Professional firefighters are often exposed to traumatic stress by helping other people in emergency situations. Traumatic stress can be caused by exposure to severely mutilated bodies, the impact of life-threatening situations, physically demanding activities, and great material destruction. In many cases, these experiences induce various psychological and physiological stress reactions, which may lead to physical complaints (
1), mental disorders, and substance abuse (
2). Occupational stress in emergency missions can induce an acute or posttraumatic stress disorder (PTSD) (
3).
According to DSM-IV, the essential feature of PTSD is the development of characteristic symptoms following exposure to an extremely traumatic stressor. PTSD symptoms are divided into three categories: reexperiencing of the trauma, avoidance of trauma-related stimuli, and increased emotional arousal. PTSD should be diagnosed if the symptoms persist for at least 1 month. If the symptoms remit within 4 weeks after the traumatic event, the diagnosis of an acute stress disorder is indicated.
The persistence of PTSD symptoms may lead to decreased job satisfaction, work absenteeism, or early retirement (
4). Depending on the type of exposure to trauma, either directly as a victim or indirectly as a helper, PTSD is classified as a primary or secondary traumatic stress disorder, respectively (
5). In contrast to primary stress symptoms, which are directly related to the experience of primary traumatic stress as a victim, secondary stress can be defined “as the natural consequent behaviors and emotions resulting from knowing about a traumatizing event experienced by a significant other—the stress resulting from helping or wanting to help a traumatized or suffering person” (
5).
A number of epidemiological studies of trauma and PTSD in several populations have been undertaken (for a review see Green [
6]). Kilpatrick and Resnick (
7) found current prevalence rates for PTSD of 12% from sexual assault and 13% from rape. Current prevalence rates for Vietnam combat veterans were shown to be 15% (
2). This selection of studies represents research on victim-oriented PTSD, in other words, primary traumatic stress disorder.
Although there is a growing interest in the consequences of occupational stress in emergency services personnel, empirical studies have rarely been performed until now. McFarlane (
8) found prevalence rates of 32%, 27%, and 30% in a sample of firefighters 4, 11, and 29 months after an Australian bushfire. About 20% of these firefighters had perceived the situation as life-threatening, 41% had to protect themselves from the fire, 23% suffered from property damage, and 25% were injured (
9). It can be stated that the firefighters in this study were personally affected by the disaster, i.e., they were mainly victims, not only helpers. This group also showed a high risk of PTSD, which was due mainly to the bushfire mission and less to helping other people in the emergency. Research on the effects of disasters has, again, usually focused on the immediate victim of the traumatic event (
10), particularly on primary traumatic stress disorder.
There have been only a few studies aimed at the psychological consequences of traumatic emergency missions (
11) and the prevalence of secondary stress disorder. About 24% of rescue workers involved in an oil rig disaster showed posttraumatic stress reactions 9 months after the disaster (
12). Prevalence rates of PTSD in rescue workers have been estimated to range from 3% to 7% (
13,
14). Studies of populations at a high risk of PTSD, e.g., firefighters, emergency workers, or policemen, may provide much-needed information about the prevalence of secondary PTSD, but they have not been carried out thus far. Such epidemiological data represent the basis for further research related to conditions and consequences of secondary PTSD. For this reason we focused on a population of professional firefighters in the State of Rheinland-Pfalz, Germany. This group is repeatedly exposed to secondary traumatic stress that qualifies as trauma beyond normal human experience. Therefore, the present study intended to examine the prevalence of primary and particularly secondary traumatic stress disorder in a representative group of German firefighters who do not share the experience of a common disaster. Furthermore, the study attempted to ascertain the comorbid symptoms of PTSD in firefighters and to identify variables that appear to increase the extent of PTSD symptoms among firefighters.
METHOD
Participants
In contrast to auxiliary firefighters, professional firefighters can be seen as a homogeneous group that shares a similar frequency and intensity of call-out alarms. Therefore, only professional male firefighters (N=574) were recruited to participate in the study. The function of professional fire departments includes different tasks, such as command and control-centered head office, mission duty, mission control duty, emergency medical service, and administration. About 90% of the firefighters were engaged in mission duty, 18% in mission control duty, 15% in command and control-centered head office, 7% in administration, 11% in emergency medical service, and 32% in multiple functions. The overall questionnaire response rate was 70% (N=402). The mean age of the firefighters was 39.68 years (SD=9.68); their average job experience amounted to 15.80 years (SD=9.66). There was no significant mean age difference between the total number of firefighters in Rheinland-Pfalz (39.66 years) and those firefighters who participated in this study. Thus, the 402 responders constitute a representative group of all professional firefighters in the state. Written informed consent was obtained by forms attached to the questionnaire package.
Questionnaire
The applied questionnaire included demographic items, such as job experience, field of activity, and number of distressing missions in the last month; a German version of the General Health Questionnaire (
15); a German version of the PTSD Symptom Scale (
16); the “openness” subscale of a personality inventory, called the Freiburger Persönlichkeitsinventar (
17); the substance use subscale of a stress coping questionnaire, called the Streßverarbeitungsfragebogen (
18); and a self-rating list of bodily complaints, the Freiburger Beschwerdeliste (
19).
The General Health Questionnaire is a screening questionnaire aimed at detecting persons with a diagnosable psychiatric disorder (
15). This questionnaire, a widely used scale in general practice studies of physical illness and distress, includes four subscales: somatic symptoms, anxiety/insomnia, social dysfunction, and severe depression. In the present study the General Health Questionnaire scoring method (0-0-1-1) was applied so that one point was given for each affirmative answer. A total score above the proposed threshold score of 4/5 (4=low score, 5=high score) indicates the presence of a psychiatric disorder (
15). The General Health Questionnaire has been recommended for screening and interviewing trauma victims (
20). The PTSD Symptom Scale is an instrument to assess the presence and severity of PTSD symptoms through use of a 4-point scale. The items on the PTSD Symptom Scale are clustered into reexperiencing (five items), avoidance (seven items), and arousal (five items) symptoms, according to DSM-IV criteria. PTSD is diagnosed if at least one reexperiencing, three avoidance, and two arousal symptoms are endorsed on the scale by firefighters who were traumatized at least 1 month before the examination. In this study, a symptom was rated as present if the PTSD Symptom Scale item corresponding to the symptom was scored one or greater. Subsyndromal PTSD can be diagnosed if the reexperiencing symptom cluster, plus either the avoidance or the arousal cluster, is visible (
21). Furthermore, the 12-item openness subscale of the Freiburger Persönlichkeitsinventar is used as a control deceit test to assess social desirability. Individuals with a low score on this scale show a high level of social desirability. The substance use subscale of the stress coping questionnaire is applied to assess the extent of substance abuse in comparison to the general population. The six items on this scale include items on smoking, drinking, and the use of medication, such as tranquilizers or sedatives. The list of bodily complaints consists of 78 items with 11 subscales that are related to relevant sets of bodily complaints: general condition, emotional reactivity, cardiovascular symptoms, gastrointestinal symptoms, head-neck syndrome, tension, sensory, pain, motor problems, skin, and a subscale that provides a total score for bodily complaints.
Procedure
In February 1997, we distributed the questionnaire to all professional firefighters on duty. The firefighters were able to return the completed questionnaires to locked ballot boxes that were placed in the fire departments in order to ensure personal anonymity. All completed questionnaires were collected after 4 weeks. This 4-week period was necessary to account for irregular changes of shift and holidays.
Data Analysis
Firefighters who scored below a standardized and age-related threshold for social desirability were excluded from further analysis in order to control the influence of social desirability. To underpin this procedure, we compared the mean scores on the General Health Questionnaire, PTSD Symptom Scale, stress coping questionnaire, and list of bodily complaints between firefighters with high and low levels of social desirability; we used analysis of variance (ANOVA) with social desirability introduced as the covariate. Firefighters with a high level of social desirability could be excluded from further analysis if the mean difference could be explained by the introduction of the covariate. Only firefighters who met the criteria for PTSD assessed by the PTSD Symptom Scale and who scored above the General Health Questionnaire threshold were classified as persons suffering from posttraumatic stress symptoms. To compare the prevalence of PTSD symptoms in different fields of professional activity, we used chi-square tests. In addition, we tested the number of firefighters with PTSD symptoms related to the different types of duties.
The comorbidity of PTSD symptoms with depressive mood or social dysfunction could be ascertained if the relevant General Health Questionnaire subscales were scored one or greater. Substance abuse and bodily complaints were estimated by comparing the scores on the stress coping questionnaire and list of bodily complaints with a well-defined German norm sample. Differences in mean scores on the General Health Questionnaire, PTSD Symptom Scale, stress coping questionnaire, and list of bodily complaints among firefighters with PTSD symptoms, subsyndromal PTSD, mental disorders, or psychiatric impairment, on the one hand, and psychologically healthy firefighters, on the other hand, were tested by ANOVA. Paired group differences were calculated with Bonferroni post hoc tests. To determine which variables might explain traumatic stress and the degree of psychiatric impairment, we used linear regression analysis with scores on the PTSD Symptom Scale and General Health Questionnaire as dependent variables and age and number of distressing missions in the last month as independent variables. To assess the influence of traumatic stress on bodily complaints, substance abuse, and psychiatric morbidity, we computed series of linear regression analysis with scores on the General Health Questionnaire, stress coping questionnaire, and list of bodily complaints as dependent variables and scores on the PTSD Symptom Scale as independent variables.
RESULTS
A high level of social desirability was assessed in 22.9% of the firefighters. We found significant mean differences between firefighters with and without social desirability in scores on the PTSD Symptom Scale, stress coping questionnaire, and list of bodily complaints. We found no significant differences in mean scores on these scales between these groups, as the covariate social desirability was introduced in this analysis. Therefore, the firefighters with a high level of social desirability were excluded from further analysis.
Of the remaining 318 subjects, 78 (24.5%) met the full criteria for acute or posttraumatic stress disorder assessed by the PTSD Symptom Scale; scale scores ranged from 8 to 38, with a mean of 17.8 (SD=6.7). Further analysis showed that 58 firefighters (18.2%) scored above the General Health Questionnaire threshold, while 20 (6.3%) displayed no psychiatric impairment on this measure. Only those firefighters who met diagnostic criteria for PTSD and who were detected as persons with mental disorders were classified as firefighters with PTSD symptoms (N=58, 18.2%). Both groups showed significant mean differences in the extent of traumatic stress calculated with Bonferroni post hoc tests. In addition, 46.2% (N=147) of the firefighters met criteria for subsyndromal PTSD.
Furthermore, 86 subjects (27.0%) were screened as individuals with mental disorders, as assessed by the General Health Questionnaire. The General Health Questionnaire total score ranged from 5 to 21; the mean was 8.72 (SD=3.58). About 81% (N=70) of these individuals showed subsyndromal PTSD symptoms in addition to psychiatric impairment. The remaining 154 firefighters (48.4%) displayed no psychiatric symptoms, but a large subgroup of 76 (49.4%) still met criteria for subsyndromal PTSD.
Of the firefighters who worked in mission duty, the percentages of those with (89.7%) and without (90.5%) PTSD symptoms were not significantly different (χ2=0.03, df=1, p=0.87). We also found no significant differences between firefighters with and without PTSD symptoms working in command and control-centered head office (17.9% versus 13.9%), administration (6.9% versus 7.6%), mission control duty (19.2% versus 17.6%), and emergency medical service (8.6% versus 10.7%). Thus, there were no significant mean differences in PTSD Symptom Scale scores among firefighters working in different professional functions.
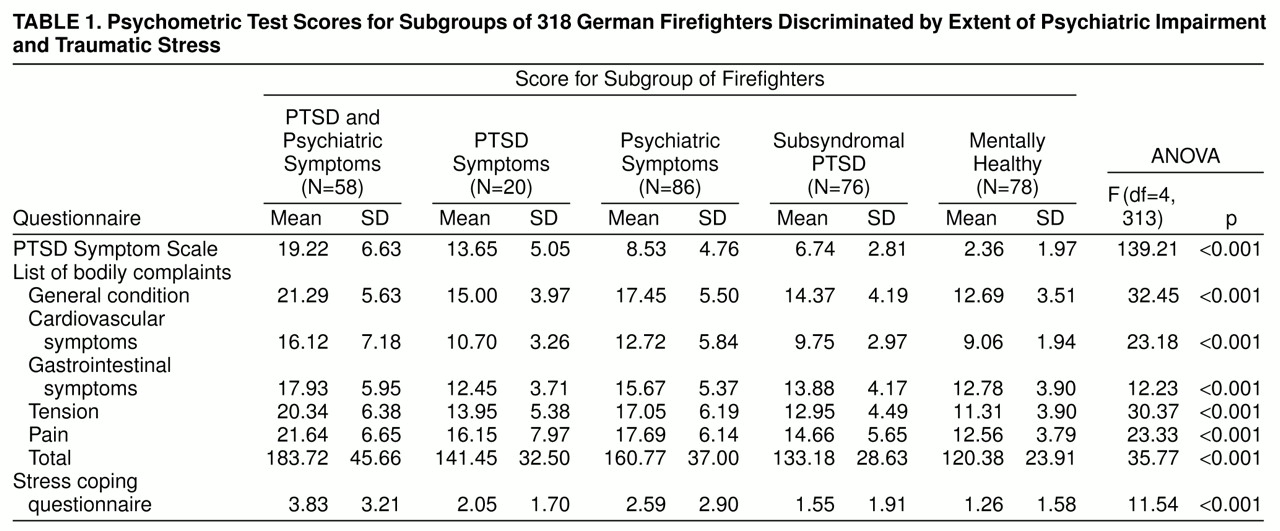
An analysis of the comorbidity of PTSD with other psychiatric dysfunctions showed that 39.7% of firefighters with PTSD symptoms (N=23) suffered from depressive mood, 60.3% (N=35) displayed social dysfunction, and 19.0% (N=11) were substance abusers. In comparison to the general population, firefighters with PTSD symptoms expressed a higher amount of cardiovascular complaints and had more tension, pain, and motor problems (
table 1). Compared with other subgroups, firefighters with PTSD symptoms showed a significantly higher level of traumatic stress, substance use, and bodily complaints, especially on the subscales of general condition, cardiovascular symptoms, tension, pain, and total score (calculated with Bonferroni post hoc tests). Furthermore, firefighters with psychiatric symptoms had significantly higher scores than their mentally healthy colleagues on all tested scales (again calculated with Bonferroni post hoc tests).
Regression analysis with the PTSD Symptom Scale score as the dependent variable showed that job experience and the number of distressing missions during the last month were significant predictors of the extent of traumatic stress in firefighters (F=40.16, df=2, 312, p<0.001). These variables explained 20.47% of the variance on the PTSD Symptom Scale and 10.47% of the variance on the General Health Questionnaire (F=18.24, df=2, 312, p<0.001).
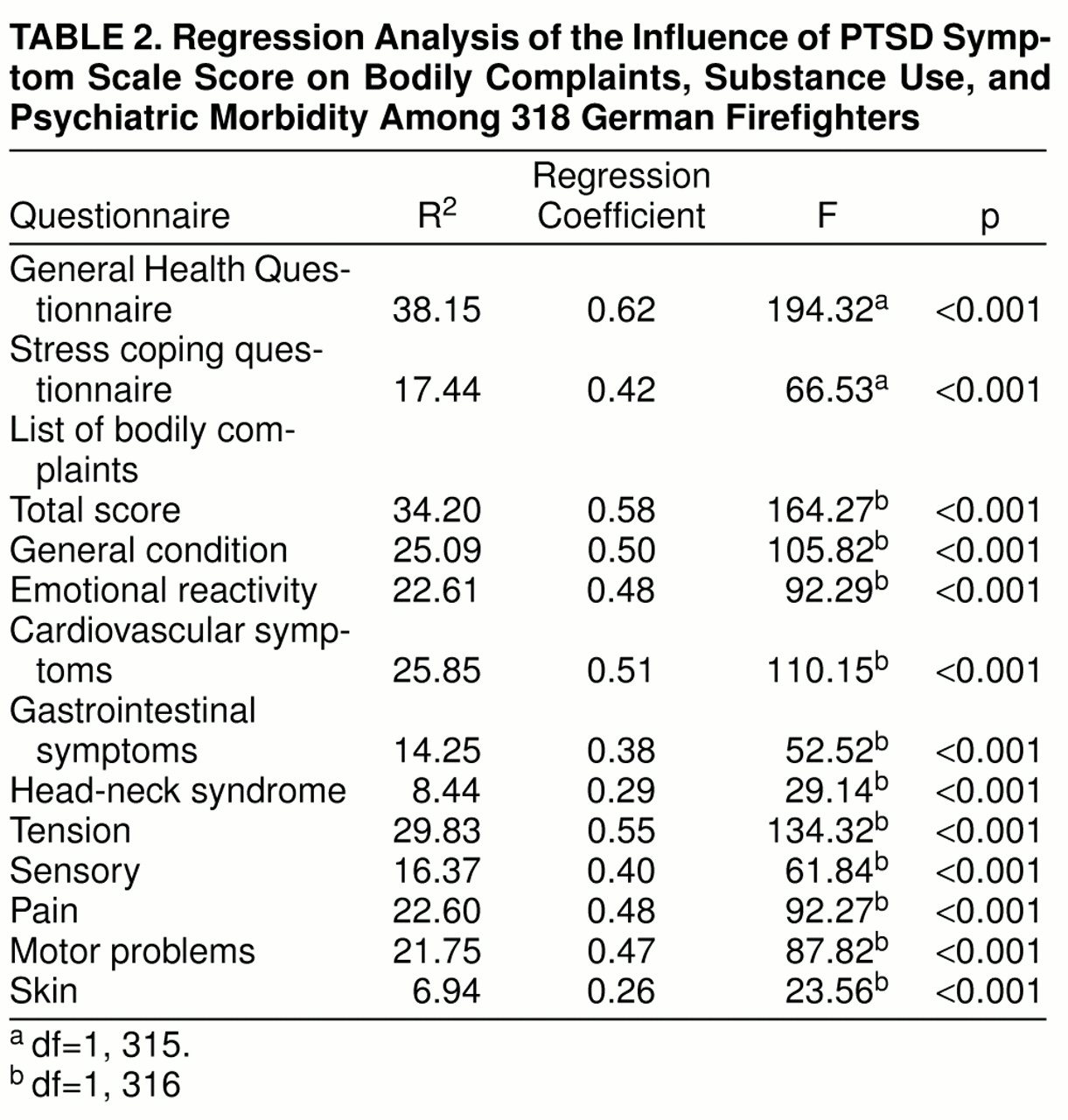
Table 2 displays the influence of traumatic stress on psychiatric impairment. The extent of traumatic stress assessed by the PTSD Symptom Scale explained 38.15% of the variance on the General Health Questionnaire total score. In other words, the exposure to a traumatic event and the characteristic stress reactions are relevant for the genesis of psychiatric symptoms. Furthermore, the PTSD Symptom Scale score explained 34.20% of bodily complaints, 20.40% of severe depression, and 17.44% of substance use.
DISCUSSION
This study examined the prevalence of PTSD symptoms, mental disorders, and substance abuse in a representative population of professional firefighters in Germany. It was intended to investigate the health status of a population at high risk for developing PTSD independent of specific common missions or traumata. We also proposed to examine the influence of job experience and number of distressing missions on the extent of traumatic stress. Firefighters are exposed to two different risk factors for PTSD. They experience life-threatening situations and are confronted with grief, death, and mutilated bodies during emergency missions. Both extremely distressing conditions can be described as potentially PTSD-inducing traumata. PTSD research studies have tended to focus on primary traumatic stress disorder, while neglecting symptoms associated with secondary traumatic stress as experienced by emergency workers such as firefighters (
5). This study was designed to pay more attention to the consequences of distressing missions in those people who try to save the lives of victims in an emergency situation. To our knowledge, this is the first study of a population at high risk for PTSD as a result of daily work. The representative group of German professional firefighters under investigation did not share a specific common traumatic event, but all participants were exposed to different missions all over the State of Rheinland-Pfalz. The main difference between our study and previous studies is our emphasis on the secondary traumatic stress disorder. Survey self-reports of 2,000 professional firefighters and paramedics indicated that about 90% were actually confronted at least once with distressing missions including dead, dying, or severely injured persons within the past year (
22).
On the basis of this representative group of 318 German professional firefighters, we found a current prevalence rate of 18.2% for PTSD symptoms. This rate is lower than the one reported by McFarlane (
8), who studied firefighters who shared firsthand the experience of a severe traumatic event, a great Australian bushfire. The prevalence of PTSD symptoms found in the present study was related to the regular daily duty of different representative fire departments. Estimates of the prevalence of PTSD in rescue workers (
13,
14) seem to underestimate posttraumatic stress reactions as a result of daily routines. In addition, we found a high prevalence of comorbid psychiatric symptoms, such as depressive mood, social dysfunction, and substance abuse. These findings are in line with several studies related to PTSD (
2,
23–
26). Furthermore, 6.3% of the firefighters showed a characteristic number and intensity of PTSD symptoms but were free from psychiatric symptoms.
In contrast, 27.0% of the participants reported psychiatric symptoms. These firefighters showed recurring and more intense bodily complaints than the general population, especially those related to general condition, cardiovascular complaints, tension, and pain. These results correspond with findings that predict elevated blood pressure during work under perceived high job strain (
27). Most of these firefighters met criteria for subsyndromal PTSD symptoms.
How can the high prevalence of PTSD symptoms and psychiatric impairment in German professional firefighters be explained? Firefighters work in heterogeneous functions, such as emergency medical service and mission duty, where they are exposed to different kinds of stressors. However, there was no evidence of differences in the degree of traumatic stress for firefighters working in distinct functions. Traumatic stress was also not related to combinations of different types of duties. Thus, the development of PTSD symptoms does not seem to depend on specific functions within a fire department. As long as firefighters maintain an active-duty status, they continue to be constantly exposed to trauma-associated stimuli. A traumatized firefighter is not able to avoid those stimuli unless he quits the profession, takes a leave of absence, or transfers to a nonemergency position (
22), like administration or command and control-centered head office.
The most important predictors of PTSD symptoms are the intensity and duration of the exposure to the trauma (
28,
29). In the present study we had no specific information about qualitative aspects of traumata. However, we found that the number of years on duty and the number of distressing missions in the past month were the most valid predictors of the occurrence of PTSD symptoms. The longer a firefighter is on duty and the more often he participates in distressing missions, the higher is the probability of the occurrence of PTSD symptoms. It can be stated that the extent of traumatic stress has clinical relevance for various psychiatric disorders, since the PTSD Symptom Scale score explained a significant amount of variance in bodily complaints, depressive mood, and substance abuse.
To discuss methodological aspects of our study, it is noteworthy that the combination of the General Health Questionnaire and the PTSD Symptom Scale as a screening instrument for PTSD had not been used in the literature previously. In several epidemiological PTSD studies (
11,
30–
32) the General Health Questionnaire and the Impact of Event Scale (
33) were applied to screen for individuals suffering from PTSD. For the detection of diagnosable mental disorders, the General Health Questionnaire represents a widely used, well-validated, and highly reliable screening instrument (
34,
35). Davidson and Fairbank (
36) reported that the General Health Questionnaire is also a useful screening instrument for PTSD. The 28-item version was especially recommended by Raphael et al. (
20). The complete list of symptoms includes reexperiencing, avoidance, and increased emotional arousal. However, the dimension of arousal is not included in the Impact of Event Scale. Therefore, in this study we employed the PTSD Symptom Scale rather than the Impact of Event Scale because it relates precisely to the diagnostic criteria of PTSD as described in DSM-IV. The PTSD Symptom Scale was evaluated by Foa et al. (
16), and a German version was evaluated by Steil (
37). The results of these studies indicated a satisfactory internal consistency, high test-retest reliability, and good concurrent validity of the PTSD Symptom Scale. We were able to confirm the high test quality of the PTSD Symptom Scale with our group of 318 professional firefighters. As a consequence, we used the General Health Questionnaire and the PTSD Symptom Scale to screen for PTSD symptoms and additional psychiatric impairment in professional firefighters. In a follow-up study, we plan to test the specificity and sensitivity of the German version of both questionnaires related to PTSD in comparison with a structured clinical interview.
In summary, our findings suggest that nearly every fifth firefighter reported PTSD symptoms and almost 50% showed further psychiatric symptoms. This fact and the high rate of comorbid symptoms emphasize the need for a more precise consideration of psychological consequences and costs of emergency work. During every workday, firefighters are confronted over and over again with traumatic situations. The lack of adequate strategies to cope with distressing missions and the exposure to traumatic events may facilitate the occurrence of PTSD and other mental disorders, such as major depression, psychosomatic syndromes, and substance abuse. The current findings represent a contribution to a better understanding of the phenomenon of PTSD and underline that more attention needs to be focused on the secondary traumatic stress disorder. The present study investigated only firefighters, but other populations at high risk for PTSD, such as policemen or emergency workers, who are also confronted with traumatic situations during their work, should be examined in future studies. It would also be helpful if the consequences of primary and secondary traumatic stress were part of a larger study in which suicide, divorce, and early retirement due to disability were correlated with the present findings.