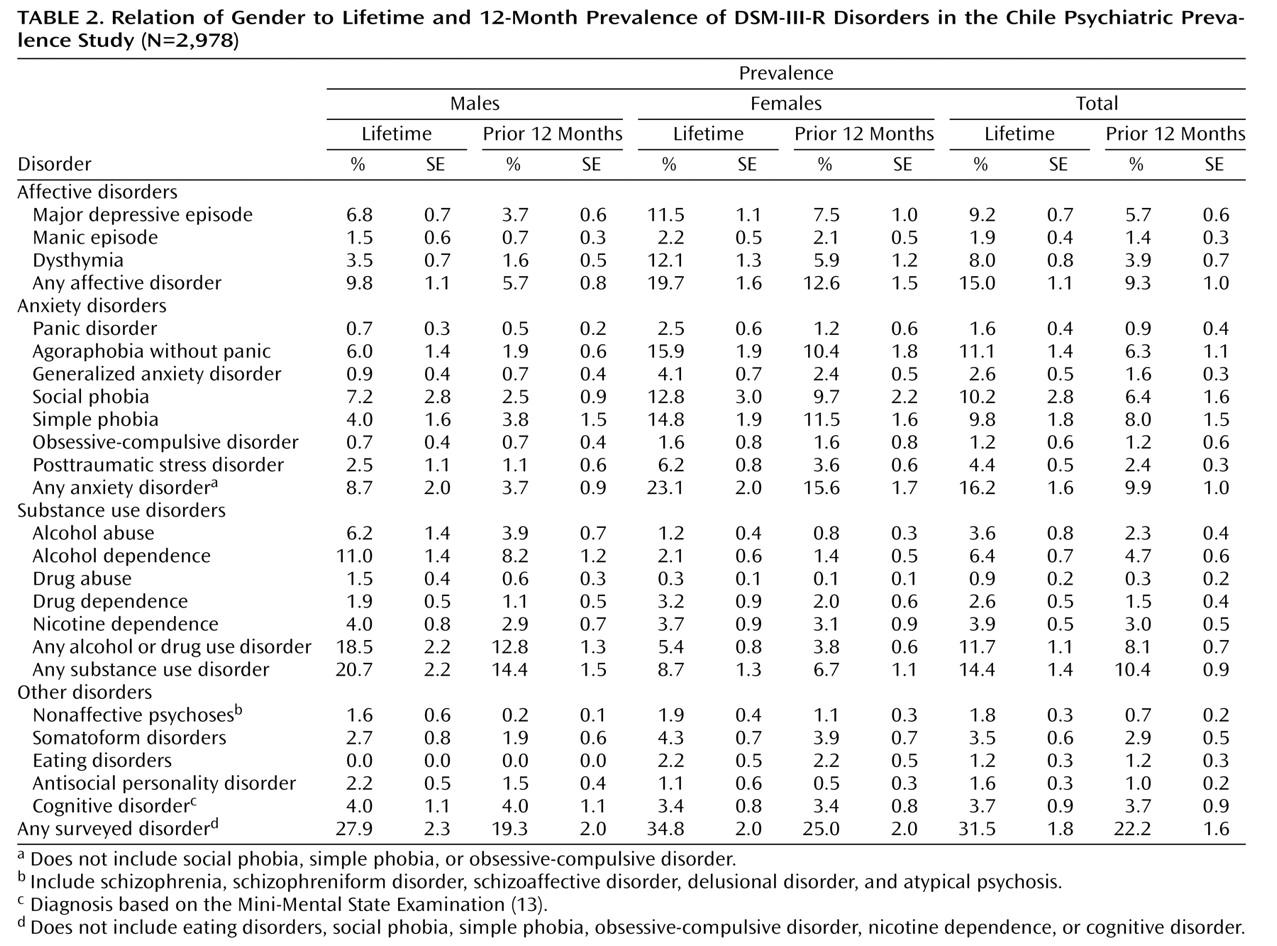
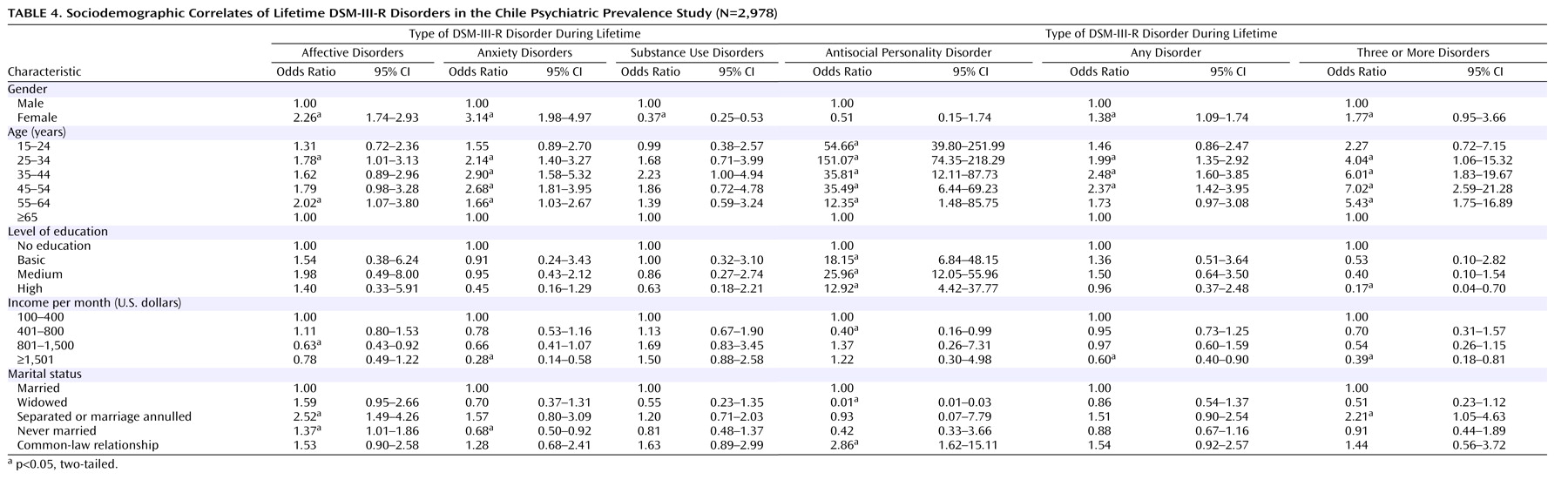
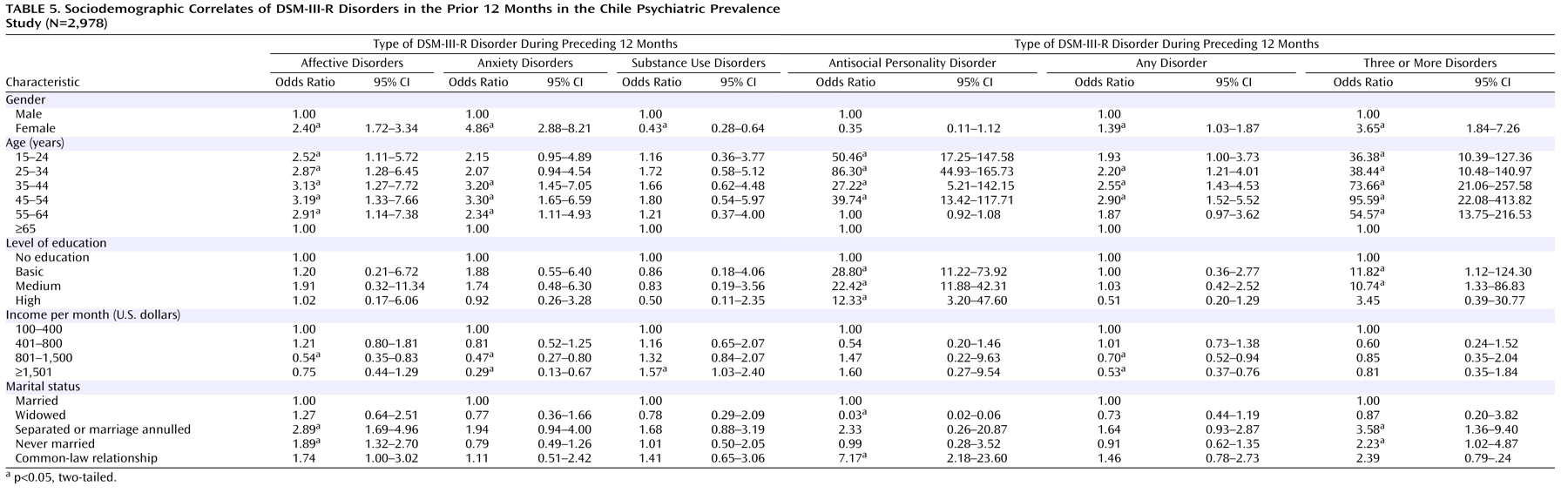
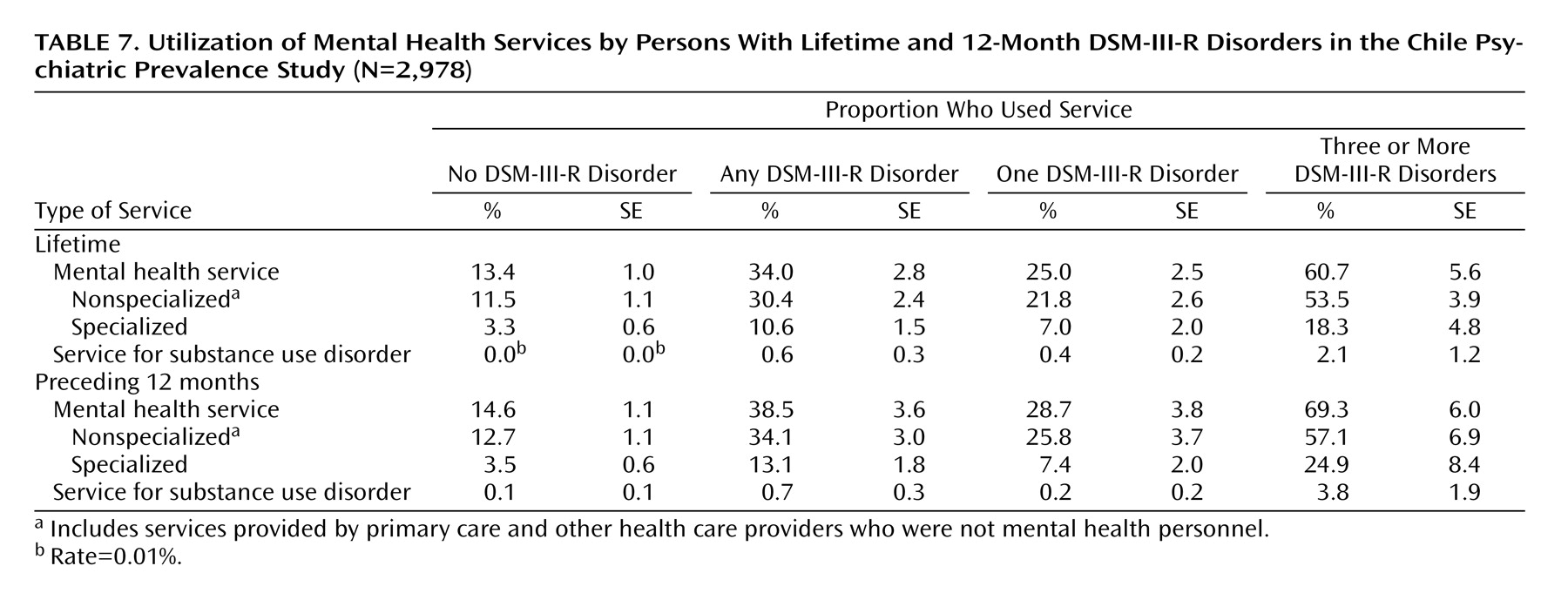
The Chile Psychiatric Prevalence Study survey is one of only a few psychiatric epidemiological prevalence studies of a nationally representative sample in a Latin American country. To our knowledge, it is the first to use appropriate statistical procedures to correct for the sampling design and weights to ensure that the sample is representative of the national population. Approximately one in three individuals in the population had a lifetime psychiatric disorder in Chile, and over one-fifth had a disorder in the past 12 months. The five most common lifetime psychiatric disorders were agoraphobia, social phobia, simple phobia, major depressive disorder, and alcohol dependence. For men the most common disorder was alcohol abuse or dependence, while for women it was an anxiety disorder. Nearly one-third of those with a 12-month prevalence diagnosis had a comorbid psychiatric disorder. The majority of those with comorbidity had sought out mental health services, but only one-quarter of those without comorbidity had done so.
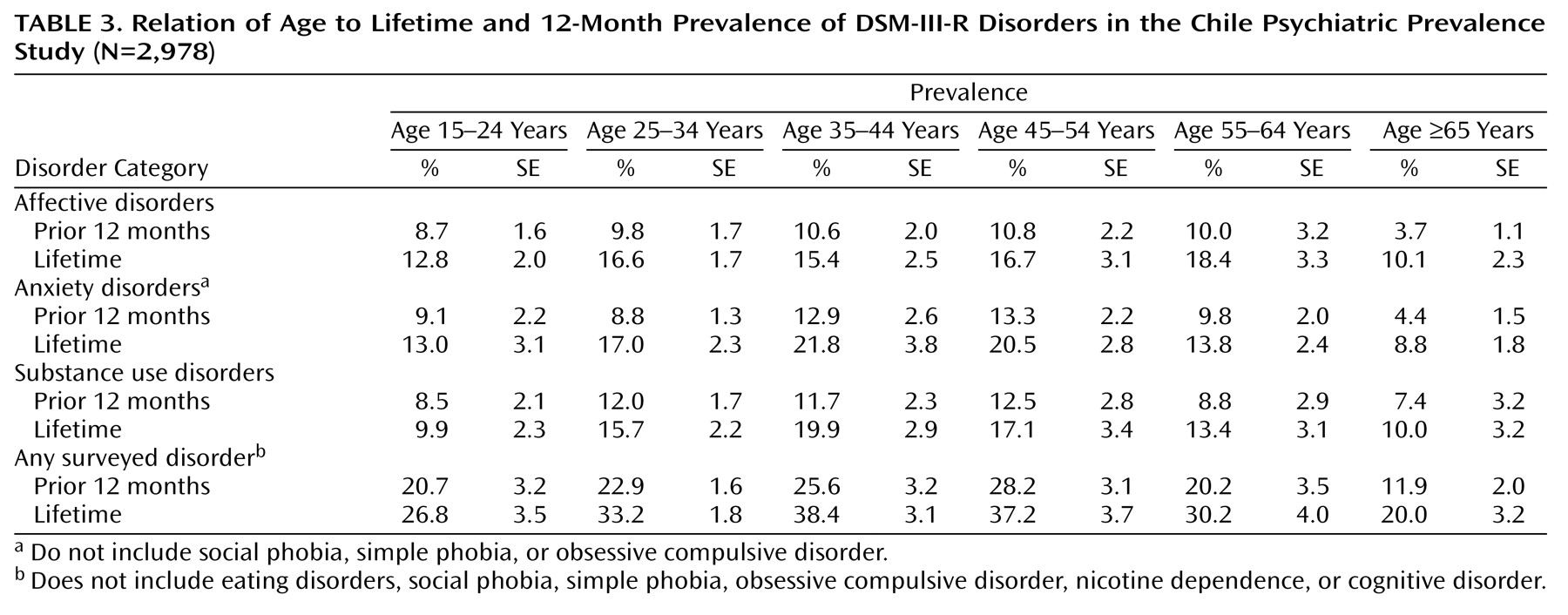
This survey suffers from the same limitations as most other cross-sectional psychiatric prevalence studies. First, the lifetime prevalence rates are based on retrospective reports. Second, the diagnostic assessments relied on the CIDI, which is an interview administered by nonclinicians. In addition, the sample size may not yield enough power to examine risk factors for the less common psychiatric disorders. The lower prevalence of disorders in the elderly, as found in most other epidemiological studies, might be due to a cohort effect, reporting bias, or differential mortality of those with a disorder. The assessment of cognitive impairment was limited to items from the Mini-Mental State Examination
(13) and did not include a formal diagnosis of dementia, the most common mental disorder of late life. The interviews conducted in the four catchment areas representing the Chile Psychiatric Prevalence Study were not completed at the same time but, rather, over 7 years. This, unfortunately, is a reflection of the difficulty of obtaining consistent funding to conduct research in developing countries.
The findings from the Chile Psychiatric Prevalence Study are by and large similar to those found among other Hispanic populations.
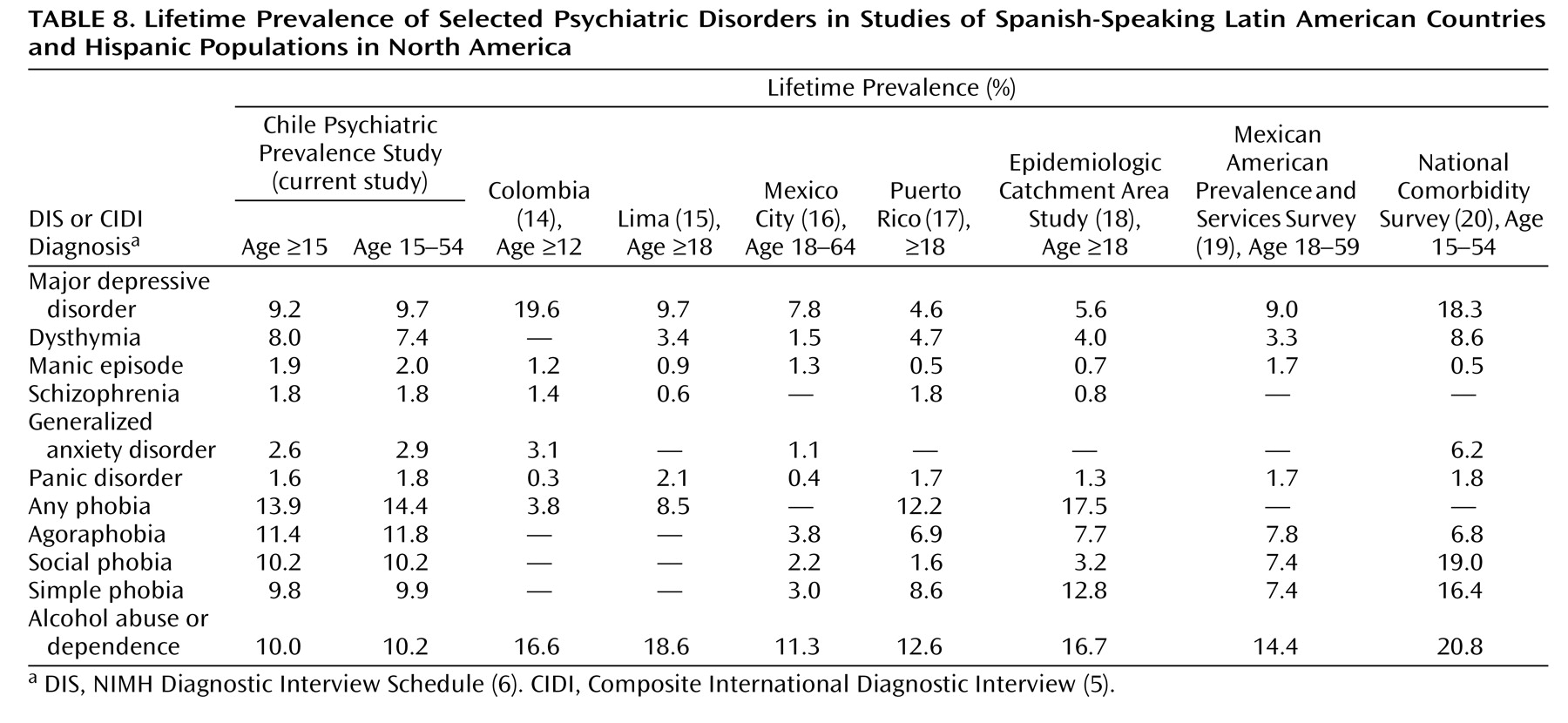
Table 8 provides a comparison of the current results with the findings from other published studies that used the DIS or CIDI to determine lifetime prevalence rates in Spanish-speaking Latin American countries and Hispanic populations in North America. In contrast to that found among Hispanics in the National Comorbidity Survey
(20) in the United States, the rate of major depression in the Chile Psychiatric Prevalence Study, for ages 15–54, was considerably lower, 9.7%, compared to 18.3%, and the rate of alcohol use disorders was also lower, 10.2% versus 20.8%. It is conceivable, but unlikely, that this could be fully explained only by differences in methods, such as the use of additional probes in the National Comorbidity Survey. Except for Colombia
(14), all of the other studies had similar rates for major depressive disorders. In the Colombia study, dysthymia was not considered as a diagnosis, and those individuals may have been included among those with major depression, accounting for the difference in rates. The higher rate of alcohol use disorders in Colombia may be due to the fact that they were identified by using the CAGE
(21) as a screening instrument, while the rates in the Lima study
(15) may reflect the lower socioeconomic status of the sample. The three studies of Hispanics in the continental United States
(18 –
20) consistently show higher rates of alcohol use disorders than were found in the South American surveys. The rate of anxiety disorders in Chile was higher than that for major depression, a finding noted in some but not all studies of Hispanic populations. The low rate of comorbidity in the Chile Psychiatric Prevalence Study was also noted in the Mexico City CIDI study
(16), in marked contrast to the National Comorbidity Survey, in which comorbidity was the norm
(20) . Rates of service utilization in the United States
(22), Mexico
(16), and Chile did not appear to differ widely. Although such cross-national comparisons are crude because of differences in methods across studies, with the inclusion of the current study a general picture of the prevalence of psychiatric disorders in Latin America is now emerging.
The importance of mental illness in disability and utilization of health care services in Latin America, although increasing, is not yet fully appreciated. Psychiatric epidemiological surveys are a means of providing data to authorities in a position of allocating resources to address the developing crisis in mental health anticipated in Latin America as the epidemiological transition continues
(2) . Future studies, however, will need to focus more on service utilization needs, the presence of medical comorbidity, prevalence rates for serious mental illnesses, and measures of disability.