Depersonalization is characterized by a detachment from one’s sense of self and one’s surroundings and a feeling of being an automaton or as if in a dream while maintaining an adequate testing of reality. Individuals meet the criteria for depersonalization disorder if they suffer from persistent or recurrent depersonalization symptoms that lead to significant distress or dysfunction and do not occur exclusively as part of another axis I disorder. Despite an increased interest in dissociation in recent years, not much is known about the etiology, course, prevalence, and incidence of depersonalization. Some reports suggest it may be the third most common psychiatric symptom after depression and anxiety; however, it is highly resistant to both psychotherapeutic and pharmacological treatment
(1). Depersonalization is classified in DSM-IV as a dissociative disorder. Although there exists an impressive theoretical literature on dissociation, there have been few empirical attempts to substantiate theoretical models. The clinical literature is mostly concerned with establishing the premise that dissociation functions to protect the self from overwhelming emotional experiences and views dissociative disorders primarily as a response to trauma
(2). In the nineteenth century, Janet
(2) described dissociation as a narrowing of attention and a disorganization in the ordinary integrative functions of consciousness that occur when a person experiences vehement emotions. Since then, long-lasting alterations in cognitive processes in response to trauma have been documented
(3). However, it is unclear at what stage of information processing dissociation takes effect and whether it involves alterations in the initial stages of encoding information, while it is being overwhelmed by trauma, or is reflective of later amnesic barriers to the retrieval of information.
Neodissociation theories
(4,
5) view dissociation as reflective of mechanisms that all people use to varying degrees. Their central premise is that dissociation involves a weakening of the highest-order executive control functions that leave infrastructures more freedom to operate independently. Strong activation of the executive system has the experiential equivalent of concentration, consciousness, and “self-hood,” whereas its weakening results in the emergence of the mind’s underlying inherently dissociated nature. Hilgard’s famous documentation of the “hidden observer” phenomenon in experiments that involved hypnotically induced analgesia and deafness is particularly illustrative of this theory
(4). Operationalizations of these theories rest on the prediction that the ability to dissociate should facilitate performance on dual-task situations such as divided and selective attention. However, studies have failed to show differences between hypnosis-prone and comparison subjects on task-interference conditions
(6). Many of these experiments rely on the premise that proneness to hypnosis is a reliable marker of dissociation proneness, whereas it appears that only a small subgroup of people are both highly dissociative and highly hypnotizable
(6). Waller et al.
(7) have argued that pathological dissociation is a categorical taxon rather than a continuous entity, which implies that normal populations would not be applicable to studies of dissociative disorders.
Several studies have examined the relationship between dissociation and cognitive functioning in patients with dissociative identity disorder. These mostly point to deterioration and excessive scattering of interest on intelligence tests, with some signs of neuropsychological deficits on distractibility measures
(8,
9). There was one early study
(10) that compared the cognitive functioning of depersonalized subjects to matched depressive and anxious patients in which tests of psychomotor abilities did not differentiate between the groups. Otherwise, to our knowledge, there has been no systematic study of the cognitive profile involved in depersonalization to date. Assessing this profile was the purpose of this study. Since neodissociation theories implicate changes in executive control functions and memory, and since patients’ subjective reports include disruptions in attention and memory, we decided to focus particularly on those areas in the context of general intellectual functioning. Our hypotheses were that the depersonalized group would show deficits in functioning on measures of attention and memory in relation to the comparison group but that it would exhibit uncompromised intelligence on the WAIS-R.
DISCUSSION
Results of the assessment test battery indicated that depersonalized subjects differed from comparison subjects on key features within a general context of comparable intellectual ability. These differences closely mirror their subjective reporting of difficulties in perception, attention, and memory. The groups’ comparable general intellectual functioning is crucial for the interpretation of the rest of the findings in suggesting that depersonalized subjects do not demonstrate the general and diffuse deterioration in functioning that is often seen in conjunction with psychiatric disorders such as schizophrenia or depression
(26). The groups did not differ in various measures of sequencing or reaction time that could intimate a disorganization or a slowing down of cognitive processing.
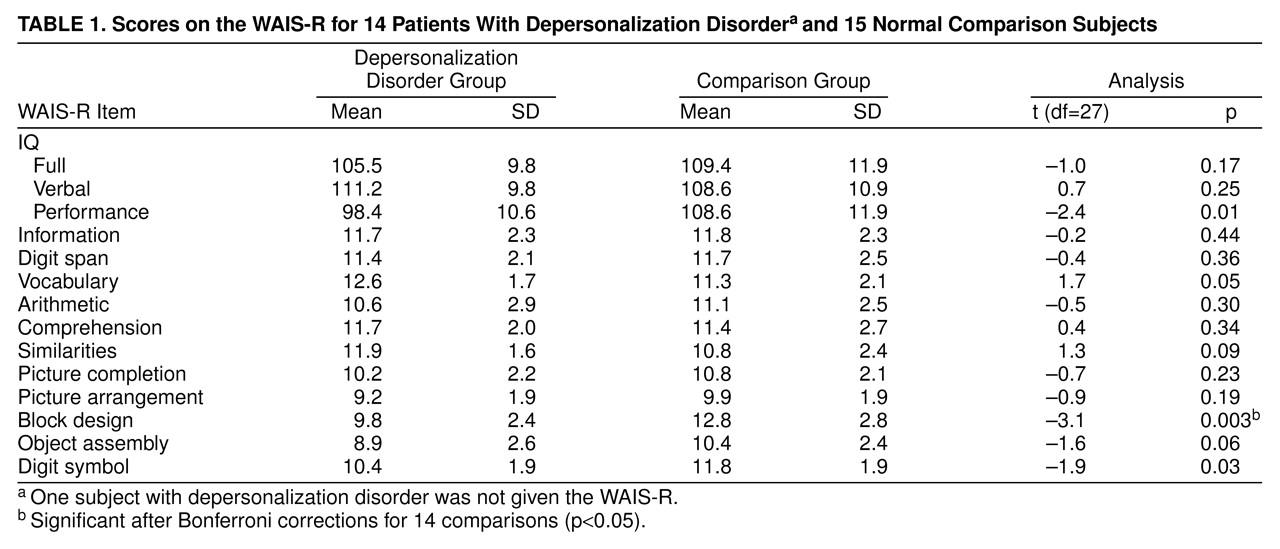
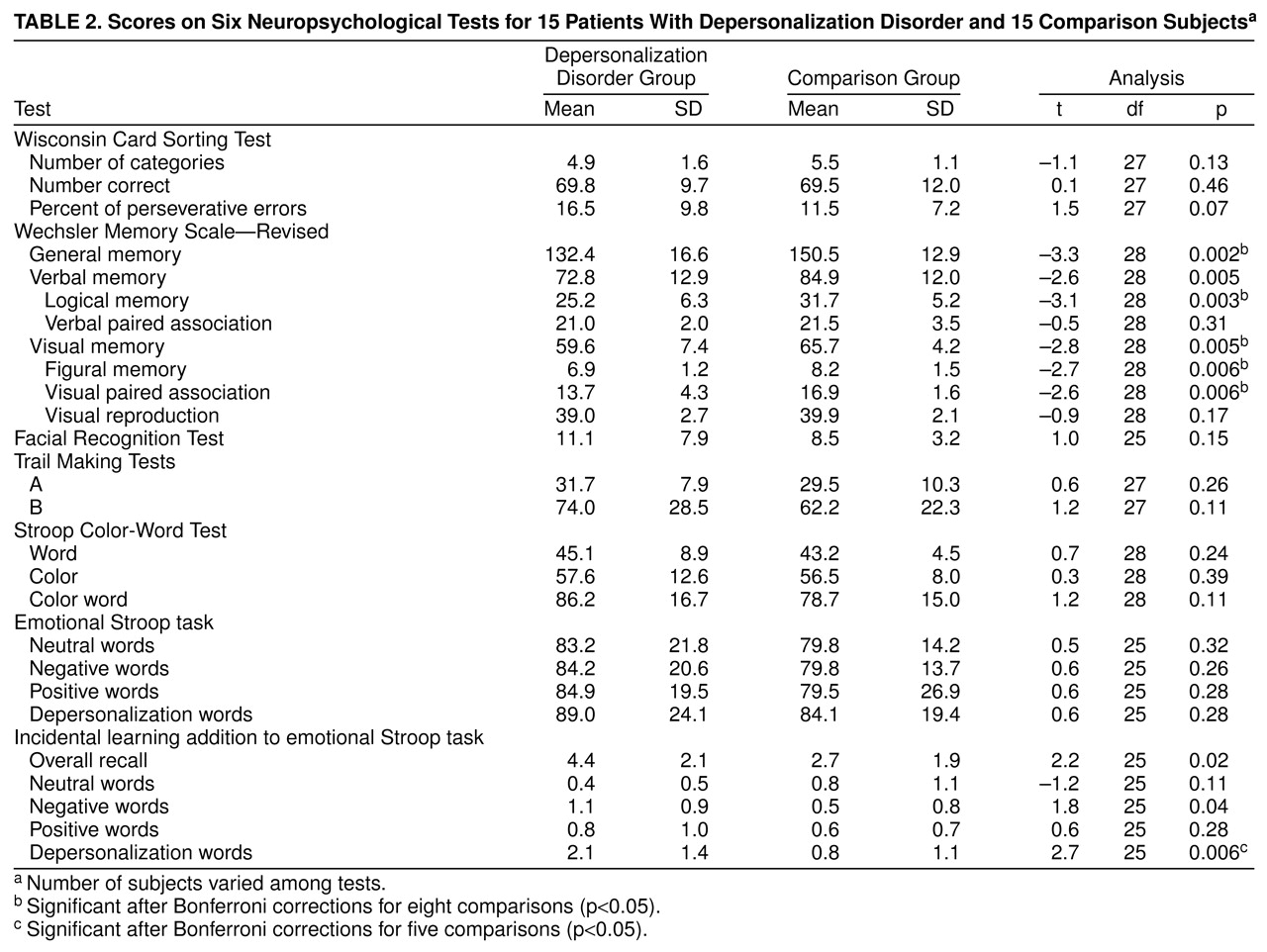
The depersonalized subjects did, however, demonstrate clear impairments on visual-spatial tasks. They did poorly on some performance tasks of the WAIS-R—significantly so on a measure of spatial reasoning (the block design subtest). The block design subtest score was the single best predictor of diagnostic group membership in the regression analysis; it emphasized the importance of this factor in differentiating between the groups. Attributing this impairment to problems in visual-motor coordination should be ruled out since the groups did not differ on scores on graphomotor tests such as the digit symbol subtest, Wechsler scale visual reproduction subtest, and Trail Making Tests A and B. The materials used in the block design subtest are three-dimensional cubes, which is of great interest since depersonalized subjects often report a subjective flattening of their visual-perceptual world into two dimensions. It is not uncommon for them to have been referred for psychiatric help after consultations with ophthalmologists, whose standard examinations yielded no findings. In fact, on the Wechsler scale, depersonalized subjects had difficulties on tasks involving memorizing geometric figures (the figural memory subtest) and pairs of colors (the visual paired association subtest)—both abstract visual stimuli. These findings lead us to conclude that depersonalization is associated with deficits in visual perception and visual-spatial reasoning with both three- and two-dimensional stimuli.
Comparable scores of the groups on the WAIS-R information and vocabulary subtests imply that depersonalized subjects do not suffer from gross impairments in long-term-memory. They also did well on various verbal short-term memory tasks, including the incidental learning test, digit span, and verbal paired association memory subtests—all sensitive to learning deficits that involve complex or novel information. However, the depersonalized subjects did much worse than the comparison subjects on the logical memory subtest; the test is unique in that it employs sentences rather than words and provides a measure of what is retained when more information is presented than most people can remember. Thus, the depersonalized subjects’ short-term verbal memory capacity tended to significantly drop in relation to that of comparison subjects when it was presented with an overload of information.
So far it is apparent that depersonalized subjects demonstrate certain compromises in both visual and verbal short-term memory with stimuli of both an abstract and meaningful nature. It is still questionable whether these deficits can be attributed to difficulties in taking in new information—i.e., in perception and attention or in retrieval—although the subjects’ adequate long-term memory supports the former. One of the symptoms that they describe is a disruption in their sense of familiarity with both themselves and their surroundings. Although they know better, they feel as if all is new, whereas their self is at an unbridgeable distance from ongoing perceptions. The blunted sense of familiarity could blatantly compromise their functioning on memory tasks that rely on recognition. Support comes from the fact that many of their visual perception and discrimination problems were not apparent when the stimuli were right in front of them, as in the Facial Recognition Test.
One of the key findings in this study is the depersonalized subjects’ impaired functioning on the Continuous Performance Test. The features of attention that are targeted in this test are the ability to selectively attend to the stimuli presented and the ability to sustain attention, as measured by decrements in functioning over time. Depersonalized subjects showed significant deficits only when visual noise was added—in response to which they tended to have more omissions, as opposed to an increased rate of false alarms—and did not differ in their ability to sustain attention over time. Degrading stimuli are among the methods used to isolate the stimulus-encoding, information-processing stage, as opposed to the response-selection and organizational stages. The addition of noise lowered the subjects’ perceptual sensitivity, which made it difficult for them to rapidly extract relevant stimulus features. The findings so far suggest that depersonalization is marked by a particular vulnerability at the level of perception and attention. Deficits in short-term memory could be, therefore, secondary to difficulties focusing, perceiving, and taking in new information.
Unlike we predicted, on the emotional Stroop task, the depersonalized subjects did not demonstrate more interference effects; they were therefore different from other clinical groups, such as patients with panic disorder and posttraumatic stress disorder, who reportedly demonstrate a strong attentional bias on the emotional Stroop task
(19). Their superior incidental learning test scores revealed that they did not ignore—and actually remembered—more emotionally charged words than did the comparison subjects; unnecessary information could potentially disrupt their task. Clearly, they can be highly perceptive and demonstrate good memory—at least when the information is of emotional significance to them. Possibly, their internal preoccupation is at the expense of allocating resources toward other aspects of their environment. Their awareness of these words weakens the hypothesis that their dissociative symptoms serve a defensive function and can be interpreted from a psychodynamic and structural point of view as a failure in repression. Repression is posited to defend the ego from anxiety-provoking information by making such material unavailable to conscious perception. Although both mechanisms aim to ward off pain, dissociation differs in that it involves a splitting off of whole chunks of experiences or self-states, which leads to an altered state of being, whereas repression is a more selective riddance of information and, in that respect, can be more adaptive. This issue will need to be further studied.
When we integrated some of our findings, it appeared that on the Continuous Performance Test, the depersonalized patients exhibited difficulties attending to target stimuli in the presence of noise; this is a task that involves selective attention. On the emotional Stroop task, they attended to irrelevant and potentially disruptive information. Our interpretation is that they find it difficult to willfully control and direct attention toward the key features of the stimulus. In terms of the neodissociation theory, the depersonalized subjects’ functioning on the emotional Stroop task and the incidental learning test supports the main hypothesis that their use of dissociation facilitates their performance on simultaneous tasks and reduces task interference. There were fewer clear-cut signs of a weakening of the executive-supervisory system, since on direct measures such as the Wisconsin Card Sorting Test, the patients showed no decline. However, on certain tasks that require the supervisory function of allocating attentional resources in response to task demands, such as the Continuous Performance Test, they did show impairment. The ability to cope with divided and selective attention tasks needs to be further studied.
The cognitive profile of the depersonalized group in this study differs from reports on patients with dissociative identity disorder. Depersonalized subjects’ scores were equivalent to those of comparison subjects on the intelligence test, whereas some case reports suggest that patients with dissociative identity disorder show above-average intelligence profiles
(27), and more recent studies demonstrate that dissociative identity disorder is associated with cognitive inefficiency and intertest scatter on intelligence tests
(9). Both patients with dissociative identity disorder and those with dissociative disorder not otherwise specified were reported to manifest abnormal intertest scatter on the verbal subtests of the WAIS-R
(10). This was attributed to deficits on the distractibility factor (arithmetic and digit span), which led the authors to recommend evaluating this population for comorbid attention deficit disorder by using the Continuous Performance Test. Depersonalized subjects did not show more verbal scatter or deficits on the distractibility factor of the WAIS-R. They did demonstrate significant deficits on the Continuous Performance Test; however, these subjects differ from typical patients with attention deficit disorder
(28) in that they have no particular difficulties sustaining attention over time, no increase in commission errors, and no problems on the Stroop-Color Word Test. The Continuous Performance Test’s profile of the subjects with depersonalization disorder was actually similar to reports on the functioning of patients with schizophrenia spectrum disorders. A low perceptual sensitivity on Continuous Performance Test items with degraded stimuli was demonstrated with relatives of schizophrenic patients
(29), replicated in later studies with schizotypal subjects, and found to be independent of anxiety and depression measures
(30). Low perceptual sensitivity on the Continuous Performance Test was also shown to be associated with the type B personality and with more frequent daydreams
(31).
Limitations of this study include the small number of subjects in each group in addition to use of a wide number of tests. The findings will need to be replicated. Future areas to focus on in studying depersonalization are primarily visual-spatial processing, attention, and short-term memory. Visual, auditory, and somatosensory modalities need to be studied in parallel and in intermodal integration. The logistic regression analysis shows the feasibility of using such tests as the Objective Diagnostic Criteria for Depersonalization. However, the fact that the same subjects were used for the regression analysis limits the inferences that can be drawn from it, and it will need to be validated on another group of subjects. To test the hypotheses regarding the defensive functions of dissociation, it would be helpful to study whether deficits are content dependent. Finally, it would be useful to study the connection between neuropsychological deficits and the depersonalized subjects’ sense of unreality. It still needs to be determined how their sense of unreality is related to disruptions in perception, an inability to connect preexisting memory traces, affective tags (familiarity), or to an altogether separate mechanism that removes from experiences their “realness.”