On the basis of these observations, we conducted a three-center, randomized, placebo-controlled study to assess the efficacy of the SSRI fluvoxamine during a 9-week course of treatment in 85 outpatients with binge-eating disorder.
METHOD
Study Design
This study was conducted at three sites: Harvard Medical School/McLean Hospital, the University of Cincinnati, and the University of Minnesota. It was a parallel-group, randomized, placebo-controlled, double-blind, flexible-dose study. It began with a 1-week screening period followed by a 1-week single-blind placebo lead-in period. A 9-week treatment period followed. Patients were randomly assigned to therapy with fluvoxamine or placebo. Equal numbers of patients were scheduled to be randomly assigned to receive either drug or placebo. All medications were in identical capsules (50 mg of fluvoxamine or placebo) supplied in numbered containers dispensed to patients according to the randomization schedule. During the placebo lead-in period, patients took one capsule each evening; once a patient entered the double-blind treatment phase, the dose was 50 mg each evening for a minimum of 3 days. Beginning on day 4, the dose could be adjusted on an individual basis between 50 mg and 300 mg until the end of week 9. If the number of capsules was even, an equal number of capsules was taken in the morning and evening; if the number of capsules was odd, the greater number of capsules was taken in the evening. Adjustments within the range of one to six capsules per day were at the discretion of the investigator, and medication was increased within this range until a patient was asymptomatic or intolerance intervened.
Subjects
Subjects were individuals meeting draft DSM-IV criteria proposed in 1991 for binge-eating disorder. In addition, these subjects had reported at their screening visit a history of at least three binge-eating episodes per week for at least 6 months (as opposed to an average of only two episodes per week, as required in the draft criteria). It should be noted that the only change from the draft criteria to those ultimately adopted in DSM-IV was the requirement that the binge eating occur, on average, at least 2 days a week for 6 months. All of the patients reported on here would have met the criterion of 2 days per week as well as that of three episodes per week. For screening purposes and throughout the course of the study, we defined a binge by using the DSM-IV criteria plus the additional requirement that the estimated number of calories consumed be at least 1500 kcal.
Patients were required to be between 18 and 60 years of age and to weigh over 85% of the midpoint of the ideal body weight for their height (
16). Patients were disqualified if they were pregnant or lactating; displayed concurrent anorexia nervosa, concurrent or recent (within 1 year of study entry) major depression or obsessive-compulsive disorder or lifetime substance dependence, psychosis, mania, or organic dementia; posed a significant suicide risk; had received psychotherapy or behavioral therapy within 3 months of entry to the study; had a history of psychosurgery or seizures; had a history of any psychiatric disorder that could interfere with diagnostic assessment, treatment, or compliance; had clinically unstable medical illness; had clinically significant abnormal laboratory results; had received monoamine oxidase inhibitors (MAOIs), tricyclics, neuroleptics, lithium, or fluoxetine within 4 weeks before randomization; had received investigational medications or depot neuroleptics within 3 months before randomization; had previously received fluvoxamine; or had fewer than three binges in the week before randomization (i.e., were considered placebo responders).
Procedures
Patients were seen weekly during the study. At the first visit, the following were obtained, ascertained, or performed: written informed consent; the Structured Clinical Interview for DSM-III-R (SCID) (
17); number of binges during the previous week; medical history; physical examination; vital signs; routine blood chemical and hematological tests; and urinalysis. Patients were given diaries at this and each of the following visits in which to record any binges and, once medication was initiated, the number of capsules of medication taken.
At each subsequent visit, patients were assessed for number of binges experienced since the last visit, medication dose, medication compliance through capsule count, any adverse events, any nonstudy medications, and vital signs. Patients were rated on the Clinical Global Impression (CGI) improvement scale (a 7-point scale on which 1=very much improved, 2=much improved, 3=minimally improved, 4=no change, 5=minimally worse, 6=much worse, and 7=very much worse) and the CGI severity scale (a 7-point scale on which 1=normal, 2=borderline ill, 3=mildly ill, 4=moderately ill, 5=markedly ill, 6=severely ill, and 7=among the most extremely ill patients). The 17-item Hamilton Depression Rating Scale (
18) was administered at the baseline, week 5, and week 9 visits.
Outcome Variables
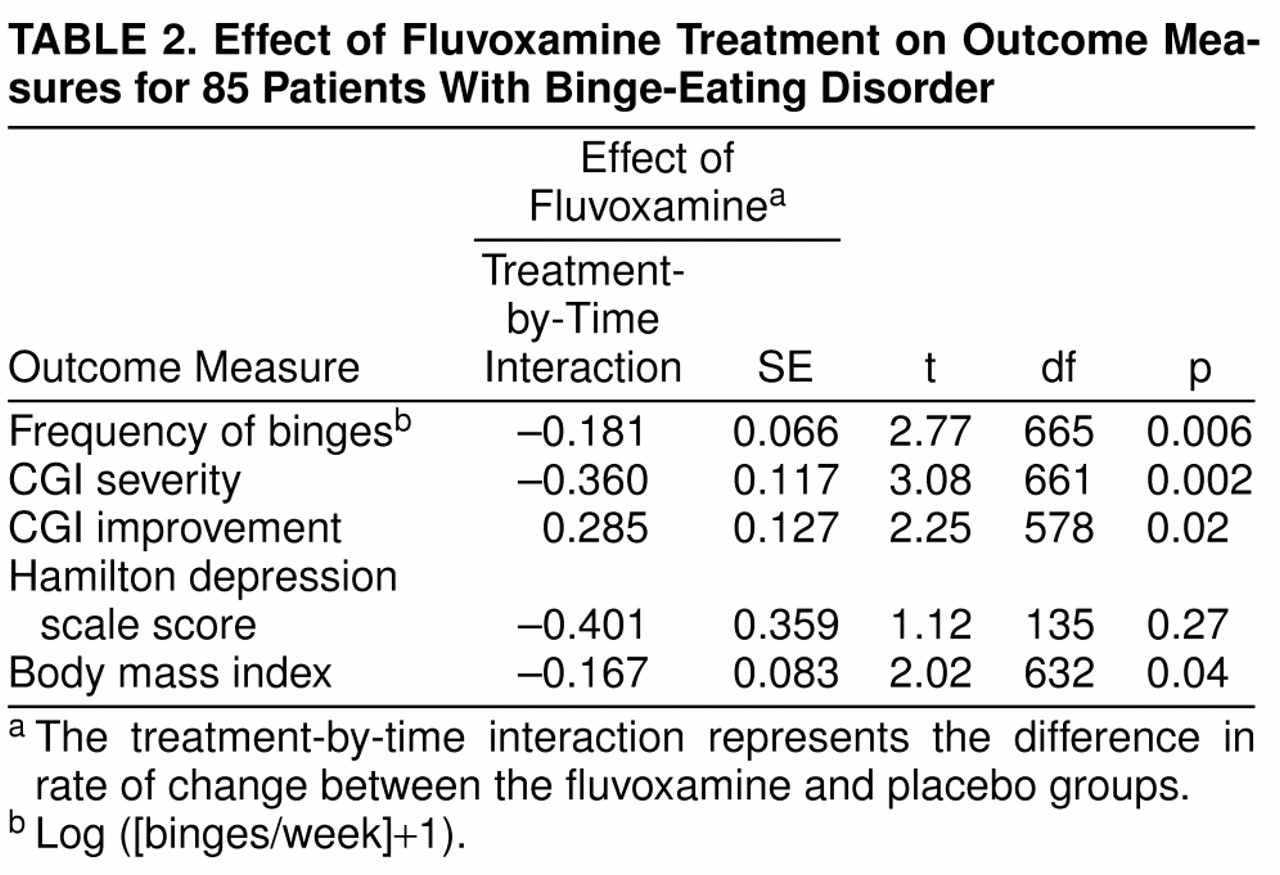
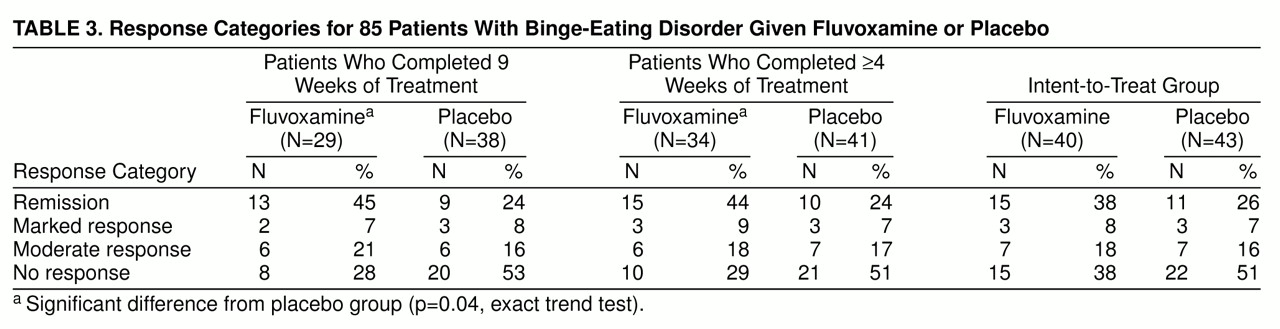
The primary outcome measures were the frequency of binges and CGI scores. Secondary outcome measures were Hamilton depression scale scores, body mass index, and response categories. For the response categories, we classified patients’ responses at endpoint as remission if there was a cessation of binges; marked if the decrease in frequency of binges from baseline was at least 75% but less than 100%; moderate if the decrease in frequency of binges from baseline was at least 50% but less than 75%; and none if the decrease in frequency of binges from baseline was less than 50%.
We also assessed the following safety measures: adverse experiences, clinical laboratory data, physical examination findings, and vital signs.
Statistical Methods
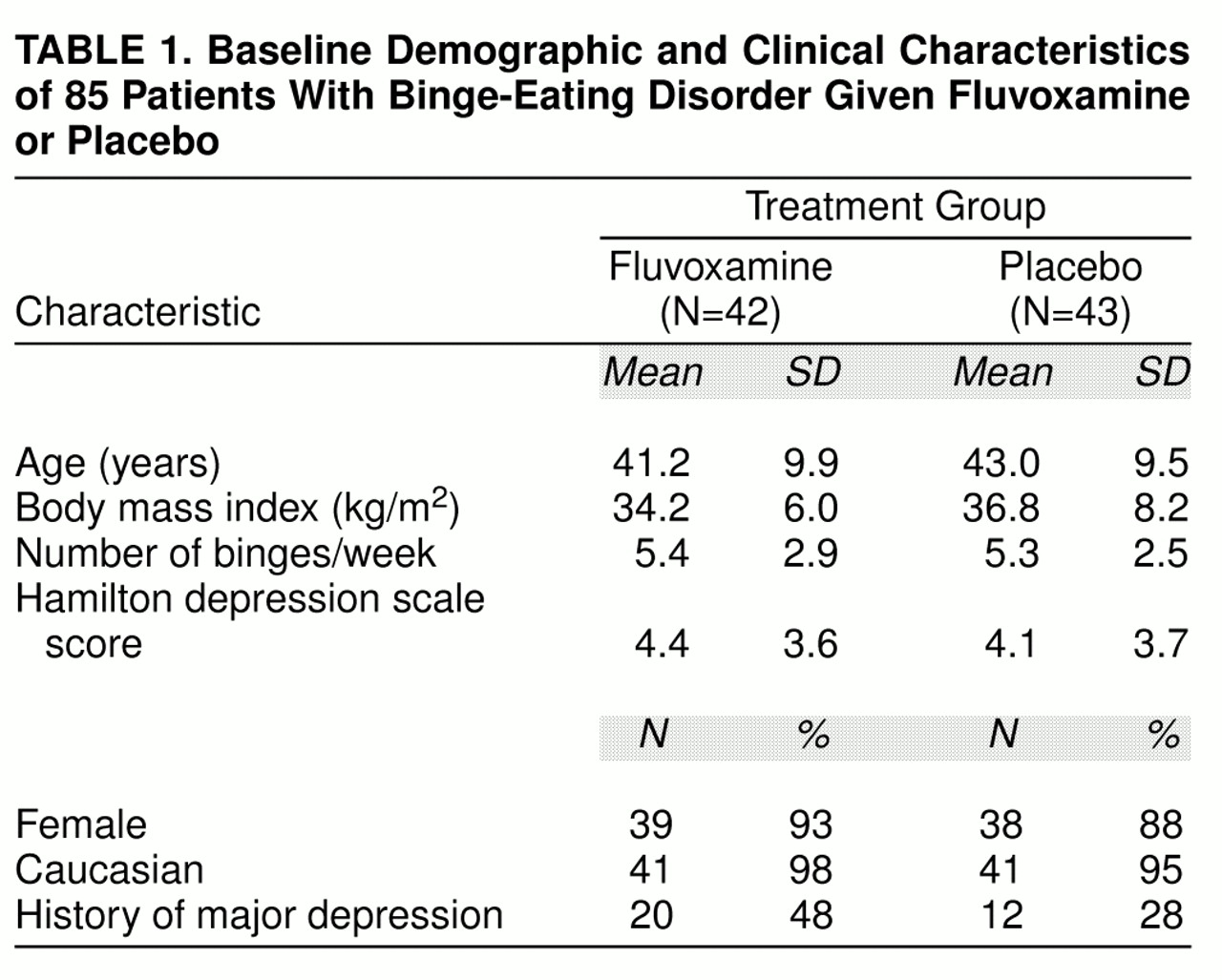
Prestudy comparisons were made by using the following variables at randomization: age, body mass index, binges/week, Hamilton depression scale score, sex, race, and history of major depression. Statistical comparisons were made between patients receiving fluvoxamine and placebo by using Fisher’s exact test for categorical variables and the t test for continuous variables.
For the analysis of each outcome measure (except response category), we used the computer program SAS PROC MIXED (
19) to perform a repeated measures random regression analysis comparing the rate of change of the measure in the fluvoxamine-treated group compared with the placebo group (see Gibbons et al. [
20] and Cnaan et al. [
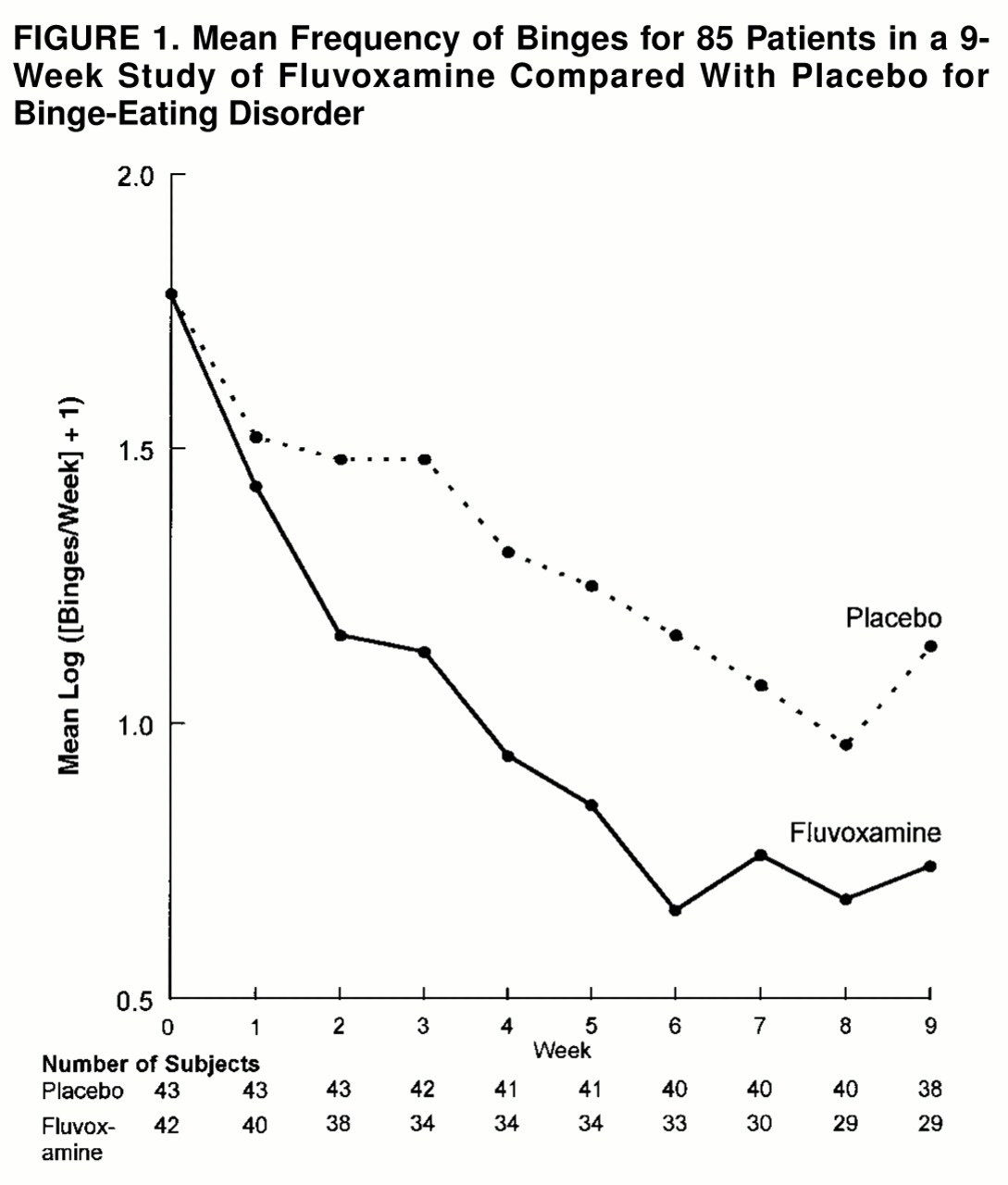
21] for discussions of random regression models to analyze clinical trials in psychiatry). We began with a model for the mean that included terms for treatment, time, center, treatment-by-time interaction, and treatment-by-center interaction. We modeled time as a continuous variable expressed as log (weeks + 1), with week ranging from 0 at baseline to 9 at the visit 9 weeks after randomization. We used the logarithmic transformation because the response of the outcome measures was approximately linear on the log scale, as is often found in treatment studies in psychiatric disorders (
20). For testing, we first checked for a significant treatment-by-center interaction. This interaction was found to be nonsignificant on all measures; therefore, we dropped terms for this interaction from the model. We retained the terms for effects of center in all analyses, regardless of whether the effect of center was significant. The term of interest was the treatment-by-time interaction, which can be interpreted as the difference in the rate of change (change per unit of time), or the difference in slope with respect to time, of the outcome measure.
We initially modeled the covariance of observations on the same individuals as having a heterogeneous first-order autoregressive structure. We then tested whether a simpler model for the covariance structure (compound symmetry or homogeneous first-order autoregressive) was defensible in comparison with the heterogeneous autoregressive structure (using a saturated model for the mean). We chose the most parsimonious model that was defensible. (It emerged that we used the heterogeneous autoregressive structure for analyses of all measures except the Hamilton depression scale, for which we used compound symmetry.)
In view of the observation that the differences between treatment groups at baseline approached statistical significance for history of major depression (see Results), we performed an analysis of covariance on the outcome measures adjusting for this variable. However, because the results of this analysis were almost identical to the unadjusted analysis for each outcome measure, we report only the results of the unadjusted analysis.
For the analysis of frequency of binges, we used the logarithmic transformation (log [(binges/week)+1]) to normalize the data and stabilize the variance.
For response categories, we did not use a repeated measures analysis but, rather, made three comparisons: 1) a completed-subjects analysis, in which we used the final visit assessments for patients who completed the entire 9 weeks of randomized treatment; 2) an evaluable-subjects analysis, in which we used the last assessment on a given subject, provided that the subject completed at least 4 weeks of randomized treatment (we chose 4 weeks as the minimum duration of randomized treatment because studies of fluvoxamine and similarly acting medications have shown that they usually take at least 3 weeks to become effective once they are titrated to an adequate dose); and 3) an intent-to-treat analysis, in which we used the last assessment on all patients who had at least one postbaseline assessment. We compared the difference in categories of response by using the exact trend test for two-by-k ordered tables (Cytel Software Corp., Cambridge, Mass.).
Correlation coefficients were calculated by using rank-transformed data (Spearman rank correlation). All statistical tests were two-sided with alpha=0.05.
DISCUSSION
Fluvoxamine treatment was associated with a significantly greater rate of reduction in the frequency of binges and a significantly greater rate of global improvement than was placebo. In addition, fluvoxamine was associated with a greater rate of reduction in body mass index than was placebo, and weight loss after 9 weeks of treatment was correlated with reduction in frequency of binges. Although fluvoxamine-treated patients were more likely than patients given placebo to withdraw because of adverse medical events, fluvoxamine proved to be safe and usually well tolerated over the 9-week period.
Fluvoxamine was also associated with a significantly higher level of response measured by categories based on percentage changes in binges/week in the analyses of patients who completed 9 weeks of treatment and patients who received at least 4 weeks of randomized treatment. The intent-to-treat analysis also produced findings favoring fluvoxamine but not reaching statistical significance. The failure of the intent-to-treat analysis to reach significance may be explained by the finding that six fluvoxamine-treated patients withdrew before they would have had sufficient time to respond fully. Alternatively, patients taking fluvoxamine who withdrew early might have become discouraged by the absence of beneficial effects and therefore less tolerant of side effects.
The results of this trial with respect to binge eating and overall response are consistent with the findings of previous studies of fluvoxamine, other SSRIs,
d-fenfluramine, and tricyclic antidepressants in binge-eating disorder or similar entities. Small open trials of fluvoxamine (
15) and paroxetine (
14) have reported beneficial effects in obese binge eaters (
15) and patients with binge-eating disorder (
14). Stunkard and colleagues (
8) found that the rate of binge eating decreased three times more rapidly in patients given
d-fenfluramine than those given placebo in a study of 28 severely overweight women with binge-eating disorder. McCann and Agras (
9), in a study of 23 patients with DSM-III-R nonpurging bulimia nervosa, found the tricyclic desipramine to be significantly superior to placebo in reducing the frequency of binges, reducing the tendency for disruptive environmental events to precipitate binges (less disinhibition), reducing hunger, and increasing dietary restraint. Another report of the tricyclic imipramine (
22) found that although the median decrease in frequency of binges was 90% in the imipramine-treated group, there was no significant difference in response compared with placebo. However, the exceptionally high level of placebo response (greater than 70% median decrease in frequency of binges) renders this study uninformative with respect to any potential beneficial effects of imipramine.
Also noteworthy among our results was the high placebo response rate (19 [44%] of the patients given placebo displayed a greater than 50% reduction in binges/week, and 18 [42%] were rated as much improved or very much improved overall). Even higher placebo response rates have been observed in two other studies of binge-eating disorder (
8,
22). These figures suggest that binge-eating disorder may often improve even with placebo. Therefore, caution should be exercised in interpreting the results of open-label pharmacological studies of binge-eating disorder, as well as nonpharmacological studies, especially those using only waiting-list control groups. Also, these results argue for a conservative approach in offering treatment to such patients, since many will tend to improve with only placebo treatment.
The effects of medication on weight in binge-eating disorder have been variable. Along with this investigation, other studies have suggested that SSRIs may cause a modest amount of weight loss. Fluvoxamine was associated with weight loss in an open trial of obese binge eaters (
15). In a controlled study of fluoxetine plus behavior therapy compared with behavior therapy alone (
23), fluoxetine plus behavior therapy was associated with significantly greater weight loss in obese binge eaters. The weight loss effect did not appear to be specific to binge eaters, however, because obese non-binge-eaters in the fluoxetine-plus-behavior-therapy group also displayed significantly greater weight loss than the behavior-therapy-alone group. There is less evidence for a weight-reducing effect of tricyclics. In placebo-controlled studies, neither desipramine (
9) nor imipramine (
22) was associated with significant weight loss. However, in a study in which patients who had completed 12 weeks of cognitive behavior therapy received either open-label desipramine plus weight loss treatment or weight loss treatment alone (
24), the desipramine-treated patients lost significantly more weight. Finally, somewhat surprisingly, the appetite suppressant
d-fenfluramine (
8) was not associated with significant weight loss in severely overweight women with binge-eating disorder. Thus, although preliminary evidence suggests that treatment with SSRIs, but not tricyclics or
d-fenfluramine, is associated with weight loss in binge-eating disorder, the effects appear to be modest.
The reduction in frequency of binges and the overall improvement observed in this study are similar to the results reported in studies of SSRIs and other antidepressants in bulimia nervosa. Among the SSRIs, fluvoxamine and paroxetine have been reported effective in uncontrolled studies, and fluoxetine has been reported effective in placebo-controlled studies (
10–
13). Similarly, numerous studies have shown efficacy for tricyclics, MAOIs, and atypical antidepressant agents, although not all studies have yielded positive results (
12,
13). In addition to studies showing efficacy in acute treatment, one study (
25) found fluvoxamine superior to placebo in preventing relapse in patients with bulimia nervosa who had been successfully treated with inpatient psychotherapy.
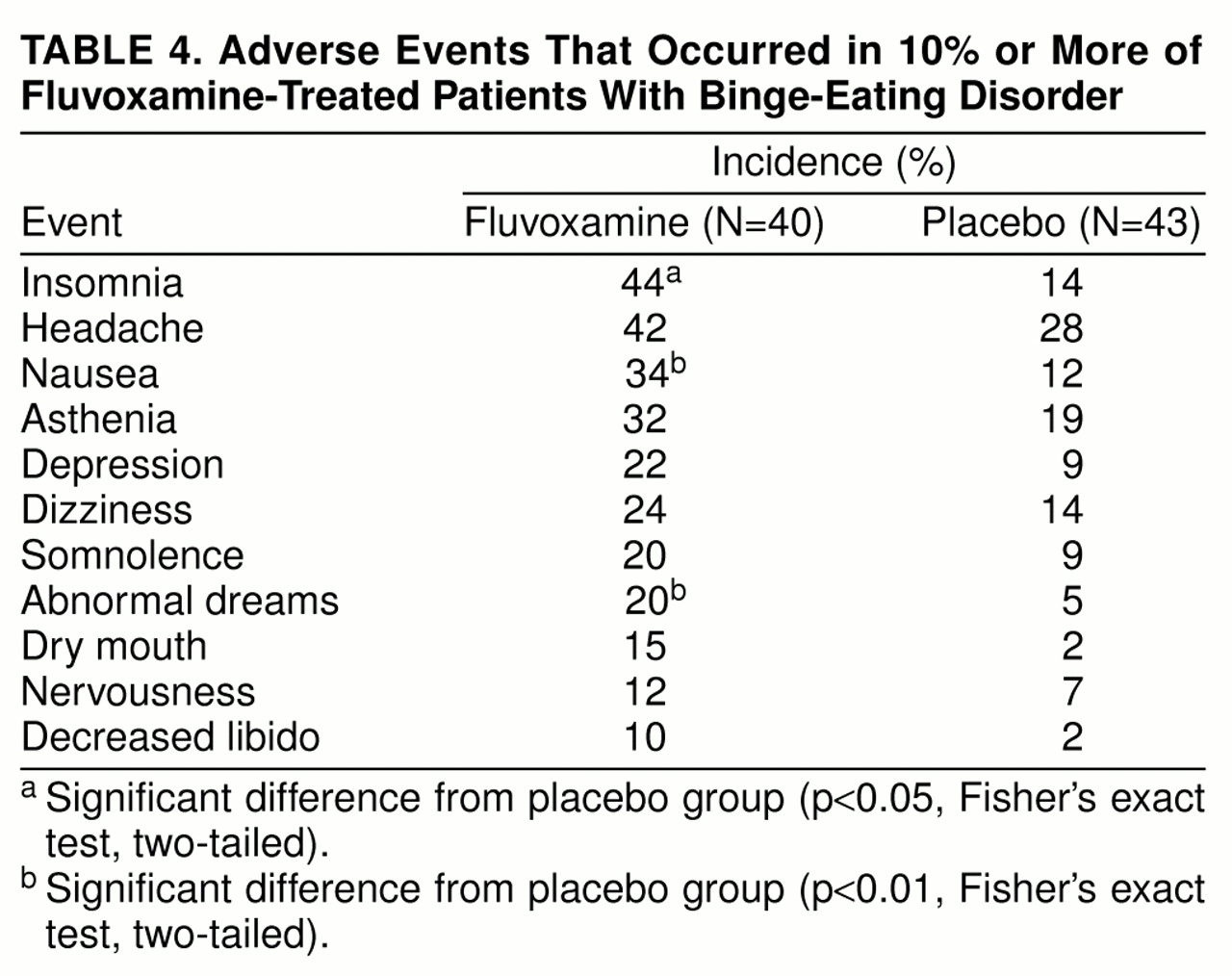
Fluvoxamine was well tolerated by most of our patients. However, 12% of fluvoxamine-treated patients withdrew because of nausea, sedation, or lightheadedness—all of which are known side effects of fluvoxamine (
26).
The mechanism of action of fluvoxamine in binge-eating disorder remains uncertain, as does the nature of the putative physiological abnormality in binge-eating disorder that is corrected by fluvoxamine. It is possible that fluvoxamine acts as an appetite suppressant and thereby reduces the urge to binge. Because nausea is a common side effect of fluvoxamine, it is possible that this effect may have contributed to the reduction in binge eating in some patients. It is also possible that fluvoxamine, as an SSRI, corrects a specific abnormality of serotonin neurotransmission in binge-eating disorder. Finally, because medications with antidepressant properties from several chemically distinct classes may be effective for a number of disorders—including, among others, certain mood, anxiety, and eating disorders—these medications may have many separate effects or, as some of us have suggested (
27), the disorders responding to these medications may share pathophysiological similarities.
Nonpharmacological therapies have also been investigated in binge-eating disorder and similarly defined conditions. Studies focusing on binge eating have reported success with group cognitive behavior therapy and group interpersonal therapy in reducing the frequency of binges; studies focusing on weight loss have generally been less successful, particularly in maintaining weight loss (
2). However, to our knowledge, no controlled trial of any form of psychotherapy in DSM-IV-defined binge-eating disorder has appeared. Thus, at present it is difficult to assess the efficacy of psychotherapy for binge-eating disorder, much less the relative efficacy of pharmacotherapy and psychotherapy.
Several limitations of this study should be considered. First, because the duration of double-blind therapy was 9 weeks, the results may not generalize to a longer duration of treatment. However, anecdotal clinical experience suggests that antidepressant treatment may be effective for longer periods of time in binge-eating disorder (
6). Furthermore, open follow-up studies of patients with bulimia nervosa (
28–
30) have reported good efficacy with SSRIs and other antidepressants on long-term follow-up, and one study (
25) has reported efficacy of fluvoxamine in relapse prevention. Nevertheless, it is important to study the long-term use of SSRIs and other medications in binge-eating disorder because almost all patients require more than 9 weeks of treatment.
Second, although investigators at the three sites were all experienced with the rating instruments (SCID, CGI, Hamilton depression scale), no formal assessment of interrater reliability was performed. Although we incorporated terms in the statistical model to adjust for the effects of center, it is possible that differences between raters may have affected the results. However, because such effects would likely be comparable for the two treatment groups, the expected effect of interrater unreliability would be to increase the standard errors of the estimates and thus produce overly conservative estimates of the significance of differences between fluvoxamine and placebo.
Third, because more fluvoxamine-treated patients experienced adverse events during the trial, it is possible that blindness to treatment assignment by patient or investigator may have been compromised in some cases (functional unblinding). The expected effect of unblinding would be to bias the results toward showing a greater effect for fluvoxamine than for placebo. The likelihood of this potential effect was reduced by the frequent occurrence of adverse events similar to those possibly related to fluvoxamine—such as asthenia, insomnia, somnolence, nausea, headache, and dizziness—in the placebo group.
Fourth, we excluded individuals with several forms of current or lifetime psychopathology, including current or recent major depressive disorder, lifetime substance dependence, and lifetime obsessive-compulsive disorder. These exclusions may have affected the generalizability of the findings, in that the results may not hold for individuals with binge-eating disorder who have certain forms of comorbid psychopathology. However, major depressive disorder is the most common form of comorbid psychopathology in patients with binge-eating disorder (
2,
3,
5,
6), and fluvoxamine is effective in the treatment of major depressive disorder (
31). Thus, exclusion of patients with recent major depressive disorder might be expected, if anything, to lead to a more conservative estimate of the effect of fluvoxamine.
Fifth, the size of the study group was relatively small. Therefore, the power to detect some potentially relevant differences between groups was low, particularly on secondary outcome measures that assessed a small range of potential change, such as the Hamilton depression scale.
In summary, in a multicenter, placebo-controlled, double-blind trial, we found fluvoxamine to be effective on most outcome measures and generally well tolerated in a short-term study in patients with binge-eating disorder. These preliminary results suggest that fluvoxamine may represent a promising treatment for binge-eating disorder.