Category of Substance of Abuse
The patients with substance-related disorder and dysthymia and patients with substance-related disorder only did not differ at statistically significant levels in their axis I abuse or dependence diagnoses for the following substances of abuse: alcohol (74% versus 78%) (χ2=0.12, df=1, p=0.73), opioids (8% versus 21%) (χ2=2.88, df=1, p=0.09), cocaine (8% versus 15%) (χ2=1.05, df=1, p=0.30), amphetamines (8% versus 10%) (χ2=0.06, df=1, p=0.81), sedatives (8% versus 7%) (χ2=0.00, df=1, p=1.00), or hallucinogens (0% versus 3%) (p=0.61, Fisher’s exact test). The two groups did differ significantly with regard to cannabis abuse/dependence, with the patients with substance-related disorder and dysthymia abusing less of this substance (10% versus 38%) (χ2=10.75, df=1, p<0.001).
Type of substance being abused did not affect the treatment and cost data between patients with substance-related disorder and dysthymia and patients with substance-related disorder only.
Substance-Related Treatment History
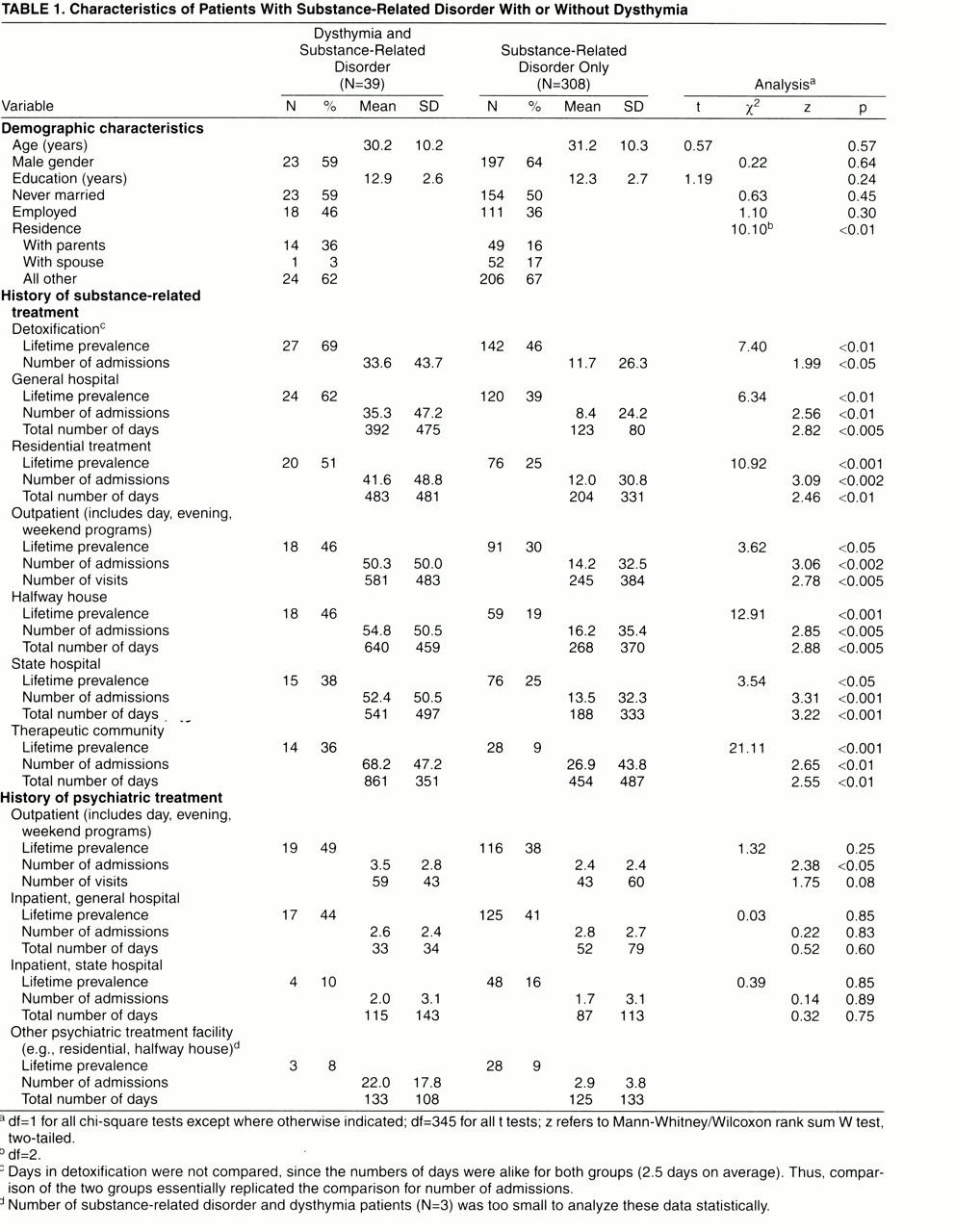
Data were obtained on history of treatment for substance-related disorder before the current treatment (
table 1). Of the 20 variables related to locus of treatment, 17 showed significant differences between the patient groups, with patients with substance-related disorder and dysthymia receiving significantly more care. Those treatments showing significant differences included the following.
1. Greater lifetime history was present for five categories of treatment setting (i.e., detoxification, general hospital substance-related disorder unit, residential substance-related disorder treatment, substance-related disorder halfway house, and substance-related disorder therapeutic community).
2. Number of admissions to the program type in previous lifetime was greater for six treatment settings; only number of detoxification admissions were not significantly different.
3. Total number of days in all seven treatment settings was greater for patients with substance-related disorder and dysthymia.
The average length of stay (i.e., dividing the total number of days by the number of admissions) was shorter for the group with substance-related disorder and dysthymia in five of the six treatment methods (excluding detoxification, which was identical for both groups). However, none of the differences was statistically significant, according to nonparametric testing.
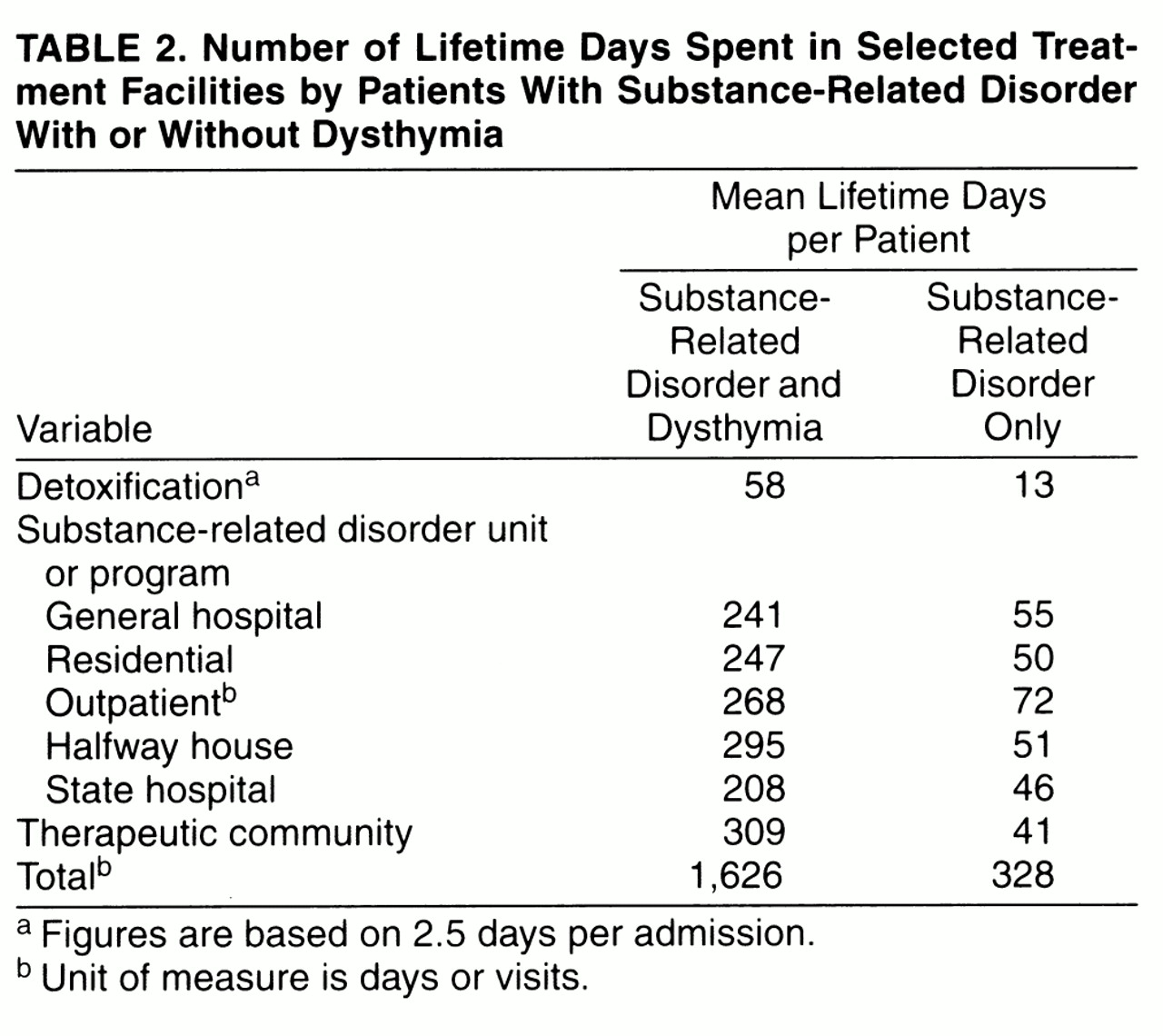
The number of lifetime days per facility was spread over the entire group for purposes of comparison. Although the number of total days is only an average, it does provide another quantitative means of comparing the resources used by both groups, as shown in
table 2.
Some patients were in more than one type of program at one time. An example would be attendance at a day program while living in a halfway house. Thus, the total number of days was slightly less than the total number of days spent per patient in treatment. The patients with substance-related disorder and dysthymia had appreciably more treatment days in all seven categories; they had spent about 4.5 years in treatment. The patients with substance-related disorder only had spent an average of 0.9 years in treatment. In sum, the patients with substance-related disorder and dysthymia spent five times as many days in treatment for substance-related disorder as the patients with substance-related disorder only.
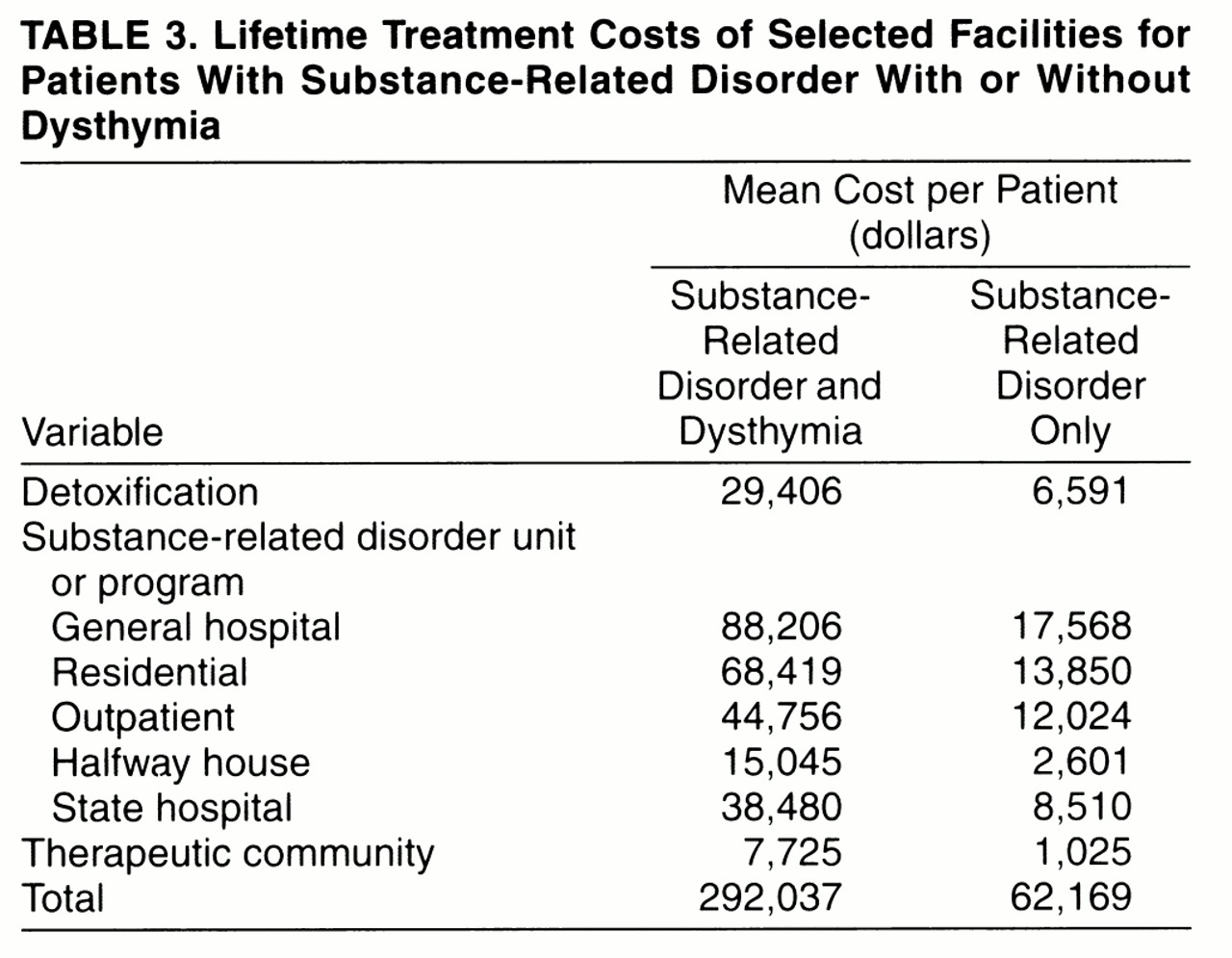
We estimated the cost of lifetime treatment by using the daily estimates described in the Method section. Lifetime treatment costs (excluding the current treatment episode) for the entire two groups (i.e., averaged across all patients in both groups) are shown in
table 3. The lifetime cost of treatment for substance-related disorder was 4.7 times higher for patients with substance-related disorder and dysthymia than for patients with substance-related disorder only.
Substance-Related-Disorder Self-Help Activities
On their own, many patients had attempted to reduce their psychoactive substance use. The two groups did not differ in regard to any of seven self-help activities: i.e., joining a self-help group (62% of 39 patients with substance-related disorder and dysthymia versus 48% of 308 patients with substance-related disorder only), reducing frequency of use (60% versus 58%), reducing dose or amount used per time (59% versus 57%), changing type of psychoactive substance (46% versus 44%), changing friends (37% versus 40%), changing residence (17% versus 31%), and changing job or school (16% versus 17%).