A rapid-cycling course
(1,
2), with at least four major affective episodes in a year, is included in DSM-IV as a diagnostic specifier for the criteria for bipolar manic-depressive disorders. Rapid cycling appears to be a diagnostically reliable phenomenon
(3-
5), is particularly common among patients with type II bipolar disorders, is associated with high rates of morbidity with potentially severe disability, and may predict an unsatisfactory response to lithium maintenance treatment
(6-
10). The reported incidence of rapid-cycling patients among persons with bipolar disorders is about 15%, although this rate may be somewhat inflated because of sampling from specialized mood disorders clinics where such difficult patients may be overrepresented
(1-
10).
It is widely accepted that women with a bipolar disorder are at particularly high risk of rapid cycling
(6,
7). Women have accounted for 72.6% (range=58%–92%) of rapid-cycling bipolar patients (9, 10). However, these rates do not necessarily represent the sex-specific risk of a rapid-cycling course, since clinical samples may contain dissimilar proportions of women and men at risk. In an attempt to clarify this remaining uncertainty, we evaluated the relative risk of rapid cycling in women and men with a bipolar disorder.
RESULTS
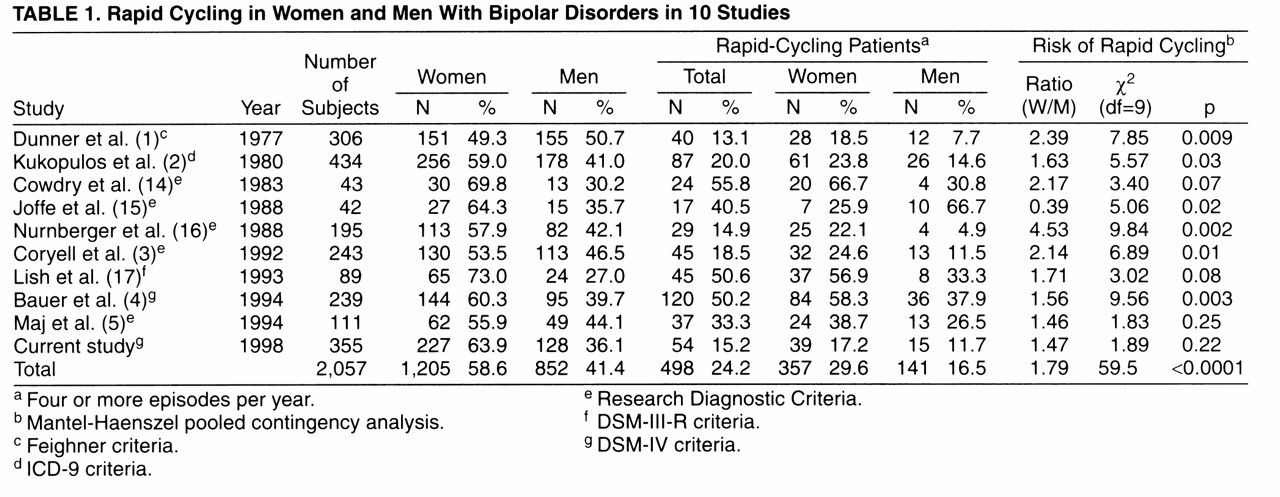
A total of 10 studies (1-5, 14-17) with 2,057 bipolar disorder patients provided suitable data (
table 1). There were more female subjects than male subjects, with no evidence of sex bias in case selection. A rapid-cycling course was found in 24.2% of the patients, but this rate was probably inflated by selection of rapid-cycling cases in some studies
(4,
14,
15,
17) that had unusually high proportions of such cases (40.5%–55.8%). Women and men, respectively, represented 71.7% (357/498) and 28.3% (141/498) of rapid-cycling cases (a 2.53-fold difference), but rapid cycling occurred in only 29.6% of women and 16.6% of men. This 1.78-fold difference was statistically highly significant when all available data were pooled. However, significant sex differences in the risk of a rapid-cycling course were found in only six of the 10 studies (
table 1), and there was highly significant inconsistency of results across studies (for lack of homogeneity, χ
2=40.2, df=9, p<0.0001).
Among our own unselected bipolar subjects, 15.2% had rapid cycling. The cycling rate (episodes per year) before maintenance treatment was 2.52 times higher among the 54 rapid-cycling patients (mean=3.85, SD=3.78) than among the 301 non-rapid-cycling patients (mean=1.53, SD=1.61) (t=7.42, df=353, p<0.0001). The rapid-cycling patients also had a 2.17 times higher average cycling rate during lithium maintenance treatment (mean=1.38, SD=1.99, versus mean=0.63, SD=0.70; t=4.54, df=353, p<0.001). However, there was little difference in cycling rates between the 15 rapid-cycling men and the 39 rapid-cycling women before lithium maintenance treatment (mean=4.94, SD=4.58, and mean=3.41, SD=3.38, respectively; t=1.33, df=52, n.s.) or during lithium maintenance treatment (mean=1.21, SD=2.37, and mean=1.45, SD=1.85, respectively; t=0.39, df=52, n.s.).
DISCUSSION
This analysis included all of the studies we found that had data permitting computation of rates of rapid cycling in bipolar women and bipolar men. It was limited by variance in patient selection and diagnoses and possible underreporting of rapid-cycling men, given a widespread impression that rapid cycling is much more common in women
(1-
10). More women than men (2.53-fold) were found among the rapid-cycling bipolar patients. However, the sex difference favoring women was inconsistent (six of 10 studies) and more moderate (1.79-fold) than suggested by analyses based on the frequency of women and men among rapid-cycling bipolar patients
(1-
10). Moreover, cycling rates (average number of episodes per year) were similar in rapid-cycling men and women both before and during lithium maintenance treatment.
Evidently, estimates of risk based on the proportion of women among rapid-cycling patients can be misleading, perhaps because of sampling factors, including possible overrepresentation of women among patients treated for major mood disorders. Although the reported sex ratio of risk for bipolar disorders is close to 1.0
(7,
18), women may more often seek and accept treatment for major mood disorders, including lithium for bipolar disorders
(7) and antidepressants for nonbipolar major depression
(19). In turn, some of the risk for rapid cycling in women may reflect excessive use of antidepressants without adequate mood-stabilizing treatment
(2,
4,
7,
20). In conclusion, the present findings indicate that rapid cycling in bipolar disorders occurs in both men and women, with somewhat greater risk in women, but at similar cycling rates before and during lithium maintenance treatment in both sexes.