Neuroimaging studies have contributed greatly to the development of contemporary neurocircuitry models of obsessive-compulsive disorder (OCD). Among these, in vivo proton magnetic resonance spectroscopic imaging (
1 H-MRSI) is a technique that allows for the study of a number of brain chemicals without the need for exogenous tracers or exposure to ionizing radiation. It is important to note that this technique also provides valuable information regarding neuronal function. In particular,
N -acetylaspartate levels may constitute a sensitive means for monitoring neuronal cellular function
(1,
2) .
Reductions in
N -acetylaspartate levels within subcortical structures have been the most frequently reported findings in OCD patients
(3,
4) . Bartha et al.
(3) reported that relative
N -acetylaspartate levels in the left corpus striatum were significantly lower in OCD patients despite the lack of difference in caudate volumes between OCD patients and comparison subjects. Ebert et al.
(4) reported a decreased
N -acetylaspartate/creatine plus phosphocreatine ratio in the right striatum and anterior cingulate. Decreased
N -acetylaspartate levels (obtained from the
N -acetylaspartate/creatine plus choline ratio) in the medial thalamus were also reported in a study of pediatric OCD patients
(5) . Little is known regarding possible cortical abnormalities in OCD patients.
Method
Subjects
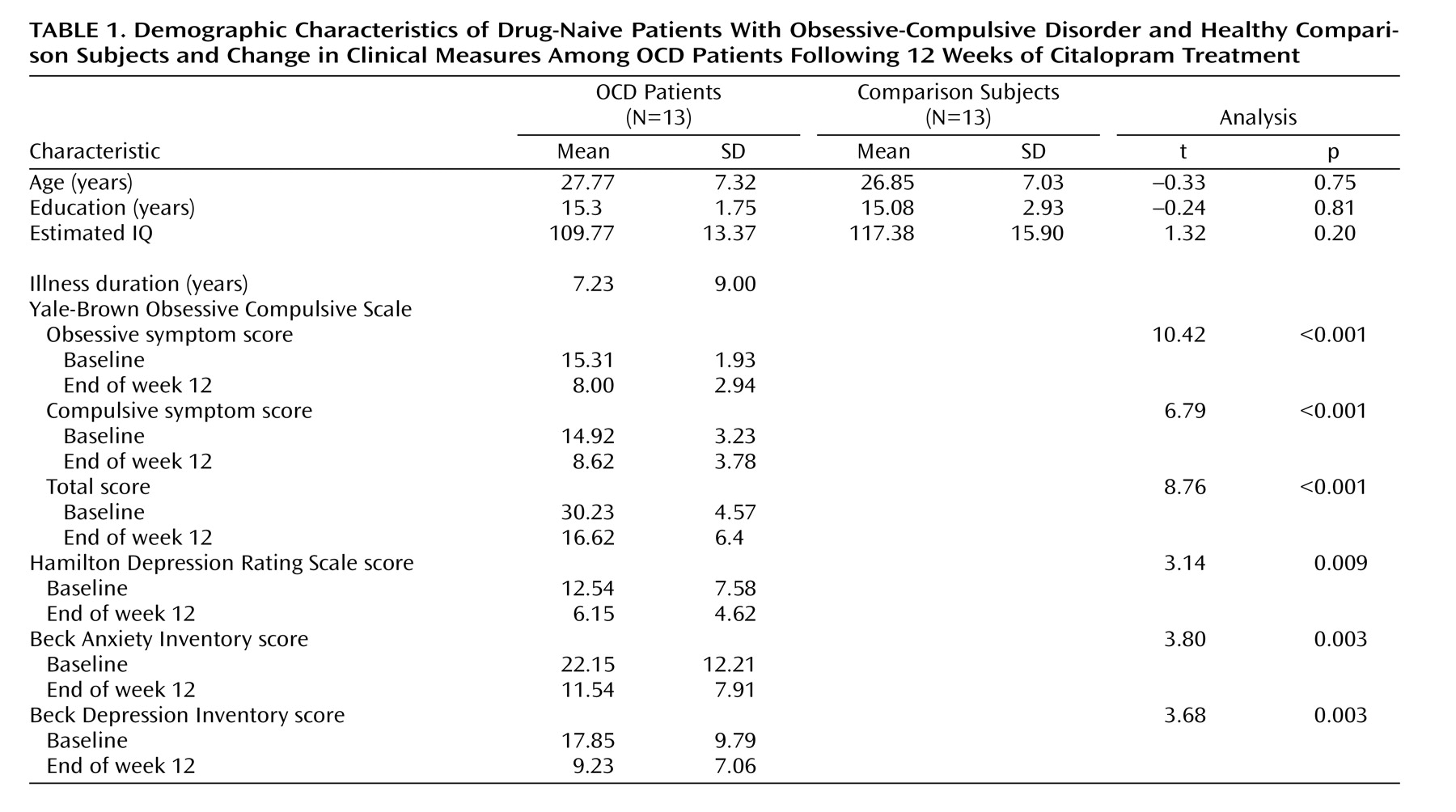
Thirteen patients who fulfilled DSM-IV criteria for OCD, as determined with the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID), were recruited. Thirteen sex- and age-matched comparison subjects were recruited through newspaper and leaflet advertisements. Absence of axis I psychiatric disorders in the comparison subjects was confirmed with the Structured Clinical Interview for DSM–IV Nonpatient Version (SCID-NP). Both groups consisted of eight men and five women. The demographic characteristics of the subjects in each group are presented in
Table 1 . There were no significant differences with regard to age, education, or mean IQ as estimated by the Korean version of the WAIS. All subjects were right-handed. Exclusion criteria were a history of psychosis, bipolar disorder, substance abuse or dependence, Tourette’s disorder or other tic-related conditions, significant head injury, seizure disorder, or mental retardation.
The patients had a mean duration of illness of 7.23 years (SD=9.00). Two of the OCD patients had comorbid major depressive disorder, and one patient had comorbid dysthymic disorder. Patients were drug-naive except one who had taken medication for a few days several years before the present study. None of the 13 patients had received cognitive behavior therapy or other psychotherapy before the present study. The study was approved by the local institutional review board, and written informed consent was obtained from all subjects after the procedures had been fully explained.
Clinical Assessments
OCD symptom severity was measured by using the Yale-Brown Obsessive Compulsive Scale. The Hamilton Depression Rating Scale, the Beck Depression Inventory, and the Beck Anxiety Inventory were also administered both before and after pharmacotherapy.
MR Acquisition and Processing
Three-dimensional T
1 -weighted MRI and
1 H-MRSI scans were performed on the same day at the Kangbuk Samsung Hospital; a 1.5-T MR scanner (Philips Medical Systems, Best, the Netherlands) was used. First, an axial three-dimensional T1 fast field echo sequence was used to obtain 150 1.0-mm contiguous axial images from the entire brain (overlapping slices, repetition time [TR]=25 msec, echo time [TE]=6.9 msec, flip angle=40°, acquisition matrix=256×256, field of view=240 mm×240 mm). Axial sections were acquired parallel to the anterior commissure-posterior commissure line.
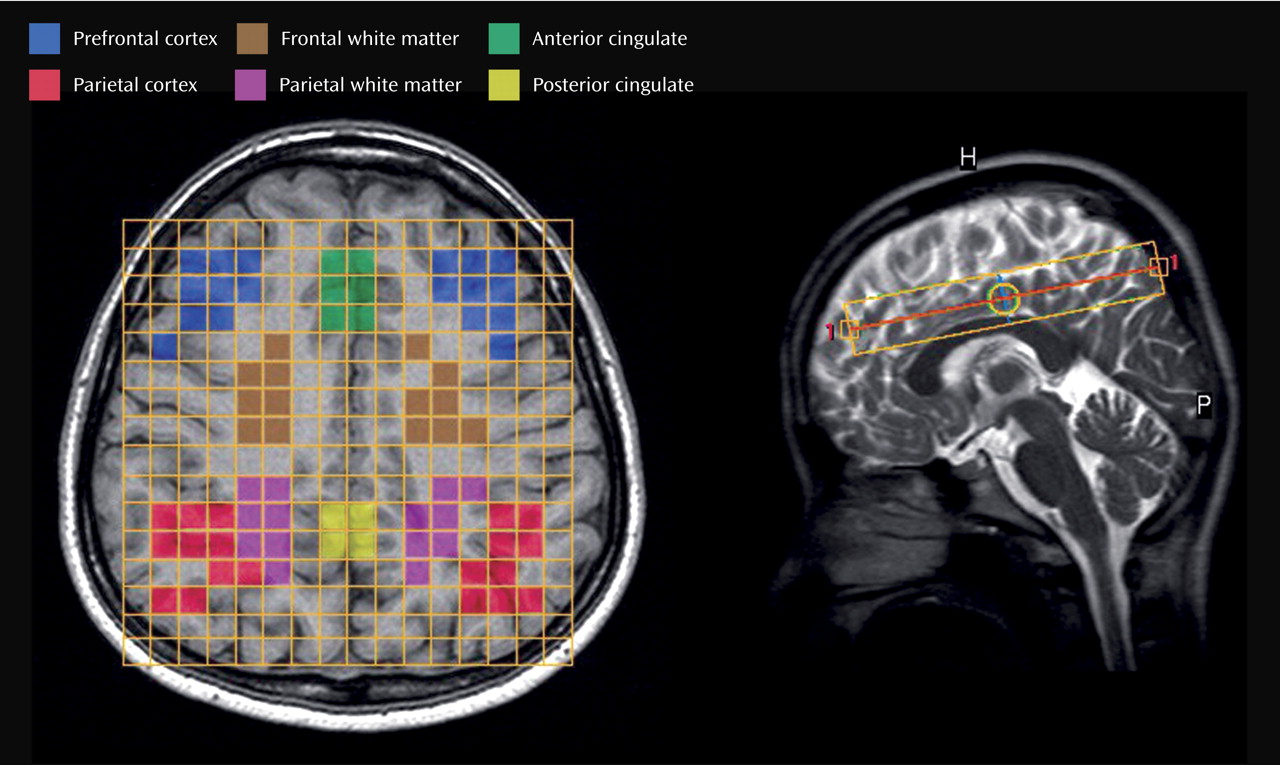
1 H-MRSI data were acquired by using a point resolved selective spectroscopy (PRESS) sequence with outer volume suppression (TR=2000 msec, TE=272 msec). One slice (thickness: 20 mm) was chosen for spectroscopy in which, according to the consensus of two investigators (J.H.J., J.S.K.), the cingulate regions were most included (
Figure 1, right). The field of view was 12 cm×12 cm for the slice; combined with 16×16 phase encoding. Voxel dimensions were 7.5 mm×7.5 mm×20 mm. The signal was digitized with 256 points and a 1000 Hz spectral width.
First, we drew regions of interest on the T
1 -weighted coaxial MR images. Boundary definitions were performed as described by Crespo-Facorro et al.
(6) and Bokde et al.
(7) . In order to select the regions of interest, the volumetric MRI data were segmented into gray matter, white matter, and CSF components, using a fuzzy C-means algorithm
(8) . Then, we classified each voxel of MRSI data into white matter when the exact same voxel location for volumetric MRI consisted of >80% white matter, and into gray matter when the exact same voxel location for volumetric MRI consisted of >50% gray matter (
Figure 1, left). Finally, the quantification of
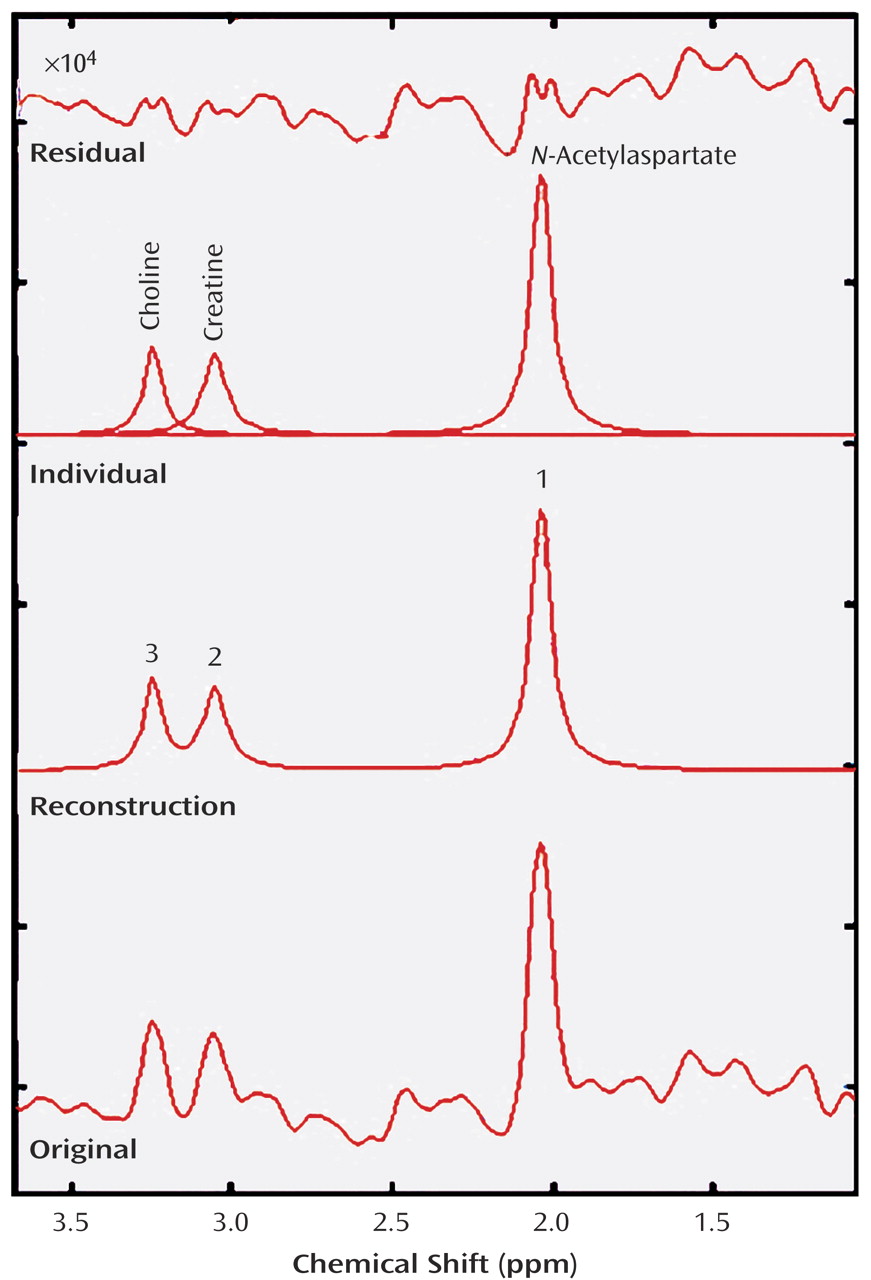
N -acetylaspartate, creatine, and choline were measured by the MRUI package (Leuven, Belgium) in each region of interest (
Figure 2 ). In order to ensure high-quality data, spectra were rejected if the resolution between the choline and creatine peaks was not at least 50% of the distance from the peak maximum to the apparent baseline. Levels of
N -acetylaspartate were measured in terms of ratios with creatine, choline, and creatine plus choline.
Pharmacotherapy
After completion of clinical assessments and the baseline 1 H-MRSI scans, citalopram (an approved medication for OCD in Korea) treatment was started at 10 mg/day and titrated up to 60 mg/day by the 6th week, increasing by 10 mg every week. It was then maintained at 60 mg/day until the end of the 12-week pharmacotherapy regimen. Patients received no medications other than citalopram and were not engaged in cognitive behavior therapy or psychoanalytic psychotherapy. Effects and side effects were evaluated every 2 weeks. None of the patients experienced clinically significant side effects during the course of the study, and all patients completed the procedures and evaluations after the 12-week pharmacotherapy; there were no dropouts.
Statistical Analyses
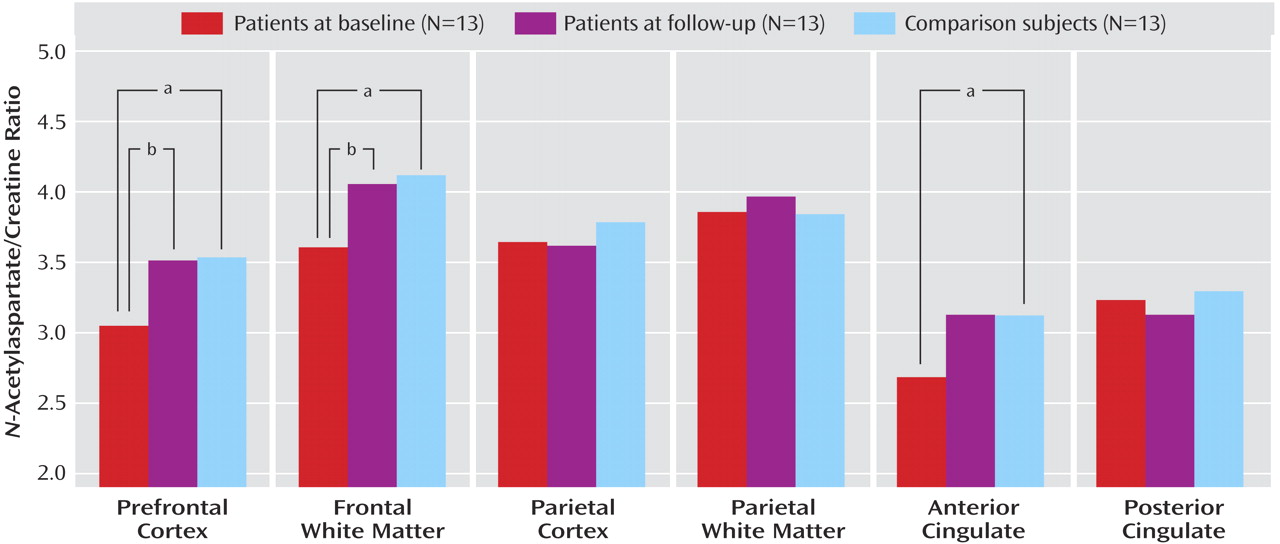
Analyses of variance (ANOVAs) were performed with least significant difference post hoc tests to examine for significant differences in the N -acetylaspartate ratios between comparison subjects and OCD patients and in OCD patients before and after citalopram treatment.
Paired t tests were employed to compare pretreatment versus posttreatment scores on the Yale-Brown Obsessive Compulsive Scale, Hamilton depression scale, and Beck anxiety and depression inventories in OCD patients, while independent t tests were used to compare OCD patients and comparison subjects with regard to baseline demographic measures. A level of p<0.05 was considered to be significant.
Discussion
To our knowledge, this is the first 1 H-MRS study demonstrating abnormalities in N -acetylaspartate levels in adult drug-naive OCD patients and the first study to address the effects of citalopram treatment on N -acetylaspartate levels in this illness.
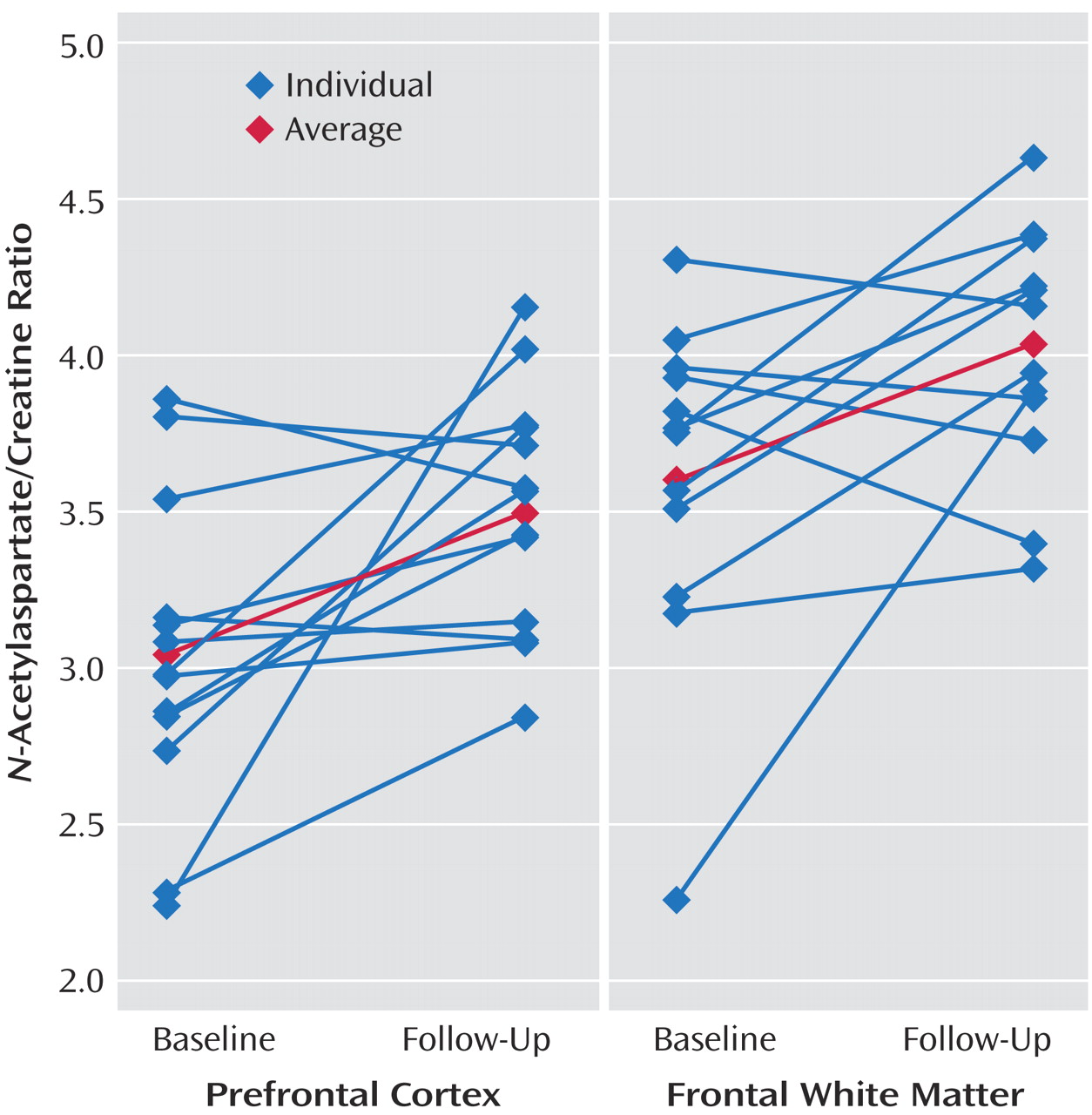
Decreased baseline N -acetylaspartate levels in the frontal white matter, prefrontal cortex, and anterior cingulate were selectively increased by citalopram treatment. Citalopram treatment had no effect on N -acetylaspartate levels in any of the other regions, namely, the posterior cingulate or parietal regions. Also, our findings do not appear to reflect effects of time. In six comparison subjects, we measured neurochemicals twice (a baseline measurement with follow-up 12 weeks later), and no significant differences were detected in any 1 H-MRS measures. This suggests that 1 H-MRS measures remain stable, at least during a 12-week period, and it is highly probable that the N -acetylaspartate concentration changes seen in OCD patients were attributable to pharmacotherapy.
The physiological role of
N -acetylaspartate in neurons has yet to be fully elucidated. In the mature brain,
N -acetylaspartate is found almost exclusively in neurons, and in the highest concentrations in the pyramidal glutamatergic neurons
(9,
10), and
N -acetylaspartate synthesis is dependent on glutamate and pyruvate or 3-hydroxybutyrate
(11) . In recent studies, it has been determined that
N -acetylaspartate is an intracellular osmolyte, and functions as a storage substrate for brain aspartate and acetate
(12,
13) . It has also been proposed that the
N -acetylaspartate cycle functions as a neuronal mechanism for the removal of large amounts of metabolic water generated in the performance of interneuronal and intercellular signaling tasks
(14) . Some
1 H-MRSI studies have also reported a positive correlation between cerebral glucose metabolic rates and
N -acetylaspartate concentrations
(15,
16) .
N -Acetylaspartate concentration varies with the structural and functional state of the neuronal cells and is associated with various pathologic conditions involving neurons
(17 –
19) . All of these studies suggest that
N -acetylaspartate concentration represents not only neuronal density, but also the metabolic status of neurons
(19) .
In positron emission tomography studies conducted with OCD patients, abnormal glucose metabolism or cerebral blood flow has been reported to occur in the prefrontal area (especially, the orbitofrontal cortex), anterior cingulate, thalamus, and caudate
(20 –
23) . These abnormal activities have all been demonstrated to be normalizable by pharmacotherapy
(24 –
26) . The results of the present study are consistent with those of previous studies.
In contrast to the results of the current study, Rosenberg et al.
(27) found no significant reductions in
N -acetylaspartate level in the anterior cingulate of drug-naive pediatric OCD patients. The difference may be due to the fact that the duration of illness in their study (mean=3.87 years) was too short to cause a significant difference in
N -acetylaspartate levels. In a study of adult OCD patients whose mean duration of illness was 11 years (SD=7 years)
(4), significantly lower
N -acetylaspartate levels were observed in the anterior cingulate. Russell et al.
(28) observed an increase in
N -acetylaspartate in the left but not right dorsolateral prefrontal cortex in pediatric OCD patients (8–15 years of age) relative to comparison subjects. This result is contrary to our study. This might be due to the differences of methodology (differences of regions of interest selection, measuring ratios versus absolute concentrations, MRSI versus single voxel) or subjects. Russell et al. suggested that increased left dorsolateral prefrontal cortex
N -acetylaspartate may represent neuronal hypertrophy or hyperplasia in pediatric OCD patients.
There are several limitations of this study. First, the group sizes were small. The lack of correlation between clinical measures and N -acetylaspartate levels may be due, at least in part, to the small group sizes. Second, we used the ratios of N -acetylaspartate to other neurochemicals as a form of normalization. Although this approach controls for the variances associated with assay irregularities, it is potentially less sensitive to changes affecting multiple metabolite signals. Thus, when we made a description of “changes in N -acetylaspartate levels,” we cannot exclude the possibility that the results of the current study were affected by changes in creatine or choline concentrations. Third, in the current study, the OCD patients were drug-naive at baseline period and had taken only citalopram. For this reason, it is difficult to speculate as to whether our results would be applicable to patients who are taking other medications or undergoing cognitive behavior therapy.