though their responses on this measure suggested a tendency for substance abuse, they apparently could control that tendency, although they failed to control other socially discredited behavior.
Finally, no obsessive-compulsive spectrum disorders were found in the patients with kleptomania, except for one subject. This finding is in keeping with the conclusion of the family study by Bienvenu et al.
(6), which did not support the inclusion of impulse-control disorders in the obsessive-compulsive spectrum.
In conclusion, kleptomania presented a specific psychopathological profile that distinguished it both from substance abuse and dependence and from other (non-substance-related and non-impulse-control) psychiatric disorders. Impulsivity remains the major psychopathological feature of kleptomania. The link between kleptomania and affective disorder is supported by the high comorbidity rates of mood disorders reported in three previous studies and in most reports of single cases. In addition, a specific pattern of variation in disorders over time in which the pathological behavior of kleptomania increases or decreases after changes in mood has been described in several cases
(11,
23). The retrospective method used here is strongly limited, but the pattern of alternating disorders was found in about half of the patients with kleptomania in this study. This specific relationship should be confirmed in further prospective studies. Because patients with kleptomania share severe psychopathology and have a low rate of comorbid major substance-related disorders, insights about the information processes and the psychobiology underlying impulsivity may be gained from studies involving them.