Study Groups
We evaluated all eligible admissions to New Hampshire Hospital over 2 years between 1994 and 1996. As the only public psychiatric hospital in the state, New Hampshire Hospital receives admissions from all regions of New Hampshire. The eligibility criteria for the study included a diagnosis of severe and persistent mental illness (e.g., schizophrenia, schizoaffective disorder, bipolar disorder, major depression) according to the Structured Clinical Interview for DSM-III-R (SCID) (
25), no organic mental syndrome or disorder, and a 6-month connection with a clinician in the New Hampshire mental health system. The selection procedure for study inclusion was blind to the clients' substance abuse status. A prior connection in the New Hampshire mental health system was necessary to obtain the clinician ratings of substance use disorder used in establishing the criterion diagnosis (to be described). Each patient was enrolled in the study only once, regardless of the number of admissions to New Hampshire Hospital over the course of the study. During the 2-year period, 352 patients met these eligibility criteria, and 320 (90.9%) of the eligible patients provided written informed consent to participate in the study. The first 247 patients admitted became the index study group, and the next 73 patients formed the validation study group.
The index study group of 247 patients had an average age of 38.03 years (SD=8.82); 52.2% were female (N=129), 1.6% were non-Caucasian (four of 246), 84.6% were not married (N=209), and 73.9% had graduated from high school or had equivalent education (176 of 238). Primary psychiatric diagnoses were available for 245 patients; most patients had primary diagnoses of schizophrenia (19.2%, N=47), schizoaffective disorder (24.9%, N=61), bipolar disorder (19.2%, N=47), or major depression (12.7%, N=31); 24.1% of the patients (N=59) had other diagnoses. A group of 73 patients consecutively admitted after the index group constituted the validation study group. These patients were similar to the index group on all demographic and clinical characteristics. Both groups were similar to all patients admitted to this hospital during this period on age, education, ethnicity, and marital status. Approximately one-third of all admitted patients were not eligible for the study because their diagnoses did not qualify as severe mental illness (e.g., personality disorders, adjustment disorder, or acute stress disorder).
Measures
Criterion diagnosis. The criterion, or “gold standard,” diagnosis was based on clinician ratings on the Clinician Rating Scale (
3) and an independent diagnosis for current (last 6 months) substance use disorder according to the SCID. Our criterion for alcohol or drug use disorder was a finding of active abuse or dependence in the past 6 months according to either the Clinician Rating Scale or the SCID.
The Clinician Rating Scale addresses the problem of diagnostic sensitivity by reducing the rater's reliance on disclosure through either self-report or interview procedures. Trained clinicians make ratings on this scale on the basis of self-reports, interviews, longitudinal behavioral observations, collateral reports, and all clinical records, including results from medical examinations, psychiatric evaluations, and laboratory tests, over the past 6 months. Separate ratings are made for alcohol and other drugs on 5-point scales: 1=abstinence; 2=use without impairment; 3=abuse (DSM-III-R criteria); 4=dependence (DSM-III-R criteria); and 5=severe dependence (DSM-III-R criteria for dependence plus a recurrent need for institutionalization due to substance use disorder). For the purpose of examining screening devices, we collapsed the five Clinician Rating Scale ratings into two levels: ratings of 1 and 2 indicated nonabuse, and ratings of 3–5 denoted substance use disorder. Clinicians made separate ratings for alcohol, cannabis, and cocaine.
The Clinician Rating Scale is reliable, sensitive, and specific when used by case managers who follow their mentally ill patients over time in the community (
3,
8,
26–
29). Analyses of interrater reliability, comparing ratings of trained clinical case managers and team psychiatrists, have yielded kappa coefficients between 0.80 and 0.95 for current use disorder (
3,
8). Clinician Rating Scale ratings have been validated with psychiatric patients by using other substance abuse measures (
3,
26,
28) and measures of motives and expectations for substance abuse (
29). Other researchers (
2,
16,
17,
30) have also shown that clinician ratings are better for detecting substance use disorder than is self-report.
The SCID (
25) is a structured interview that entails specific questions for DSM-III-R criteria. The substance use disorder section addresses alcohol and other drugs separately. For the purpose of this study, interviewers focused the alcohol and drug questions on the 6 months preceding hospitalization so that the time interval coincided with that represented by the Clinician Rating Scale ratings.
Substance use disorder among psychiatric patients is often detected with one mode of assessment but not another, and the discrepancy between any two measures is typically due to nondisclosure on one measure rather than to a false positive on the other (
3,
11,
17,
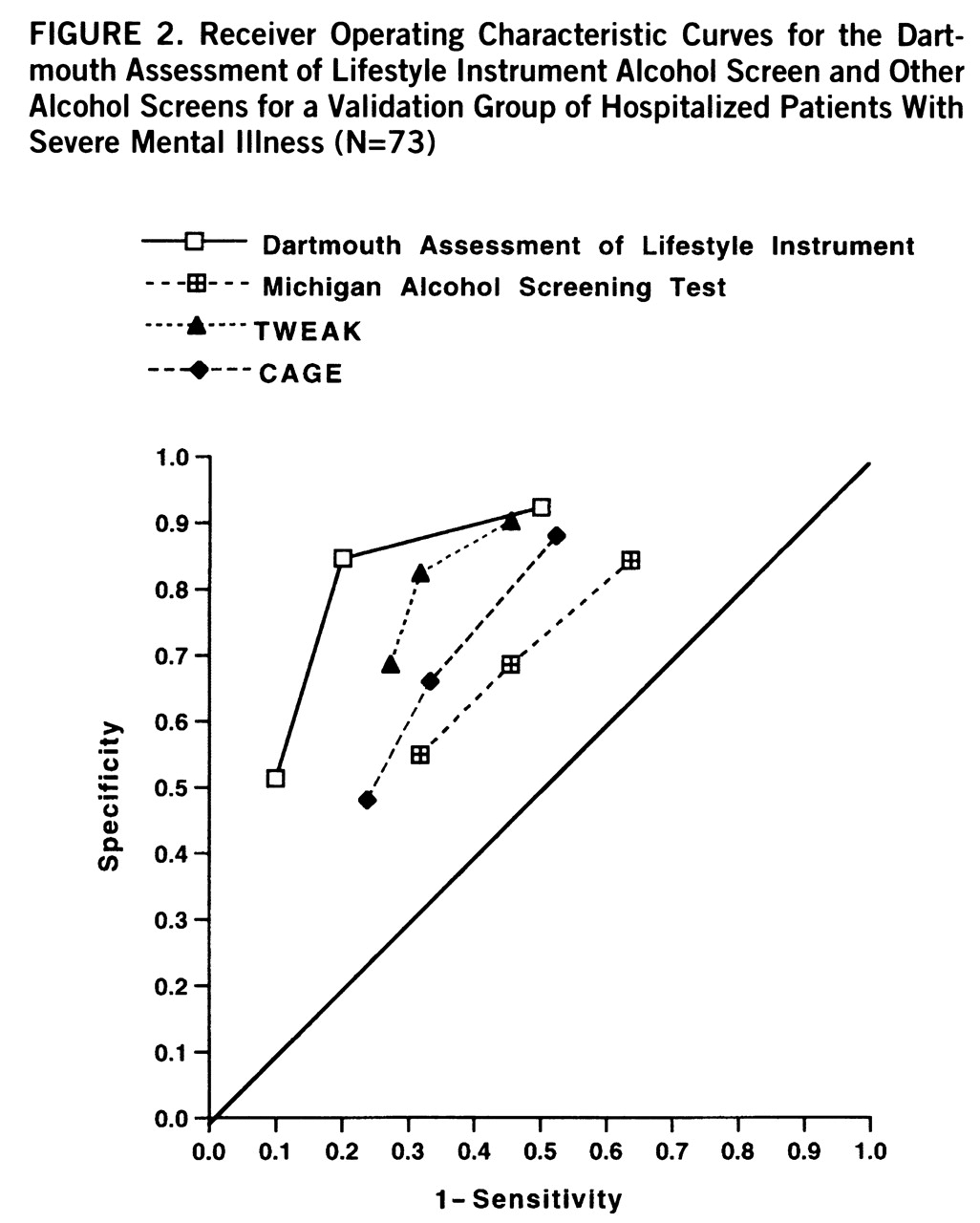
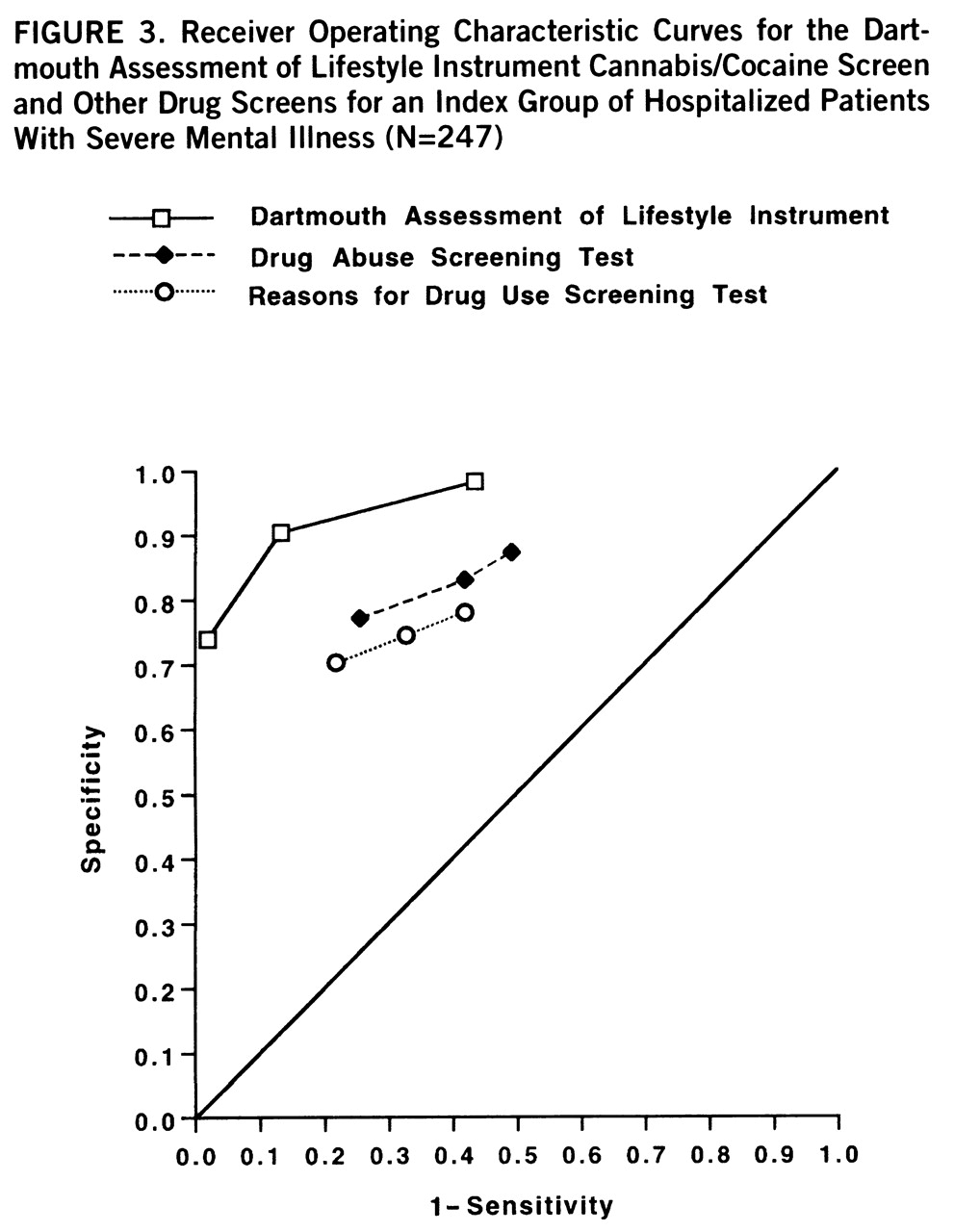
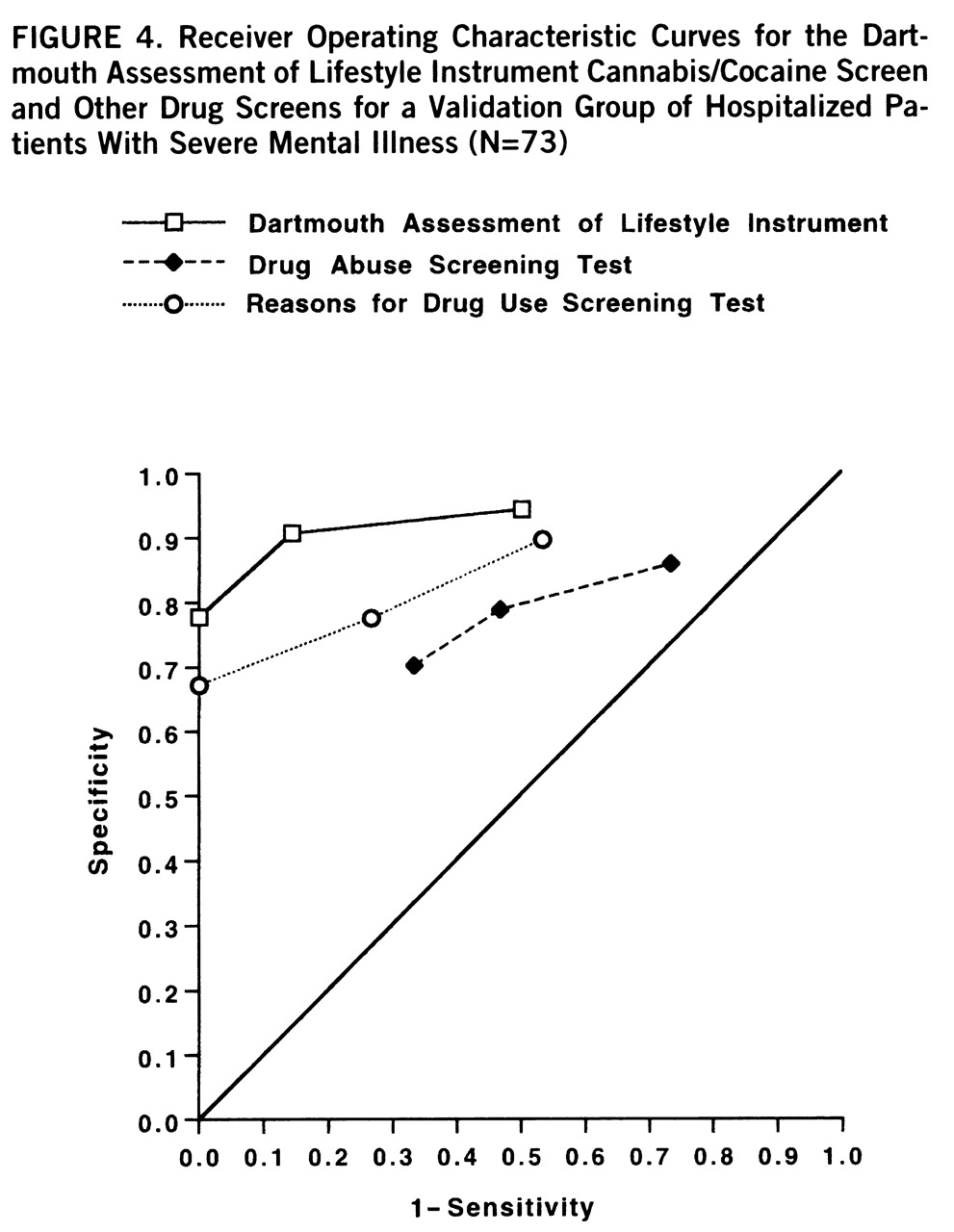
31). For this reason, our criterion diagnosis was defined as the presence of substance use disorder according to either the Clinician Rating Scale or the SCID. Among the total of 118 patients with an alcohol use disorder according to either the Clinician Rating Scale (scores of 3–5) or the SCID, 46 patients (39.0%) were identified by both the Clinician Rating Scale and SCID, 47 patients (39.8%) were identified by only the Clinician Rating Scale, and 25 patients (21.2%) were identified by only the SCID. Among the 69 patients with drug use disorder, 26 (37.7%) were identified by both the Clinician Rating Scale and SCID, 26 (37.7%) were identified by only the Clinician Rating Scale, and 17 (24.6%) were identified by only the SCID. The SCID-only diagnoses were taken as face valid, as already described, but the diagnoses determined by only the Clinician Rating Scale were confirmed by a check of all community records on 15 randomly selected patients. These records contained strong confirmatory evidence. For example, one patient had been hospitalized five times because of alcohol abuse during the 6-month interval but was not given a diagnosis of substance use disorder with the SCID because he denied any use.
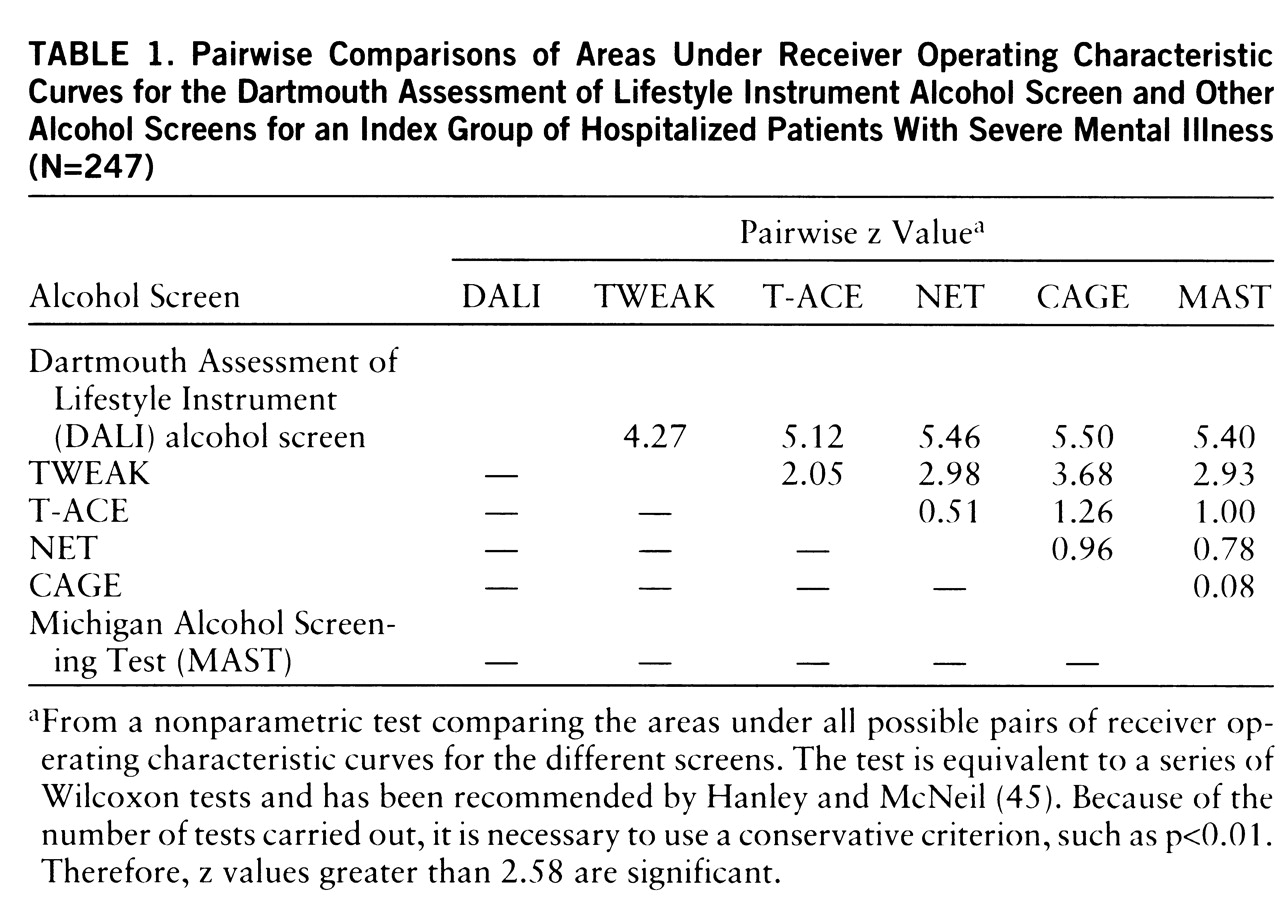
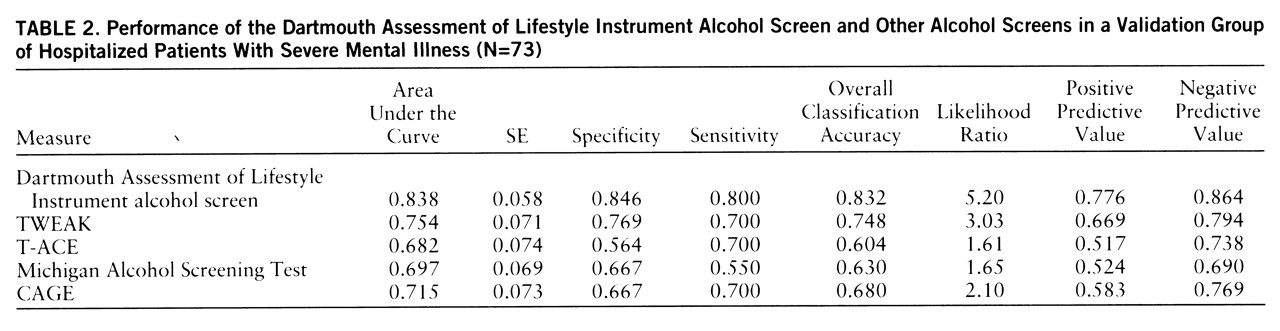
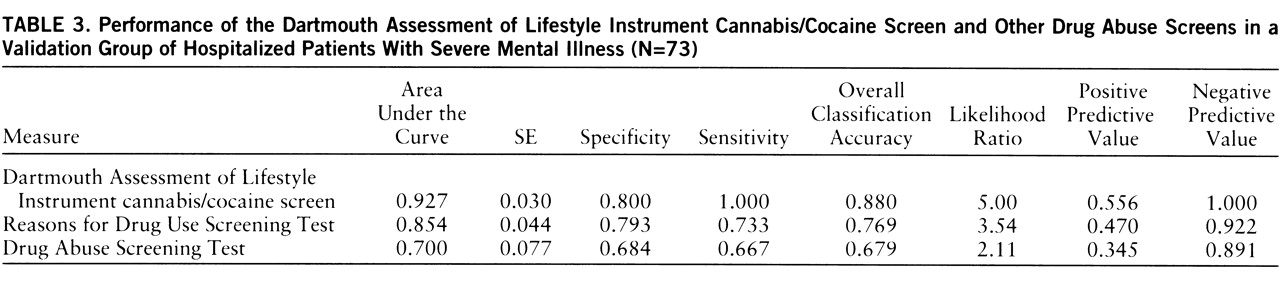
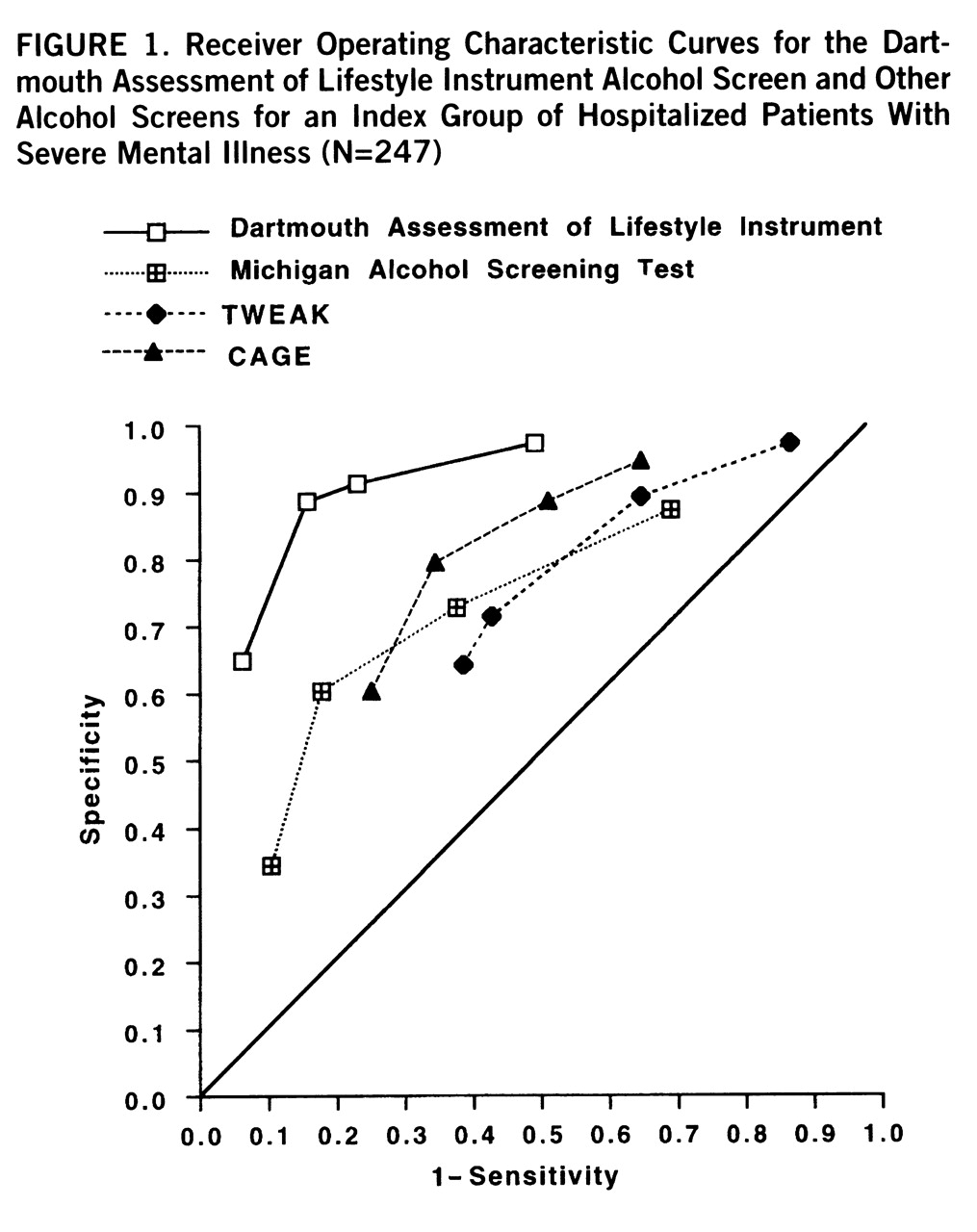
Substance use disorder screening instruments. The following widely used screens were administered in their entirety to all participants as part of a comprehensive battery: MAST (
19), CAGE (
32), T-ACE (
33), NET (
34), TWEAK (
35), Drug Abuse Screening Test (
36), and Reasons for Drug Use Screening Test (
37). These scales vary in length from three to 31 items, and all have shown good reliability and validity with nonpsychiatric populations. Although these screens are often self-administered, in this study trained interviewers administered the entire battery. This procedure has been recommended by both researchers and clinicians assessing acutely and severely mentally ill persons because problems of attention, motivation, question comprehension, and literacy are likely to interfere with direct self-report procedures (for example, see reference 38). At the study site we had evidence that standard scales, such as the SCL-90-R (
39), had much lower completion rates when self-administered than when used in the interviewer-administered format. Some of the scales have overlapping items, and we asked each of the overlapping questions once.
Structured interviews for substance use disorder. We also incorporated portions of the Life-Style Risk Assessment Interview (
40), the Alcohol Research Foundation Intake Interview (
41), and the Addiction Severity Index (
42). The Life-Style Risk Assessment Interview was designed to be nonthreatening and to detect alcohol use disorder in medical settings where patients' presenting complaints are not related to substance use disorder. We incorporated the nine introductory questions from this scale to reduce subject defensiveness. The Alcohol Research Foundation Intake Interview deals with legal and treatment history, alcohol consumption patterns, quantity, social context, beverage preference, recent drug use, and adverse consequences of alcohol use. The Addiction Severity Index sections on drug and alcohol use, family and social relationships, and family history of substance use disorder were also included.
Cognitive function. The Mini-Mental State examination (
43) is a brief screen for assessing cognitive functioning. It consists of 11 questions. The maximum score is 30, and a score of less than 23 is generally taken to indicate cognitive impairment.
Procedures
Researchers tracked all admissions to New Hampshire Hospital daily to determine study eligibility. Hospital charts were reviewed to determine probable diagnosis and prior connections with community mental health centers, and staff nurses provided initial estimates of current mental status, ability to provide informed consent, and approachability. Hospital psychologists and trained clinicians, independent from the research interviewers, administered the SCID, including the alcohol and substance use module. Once probable eligibility was determined, the project coordinator contacted potential subjects to explain the nature of the study, to obtain written informed consent, and to administer the Mini-Mental State examination. When appropriate, consent from legal guardians was also obtained.
Trained research interviewers administered the composite substance use disorder interview, which averaged less than 1 hour. Interrater reliability was checked throughout the study on every 10th patient. To simulate usual clinical procedures, the subjects were informed that information gleaned during the interview would be shared with their clinical team at the hospital and treated as part of the clinical record.