The aim of this study was to systematically ascertain the views of mental health service users and staff in England about the use of coercive measures during acute psychiatric hospitalizations. It has been found that coerced admission to hospitals is not associated with subsequent adherence to treatment ( 1 ), but the focus of this study was on coercion after admission to an acute psychiatric unit.
It is widely accepted that effective inpatient care sometimes includes the deployment of coercive measures, such as seclusion and restraint, by staff to contain dangerous or severely disruptive behavior by a service user. Extensive efforts have been made in Europe and the United States over the past decade to systematically assess rates of coercive measures ( 2, 3, 4 ) and to reduce them ( 5 ). D'Orio and colleagues ( 6 ), for example, found a 39% reduction in coercion after implementing a comprehensive plan that included the availability of a response team with enhanced verbal deescalation skills.
Involvement in the use of these measures or witnessing their use can be highly distressing for both service users and staff ( 7, 8, 9 ), and few are likely to remain neutral about them. Little is known about the attitudes or preferences of staff or service users regarding different types of coercive measures. Such preferences are likely to have some influence on the decision to deploy certain coercive measures and thus are worthy of the systematic investigation reported in this article.
Much research on subjective perceptions in this area has been qualitative and focused on emotional responses to the experience of coercion ( 10 ). Qualitative studies conducted outside of the United Kingdom and United States have indicated that many of the responses of service users and staff are recognizable across cultures—for example, fear and anxiety ( 11, 12 ). More structured approaches are increasingly being developed to survey the attitudes of staff and service users ( 13, 14 ), and they have revealed intriguing patterns that may vary across cultures—for example, in a study of 30 Chinese inpatients, most viewed physical restraint in a positive light when staff provided psychological and informational support to patients throughout the procedure ( 15 ); however, many other studies in Europe and North America report highly negative views toward physical restraint ( 10 ).
However, instruments that survey the attitudes of staff and service users and qualitative studies do not enable direct comparison of different types of coercive measures, which was the aim of this study. Two U.S. studies did allow such comparisons and found that staff in a high-security psychiatric hospital ( 16 ) and in a neuropsychiatric facility ( 17 ) ranked the following measures in the same order of preference: medication, seclusion, and mechanical restraint. However, no distinction was drawn in these studies between consensual PRN (as needed) medication and coerced intramuscular (IM) medication, even though these are clearly two very different scenarios.
A Canadian study ( 18 ) compared staff and service user preferences in a small, purposive sample and found a number of patterns—for example, service users approved of PRN medication much more than staff did. However, the questionnaire used presented the methods hierarchically, making interpretation of relative preferences difficult. Bowers and colleagues ( 19 ) reported the development of a new tool, the Attitudes to Containment Measures Questionnaire (ACMQ), which enables direct comparison of coercive measures. Coerced medication is explicitly identified to distinguish it from consensual medication in this instrument. Preliminary data from student nurses in four countries suggest that students in England had greater reservations about coercive measures, compared with their counterparts in the Netherlands and Finland ( 20 ).
The aim of the study reported here was to move beyond previous research by eliciting service user and staff preferences and approval ratings for various coercive measures used in inpatient care. ACMQ scores were used to compare the approval ratings of staff and service users. A large national sample was used, which provides a benchmark against which other national samples can be compared. A cross-sectional survey design was adopted.
Methods
Setting and sample
Study participants were staff and service users who were drawn from the 136 acute wards participating in the City 128 study ( 21 ). The intention was to recruit ten service users and all staff from each ward. Service users on each ward who were potential participants were identified by random sampling, but once identified, only those judged by staff as able to grant informed consent and participate were approached. After complete description of the study to service users who were potential participants, written informed consent was obtained. Most service users were interviewed by a research assistant to aid completion of the ACMQ instrument. All staff members on each ward were sent a copy of the ACMQ instrument, and those who completed it returned it anonymously through an internal mailbox.
Measure
The ACMQ ( 19 ) lists 11 coercive measures used widely in inpatient care either in the United Kingdom (consensual PRN medication, compulsory IM medication, physical restraint, intermittent observation, constant observation, time out, transfer to a psychiatric intensive care unit (PICU), locked-door seclusion, and open-area seclusion) or elsewhere in Europe (mechanical restraint and use of a net bed, defined as a lockable metal frame with side netting bolted to a bed [4,22]). Each listed coercive measure is accompanied by a short description and a visual illustration, and then six dimensions of approval for each measure are assessed: effectiveness, acceptability, respectfulness, safety for service users, safety for staff, willingness to undergo (asked of service users) or to use (asked of staff). The respondent is asked to indicate his or her degree of approval on a 5-point Likert scale (ranging from strongly agree, 5, to strongly disagree, 1) and then is asked to indicate (yes or no) whether he or she has been involved in implementing the measure (asked of staff) or been subjected to it (asked of service users). Responses were summed across approval ratings for each coercive measure. Possible scores range from 6 to 30, with higher scores indicating higher levels of approval. Comparisons between groups were tested with independent samples t tests, chi square analysis, or Spearman correlations.
The study was approved by the National Health Service North West Multicentre Research Ethics Committee.
Results
The final sample consisted of 1,226 staff and 1,361 service users ( Table 1 ). Ninety-five percent of the staff members who responded were nurses (N=834, 68%) or health care assistants (N=331, 27%), and the rest were from other occupations—occupational therapist (N=3, <1%), psychiatrist (N=3, <1%), psychologist (N=2, <1%), social worker (N=1, <1%), and other groups (N=52, 4%). Data were collected in 2004 and 2005.
Table 1 Characteristics of acute psychiatric inpatients and staff members in England who were surveyed about coercive interventions
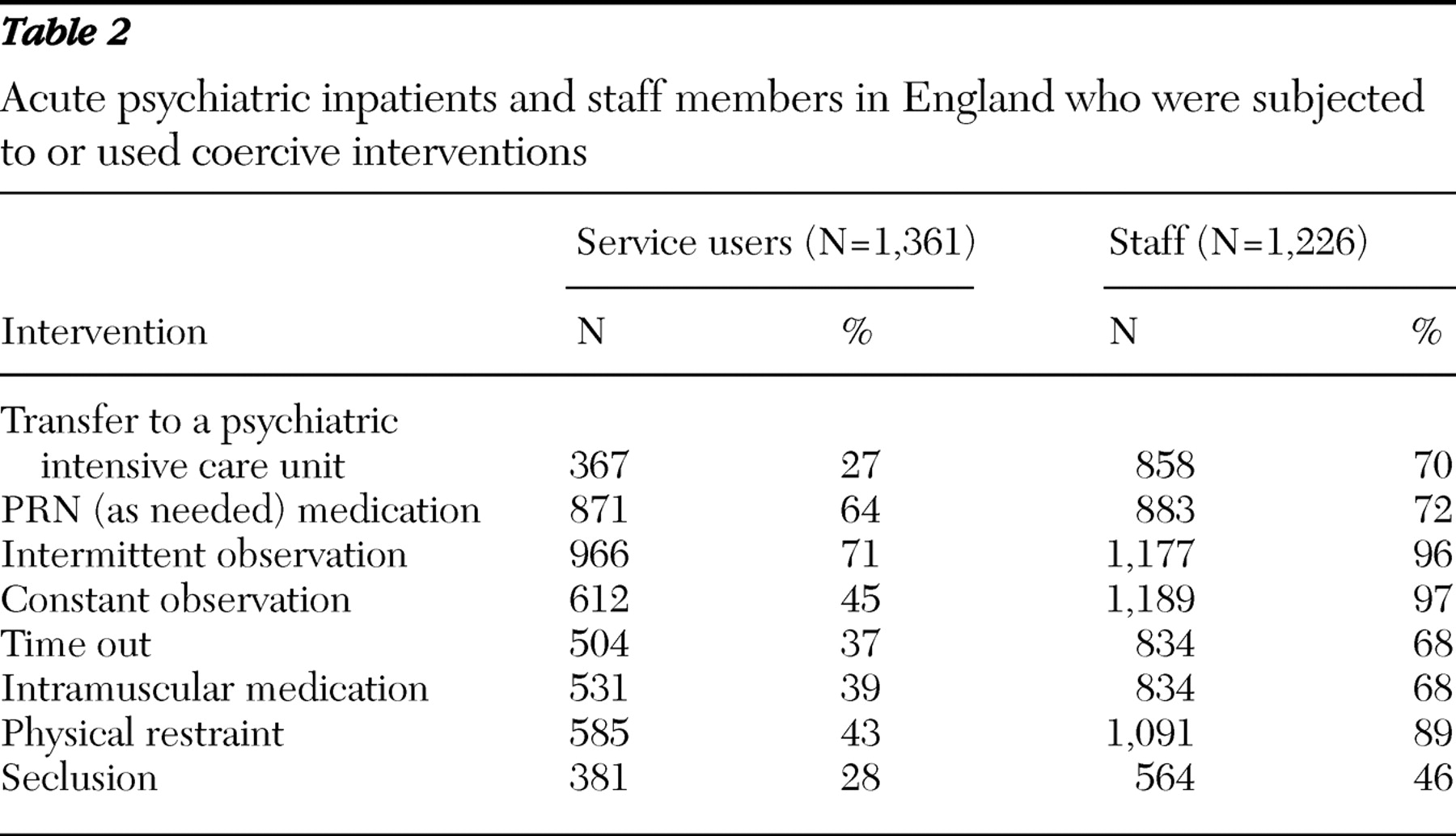
For the coercive methods in use in the United Kingdom, service users were asked whether they had been subjected to them and staff were asked whether they had used them. A summary of responses to these items is presented in Table 2 . As might be expected, compared with service users, staff had greater experience with coercive methods, because staff have a constant presence in the acute ward, whereas individual service users tend to be in the acute ward for a relatively short time.
Table 2 Acute psychiatric inpatients and staff members in England who were subjected to or used coercive interventions
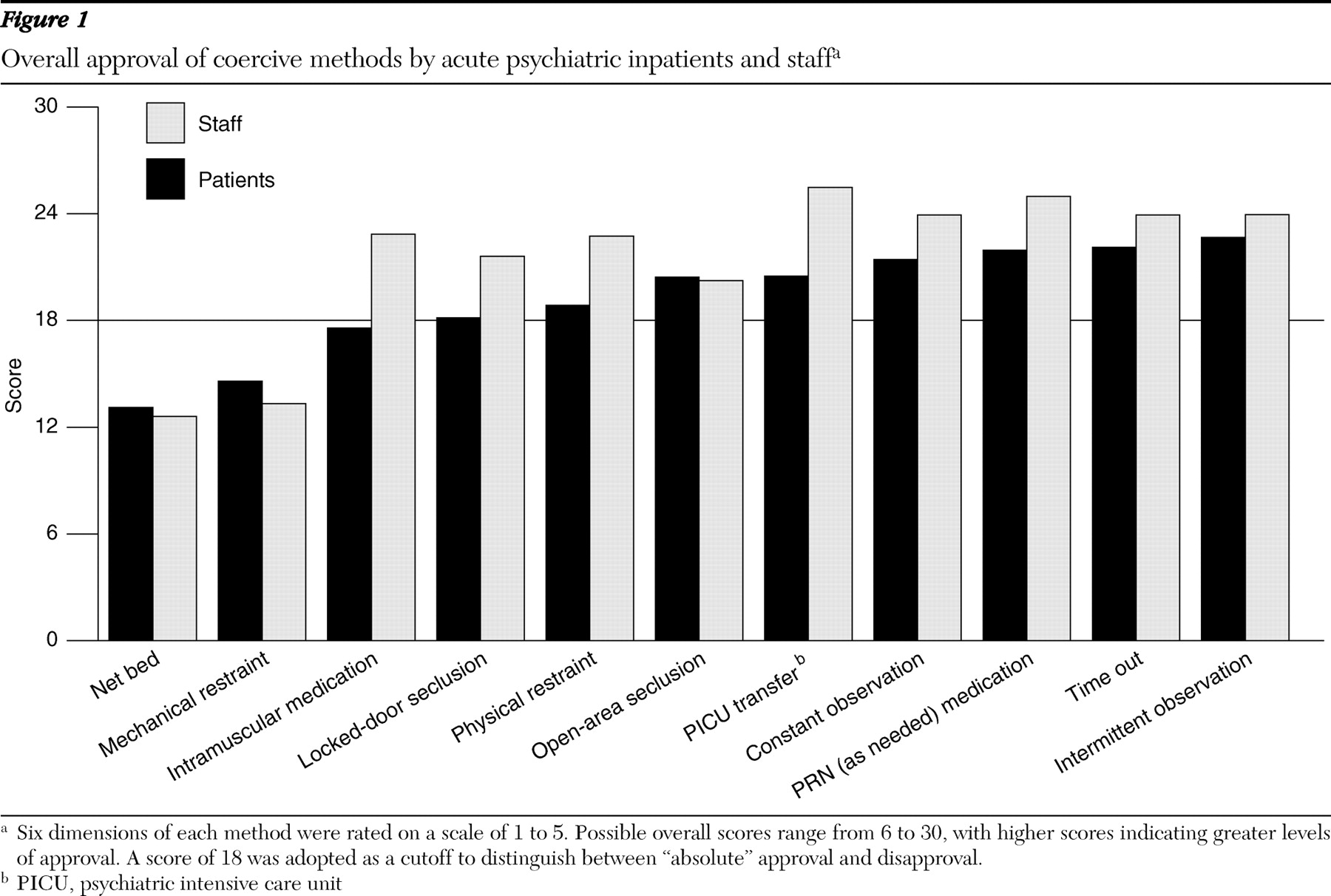
Figure 1 plots the sum total approval score for each group for comparison purposes. It can be seen that the three methods that service users most disapproved of were net beds, mechanical restraint, and IM medication; the three methods that staff most disapproved of were net beds, mechanical restraint, and open-area seclusion. The three methods that the service user group most approved of were intermittent observation, time out, and PRN medication; the staff group most approved of PICU transfer, PRN medication, and observation. As shown in Figure 1, a score of 18 was adopted as a cutoff to distinguish between "absolute" approval and disapproval, because this value lay at the midpoint of the modified Likert scale. Using this cutoff, the study showed that both service users and staff disapproved of net beds and mechanical restraint and service users also disapproved of IM medication.
Figure 1 Overall approval of coercive methods by acute psychiatric inpatients and staff
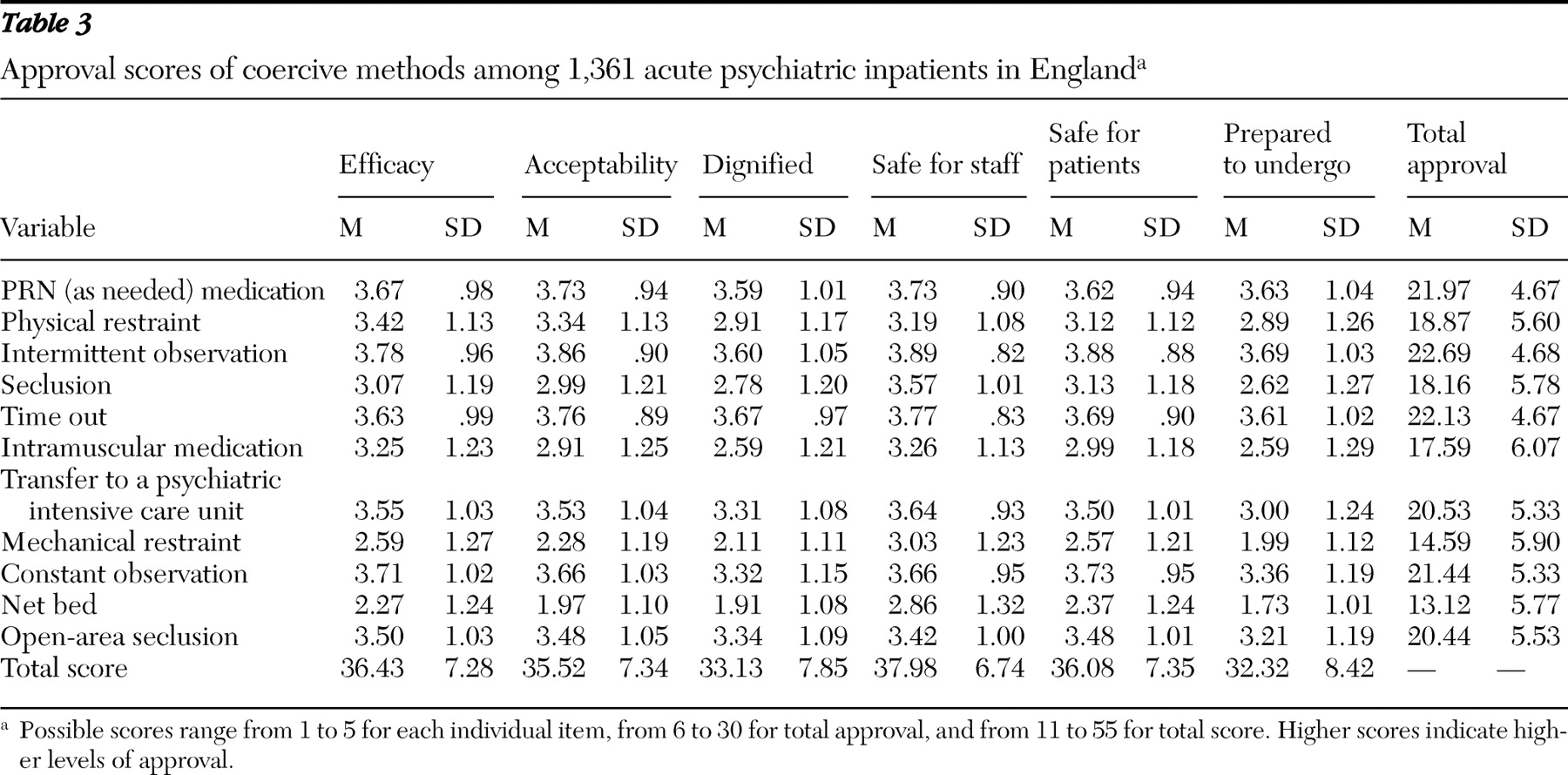
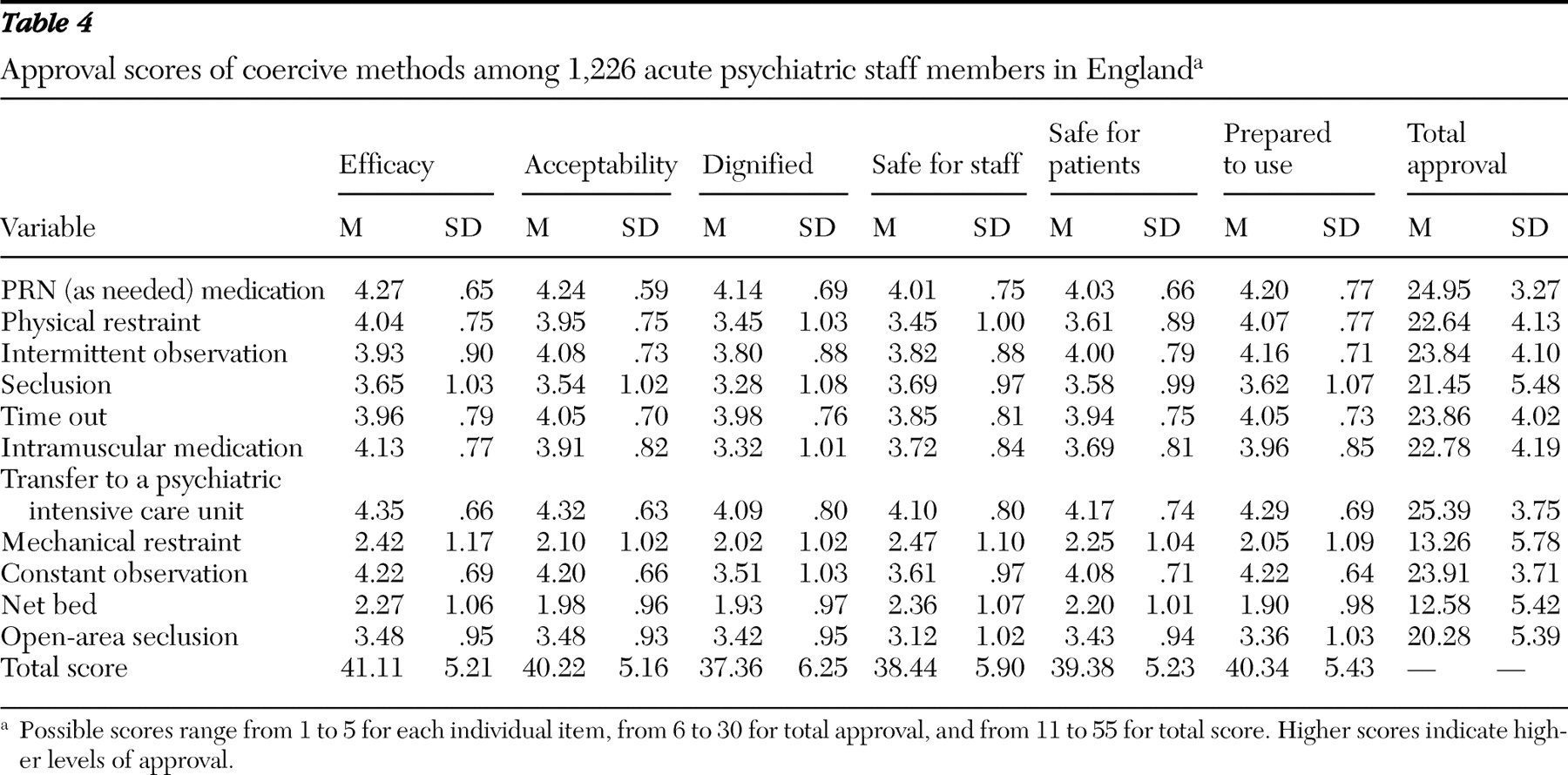
Tables 3 and 4 present the mean±SD scores for service users and staff on each of the six dimensions of approval with regard to the 11 coercive measures. Overall, compared with service users, staff had higher levels of approval on each dimension, although both groups had approximately equal levels of approval for the dimension "safe for staff." Service users and staff strongly disapproved of most aspects of net beds, and it is noteworthy that there was a relatively strong endorsement of the item "I would not be prepared to undergo mechanical restraint" by the service user group.
Table 3 Approval scores of coercive methods among 1,361 acute psychiatric inpatients in England
Table 4 Approval scores of coercive methods among 1,226 acute psychiatric staff members in England
Variations by gender
Service users. Approval ratings by male service users were consistently significantly higher than those by female service users for manual restraint (t=2.26, df=1,339, p=.024), seclusion (t=2.42, df=1,330, p=.016), mechanical restraint (t=3.16, df=1,318, p=.002), and net beds (t=3.79, df=1,308, p<.001). Female service users were more likely than male service users to have been subjected to intermittent observation ( χ2 =10.81, df=1, p=.001) and constant observation ( χ2 =4.81, df=1, p=.028), whereas male service users were more likely than female service users to have been subjected to seclusion ( χ2 =5.48, df=1, p=.019) and psychiatric intensive care ( χ2 =21.21, df=1, p<.001). [Tables showing the mean± SD scores for service users and staff, by gender, with regard to the 11 coercive measures are available as an online supplement at ps.psychiatryonline.org .]
Staff. There were also multiple differences within the staff group by gender. Compared with female staff, male staff consistently had higher levels of approval of every coercive method except for time out, psychiatric intensive care, and IM medication (PRN medication, t=2.14, df=1,153, p=.03; manual restraint, t=3.01, df=1,159, p=.003; intermittent observation, t=2.5, df=1,157, p=.013; seclusion, t=3.97, df=1,0791, p<.001; mechanical restraint, t=4.14, df=1,080, p<.001; constant observation, t=2.08, df=1,150, p=.038; net beds, t=2.6, df=1,033, p=.009; and open area seclusion, t=3.05, df=1,077, p=.002). Male staff were more likely than female staff to have used seclusion ( χ2 =9.17, df=1, p=.002).
Variations by age
Service users. There was a positive relationship to age for most coercive methods, with older service users expressing greater approval of many coercive methods (manual restraint, r=.123, p<.001; seclusion, r=.083, p=.002; IM medication, r=.127, p=.077; PICU transfer, N=1,333, r=.072, p=.008; constant observation, r=.105, p<.001). Younger service users were more likely than older service users to have been subjected to physical restraint ( χ2 =11.67, df=5, p=.04), time out ( χ2 =20.44, df=5, p=.001), and constant observation ( χ2 =11.67, df=5, p=.04). [Tables showing the mean± SD scores for service users and staff, by age, with regard to the 11 coercive measures are available as an online supplement at ps.psychiatryonline.org .]
Staff. Younger staff were significantly more approving than older staff of mechanical restraint (r=-.175, p<.001) and net beds (r=-.117, p<.001). There were relationships between staff age and their experience of having used some coercive measures, but these relationships were not straightforward or in each case the same. Younger and older staff used some coercive measures more frequently than middle-aged staff, but for other measures middle-aged staff (30–49 years) had used the coercive measure more frequently than the other two age groups. For staff, therefore, there is probably an interaction between age, duration of time working in psychiatry, and training period (that is, someone trained in the 1990s might have been exposed to a different set of attitudes during training than someone trained in the 1980s).
Variations according to personal experience
Service users. With regard to overall approval score, service users who had been subjected to PRN medication (t=6.29, df=1,342, p<.001) and constant observation (t=2.78, df=1,327, p=.005) approved of these measures more strongly than service users who had not been subjected to these measures. Those who had been subjected to manual restraint (t=7.44, df=1,344, p<.001) and compulsory IM medication (t=7.08, df=1,332, p<.001) disapproved of these measures more strongly than service users who had not been subjected to these measures. [Tables showing the number of service users who experienced the 11 coercive measures and staff who used them are available as an online supplement at ps.psychiatryonline.org .]
Staff. There was a universal tendency for staff who had used a specific coercion measure to approve of it more strongly than staff who had not—for example, PRN medication (t=6.63, df=1,139, p<.001) and manual restraint (t=6.13, df=1,161, p<.001). Sample sizes for physical restraint and intermittent observation were highly unbalanced, because only some staff (85% to 90%) had ever been involved in implementing these procedures.
Discussion
Overall, this study established a robust set of benchmark values with regard to how mental health service users and staff in England view various coercive measures that are commonly used in inpatient care. These benchmark values can be used as a platform for further work in which the views of staff in other hospitals in the United Kingdom and in other countries can be compared. The values could also be used in pre-post evaluation studies, in which attitudinal change is considered desirable, and could be combined with data from structured assessments of perceived coercion at the time of admission ( 1 ).
This sample covering three regions of England is larger and more representative than the sample that was previously surveyed with the ACMQ—that is, a sample of approximately 100 student nurses at one university ( 19 ). Nevertheless it is worth noting that the relative order of approval of coercive methods from the students was slightly different than the order for the staff we surveyed in this study. Among the student nurses, PRN medication was the coercive method with the highest approval rating (whereas staff in our sample gave PICU transfer their highest approval rating), and student nurses had higher approval ratings of open-area seclusion, compared with staff in our study. The students' ranking of methods and their overall approval scores were closer to those of the service users than to the staff members in our study.
The Canadian staff in a high-security hospital that was studied by Harris and colleagues ( 18 ) had the greatest preference rating for seclusion combined with manual restraint, as compared with other methods (time out and PRN medication), in stark contrast to the English staff in an acute care hospital in this study, who rated them relatively poorly. This difference may be in part due to the different settings of the two studies. However, equal proportions of Canadian staff and Canadian service users disapproved of mechanical restraint, which matched findings in our study. And there is agreement between staff in the United States and staff in our study in that mechanical restraint was the most disapproved coercive method.
Some significant findings in this study are worth highlighting. Evidence was found of strong disapproval among both staff and service users with regard to the introduction of mechanical restraint. Attitudes toward other measures did not differ substantially between the two groups, although service users tended to be more disapproving overall than staff. The staff responses varied according to age, with older staff tending to disapprove more strongly of coercive measures. The age effect, in which younger staff were less disapproving of mechanical restraint, may reflect a generation change in which "old-fashioned" prejudices against an apparently legitimate technique are being shed or may result from a lack of exposure to concrete examples of use in the real world.
There was greater approval among men of coercive methods (whether they were staff or service users), a finding that confirms results from a previous international study that used the same instrument ( 20 ). This indicates the importance of gender roles, perceptions, and identity in this area. The United Kingdom is fairly unique in having a psychiatric nursing workforce that is composed of approximately equal amounts of men and women. The gender effect could reflect any of a large number of more general hypothesized gender-related differences (for example, empathy and emotional intelligence). It could be that a nursing workforce that is more dominated by women would result in less coercive practice. However, in other countries where female nursing staff predominate, harsher coercive measures are implemented by male security guards or by male nursing aides with no formal professional qualification ( 23 ), ultimately resulting in much higher levels of use.
Personal experience was associated with some heterogeneity in attitudes in the service user group. There appeared to be a tendency for exposure to "gentler" measures (for example, observation) to enhance approval ratings and, conversely, for exposure to "harsher" measures (for example, IM medication) to lead to stronger rejection of the measure. Staff had a consistent tendency to approve of techniques once they had employed them in their practice, which may reflect a process of attitudinal adjustment in which persons justify the measure to themselves afterward to avoid unpleasant feelings of cognitive dissonance ( 24 ).
Various study limitations must be acknowledged. The sample was large and representative of the three regions (although not necessarily of elsewhere in England), but staff involvement in the selection of service users could have introduced bias. Because of time constraints when assembling the large sample, it was not possible to assess potentially important covariates, such as service user diagnosis, type of unit, or rates of assault in the unit. In addition, the analysis presupposes the notion of a stable attitude toward a coercive measure, which is consistent across situations. However, it is possible that such attitudes are more fluid and that specific incidents will require different types of intervention at different times. Further testing of the instrument, especially in relation to test-retest reliability, would be beneficial.
Conclusions
Mental health service users and staff both strongly disapproved of the use of any form of mechanical restraint, although that disapproval was slightly stronger among staff. This result suggests that any endeavor to introduce the use of mechanical restraint into adult acute psychiatry in the United Kingdom is likely to be met with significant opposition. From the pattern of results we can also predict that if mechanical restraint were introduced to the United Kingdom, staff who used it would approve of it more, and service users who were subjected to it would dislike it even more, leading to a harmful schism between service users and staff.
The greater approval of coercive methods by male staff—and in the case of the harsher methods, their greater involvement in the use of them—raises questions about gender roles within psychiatric nursing. More attention to this aspect of psychiatric care and the issues around it during nurses' training might be necessary.
For service users the most acceptable coercive measure was intermittent observation, followed by time out and PRN medication. Ward regimens that use these methods rather than others are likely to be better received by service users. The least acceptable methods to service users (excluding those not in use in the United Kingdom) were manual restraint, locked-door seclusion, and coerced IM medication. For these methods, disapproval increased with experience, and their use should therefore be avoided as much as possible.
Acknowledgments and disclosures
This study was funded by the Service Delivery and Organisation Research and Development Programme, Department of Health, England.
The authors report no competing interests.
Footnote
Dr. Whittington is affiliated with the School of Health Sciences, University of Liverpool, Thompson Yates Bldg., the Quadrangle, Liverpool L69 3GB, United Kingdom (e-mail: [email protected]). Dr. Bowers and Dr. Simpson are with the Department of Mental Health and Learning Disability, City University, London. Dr. Nolan is with the School of Health, Staffordshire University, Stafford, United Kingdom. At the time of the study, Dr. Neil was with the School of Health Sciences, University of Liverpool, Liverpool, United Kingdom.
References
1.
Rain SD, Williams VF, Robbins PC, et al: Perceived coercion at hospital admission and adherence to mental health treatment after discharge. Psychiatric Services 54:103–105, 2003
Steinert T, Martin V, Baur M, et al: Diagnosis-related frequencies of compulsory measures in ten German psychiatric hospitals and correlates with hospital characteristics. Social Psychiatry and Psychiatric Epidemiology 42:140–145, 2007
Donat DC: Special section on seclusion and restraint: encouraging alternatives to seclusion, restraint, and reliance on PRN drugs in a public psychiatric hospital. Psychiatric Services 56:1105–1108, 2005
Whittington R, Baskind E, Paterson B: Coercive measures in the management of imminent violence: restraint, seclusion and enhanced observation, in Violence in Mental Health Settings: Causes, Consequences, Management. Edited by Richter D, Whittington R. New York, Springer Verlag, 2006
Huckshorn K: Reducing seclusion restraint in mental health use settings: core strategies for prevention. Journal of Psychosocial Nursing and Mental Health Services 42(9): 22–33, 2004
D'Orio BM, Purselle D, Stevens D, et al: Reduction of episodes of seclusion and restraint in a psychiatric emergency service. Psychiatric Services 55:581–583, 2004
Lind M, Kaltiala-Heino R, Suominen T, et al: Nurses' ethical perceptions about coercion. Journal of Psychiatric and Mental Health Nursing 11:379–385, 2004
Bonner G, Lowe T, Rawcliffe D, et al: Trauma for all: a pilot study of the subjective experience of physical restraint for mental health inpatients and staff in the UK. Journal of Psychiatric and Mental Health Nursing 9:465–473, 2002
Duxbury J: An evaluation of staff and patient views of strategies employed to manage inpatient aggression and violence on one mental health unit: a pluralistic design. Journal of Psychiatric and Mental Health Nursing 9:325–337, 2002
Chien WT, Chan C, Lam L, et al: Psychiatric inpatients' perceptions of positive and negative aspects of physical restraint. Patient Education and Counseling 59:80–86, 2005
Terpstra TL, Terpstra TL, Pettee EJ, et al: Nursing staff's attitudes toward seclusion and restraint. Journal of Psychosocial Nursing and Mental Health Services 39:20–28, 2001
Harris G, Rice M, Preston D: Staff and patient perceptions of the least restrictive alternatives for the short-term control of disturbed behaviour. Journal of Psychiatry and Law 17:239–263, 1989
Bowers L, Alexander J, Simpson A, et al: Cultures of psychiatry and the professional socialization process: the case of containment methods for disturbed patients. Nurse Education Today 24:435–442, 2004
Bowers L, van der Werf B, Vokkolainen A, et al: International variation in attitudes to containment measures for disturbed psychiatric inpatients. International Journal of Nursing Studies 44:357–364, 2007
Bowers L, Whittington R, Nolan P, et al: The City 128 Study of Observation and Outcomes on Acute Psychiatric Wards: Report to the NHS SDO Programme. London, City University, 2006
Morrison E, Morman G, Bonner G, et al: Reducing staff injuries and violence in a forensic psychiatric setting. Archives of Psychiatric Nursing 16:108–117, 2002
Harmon-Jones E, Mills J (eds): Cognitive Dissonance: Progress on a Pivotal Theory in Social Psychology. Washington, DC, American Psychological Association, 1999