Light therapy is recognized as an effective treatment, routinely prescribed for seasonal affective disorder (
1,
2). Early clinical studies exposed subjects to 2,500 lux for 2–6 hours daily. These lengthy daily treatments were often inconvenient (
3). Compliance became a problem (
4). Several studies of the side effects of light therapy were done (
3,
5–
8). These showed that low-intensity (2,500–3,500-lux) light therapy produced side effects in some users.
In 1990 Terman et al. (
9) reported that shorter exposure to brighter, 10,000-lux light therapy produced a 75% rate of improvement in seasonal affective disorder. Clinicians began to recommend these 10,000-lux treatments. Our purpose here is to present data on side effects experienced by 70 subjects with seasonal affective disorder who underwent short-term 10,000-lux treatment. Aside from a study of ocular side effects by Gallin et al. (
10), we are unaware of other published reports of side effects from 10,000-lux light therapy.
METHOD
Participants were selected from referrals to a specialty seasonal affective disorder program over two fall-winter seasons (1993–1995). All met the DSM criteria for a seasonal pattern, and each participant received a psychiatric evaluation and was assessed with the Hamilton Depression Rating Scale, Seasonal Affective Disorder Version (
11). For 46 subjects the scale was administered both before and after treatment. A minimum Hamilton depression scale score of 15 was required. A total of 70 patients met the criteria; 59 (84.3%) were female, and their average age was 41.5 years (SD=11.5). Written informed consent was always obtained.
The subjects underwent a 5-day protocol of daily 30-minute light therapy with commercial 10,000-lux light units. Nonresponders could continue with additional sessions. Their data are included. An experienced clinician supervised the sessions. The subjects reported side effects that developed during or after each treatment session, using a form we developed. Side effects were excluded if they were present before the light therapy trial.
RESULTS
The subjects underwent an average of 6.8 sessions each (SD=3.0). Of the 46 subjects for whom the Hamilton depression scale (seasonal affective disorder version) was completed both before and after treatment, 36 (78.3%) had posttreatment reductions in their Hamilton scores of more than 50%. After the initial five-session protocol, 42 subjects (60.0%) continued daily light therapy; these 42 included some subjects who responded within the initial five sessions. Ten (14.3%) dropped out before completing the initial protocol. Of the 32 subjects who reported side effects, six (18.8%) dropped out early but were included in the findings reported here. Of the 38 subjects without side effects, four (10.5%) dropped out. The difference in dropout rates was nonsignificant (χ2=0.33, df=1, p=0.52 with continuity correction).
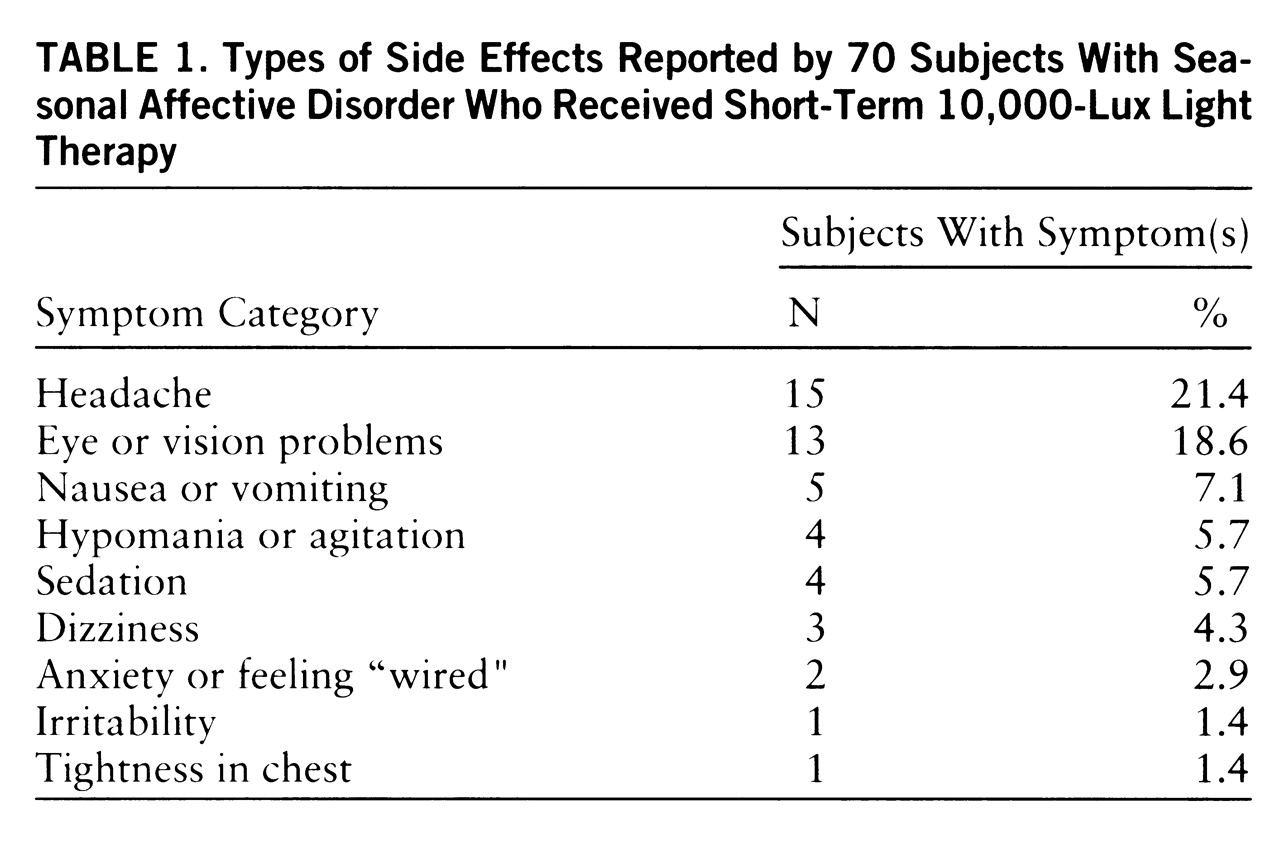
Table 1 lists the side effects by category. Of the 32 subjects (45.7%) who reported side effects, 23 (71.9%) experienced only one side effect apiece. Headaches were the most frequent type of side effect but, with one exception, ceased after the third day. Eye or vision problems, the second most common, included strain, excessive glare, seeing spots, blurring, and irritation. Few eye or vision problems occurred after the first 2 days. Nausea occurred mostly on the first day. Three subjects reported agitation on the first day. One experienced hypomania after the fifth day. None of the side effects was considered serious except the hypomania.
On day 1, 24 subjects (34.3%) reported side effects. By day 2 this decreased to 17 (24.3%), with a further decrease on day 3 to 12 (17.9%) of the 67 remaining subjects. By days 4 and 5 fewer than 10% of the subjects reported side effects.
DISCUSSION
Our response rate, 78.3%, is similar to that in the Terman et al. study of 10,000-lux light therapy (
9) and compares favorably to response rates from earlier studies of dimmer light therapy (
2).
Eye or vision problems and headaches were each reported by about 20% of the subjects. While this is a slightly lower frequency than Oren et al. (
3) found when using 2,500-lux treatments for a mean of 4 hours daily, overall our findings are similar to those of Oren et al., who found that eye or vision problems and headaches were the most common side effects. Labatte et al. (
7) reported a higher rate of eye or vision problems.
Our data collection differed from that in previous studies. We received reports after each treatment session. This may have led to the reporting of fewer side effects than would have been found from use of a structured questionnaire. Lack of a control group also weakened our findings.
None of our subjects reported insomnia. Oren et al. (
3) reported a 24% rate of insomnia, and Labatte et al. (
7) found a 29.9% rate. The discrepancy between our finding in this regard and the rates in those other studies may be attributable to the difference in intensity and duration between 10,000-lux and 2,500-lux treatments or to the fact that almost all of our subjects underwent light therapy before 5:00 p.m. Labatte et al. reported a higher rate of insomnia among subjects who received evening treatment than among subjects who received morning treatment.
Although almost one-half of the participants in our study reported side effects, these were generally mild and short lived. Several subjects reported transient eye or vision problems. Previous follow-ups of dimmer, 2,500-lux treatments showed no structural or physiologic eye changes (
12,
13). Gallin et al. (
10) provided evidence for the ophthalmologic safety of brighter light.
These positive results from 10,000-lux light therapy are encouraging. Our findings support the use of 10,000-lux light therapy for newly diagnosed seasonal affective disorder and suggest that patients currently receiving 2,500-lux treatments be considered for 10,000-lux light therapy if the less intense treatments are inconvenient or not effective.