There has been little research in this field from the developing world. The lack of resources and the high prevalence of depression and its close association with poverty have created a rather nihilistic view about the treatment of depression in the developing world. Recent research challenges this view, however. An Indian study showed improvements with antidepressants at 2 months
(18), and a study in Uganda found that group interpersonal therapy alone delivered by trained local health workers was effective at 6 weeks
(19) . These studies show that some improvements can be achieved even with limited resources and when treating extremely deprived populations.
Results
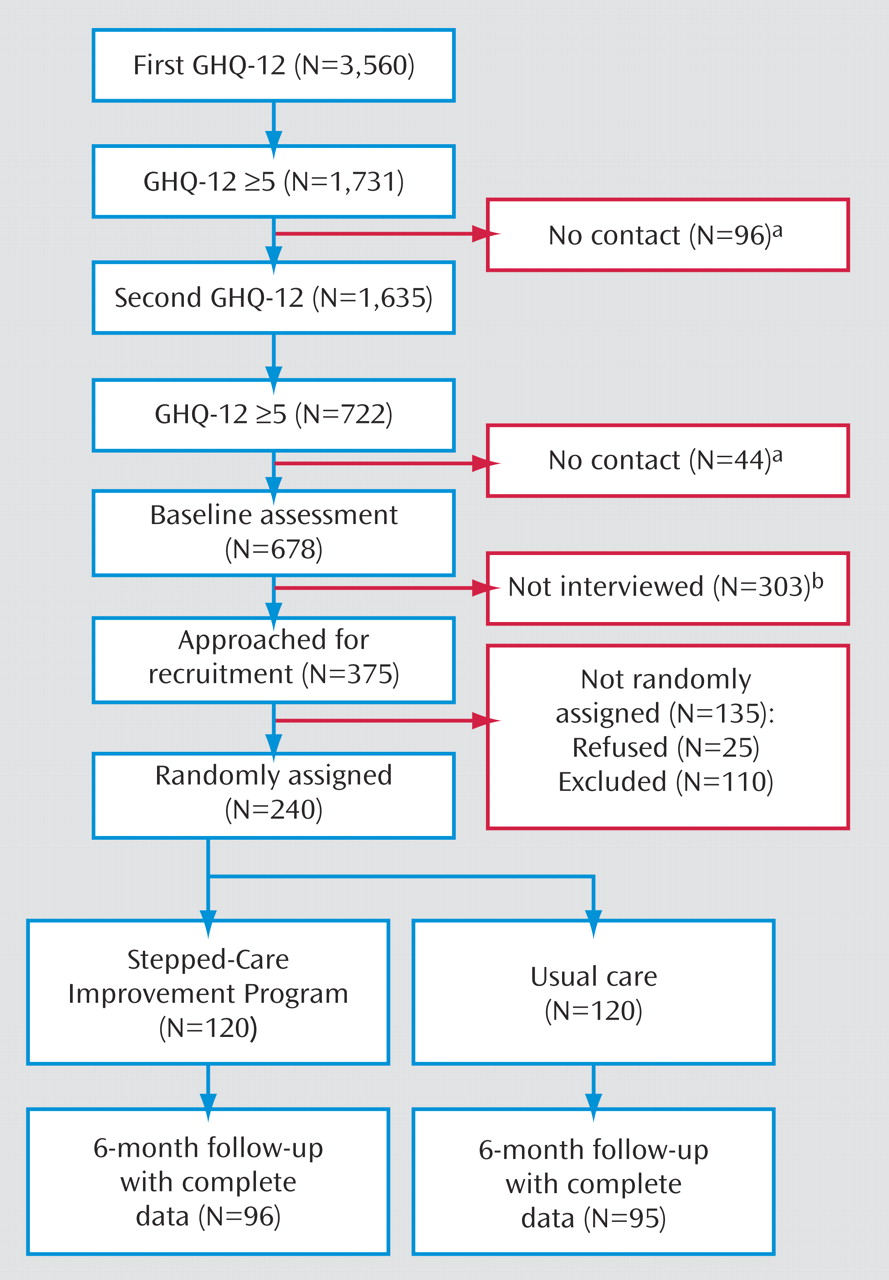
Approximately one out of five patients was identified as potential cases after screening. All of them were sent appointments for baseline assessments, but only 375 were interviewed before completing recruitment of 240 women needed for the trial. Of the 135 women who were not included, 110 did not meet DSM–IV criteria for major depression. Patients who received baseline interviews had similar scores on the 12-item General Health Questionnaire than those who were not interviewed
(20) (
Figure 2 ).
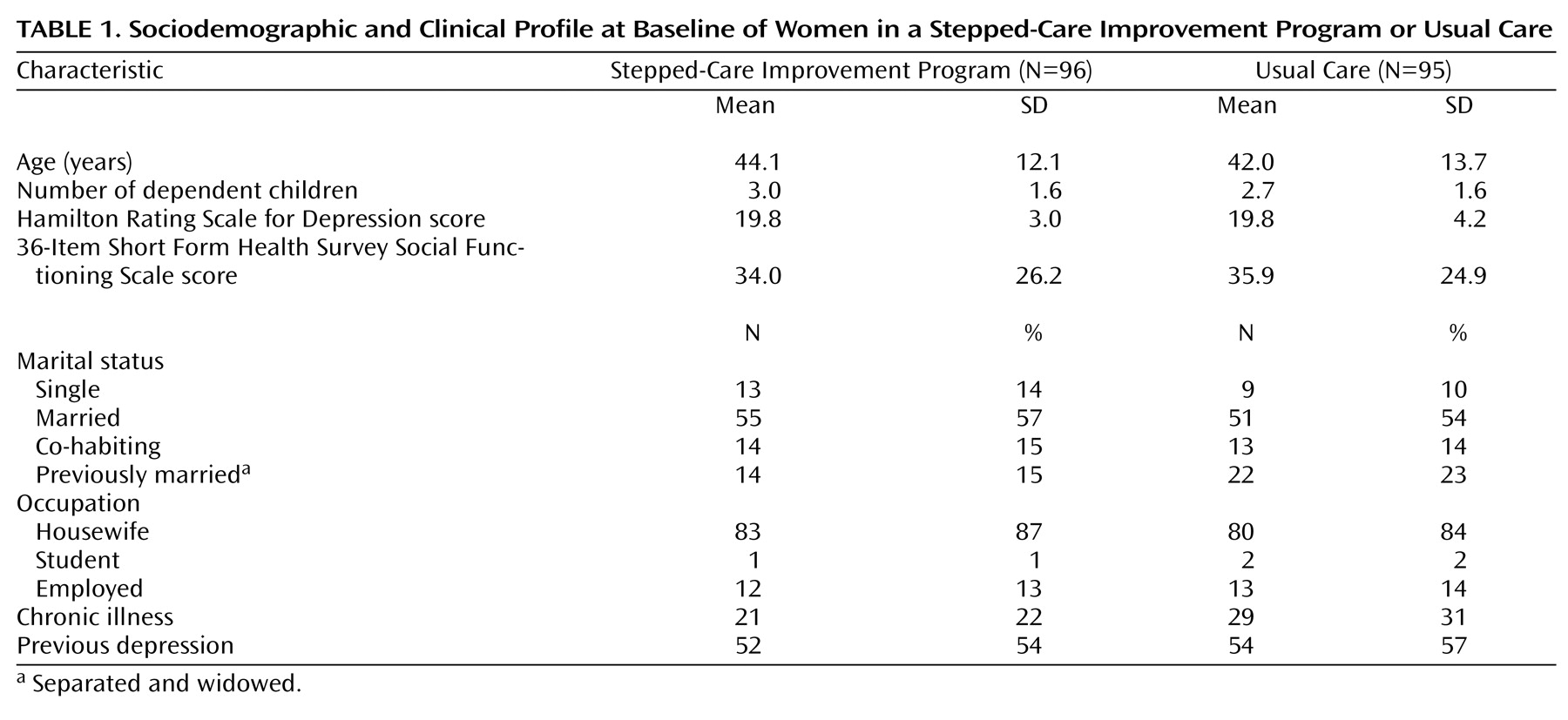
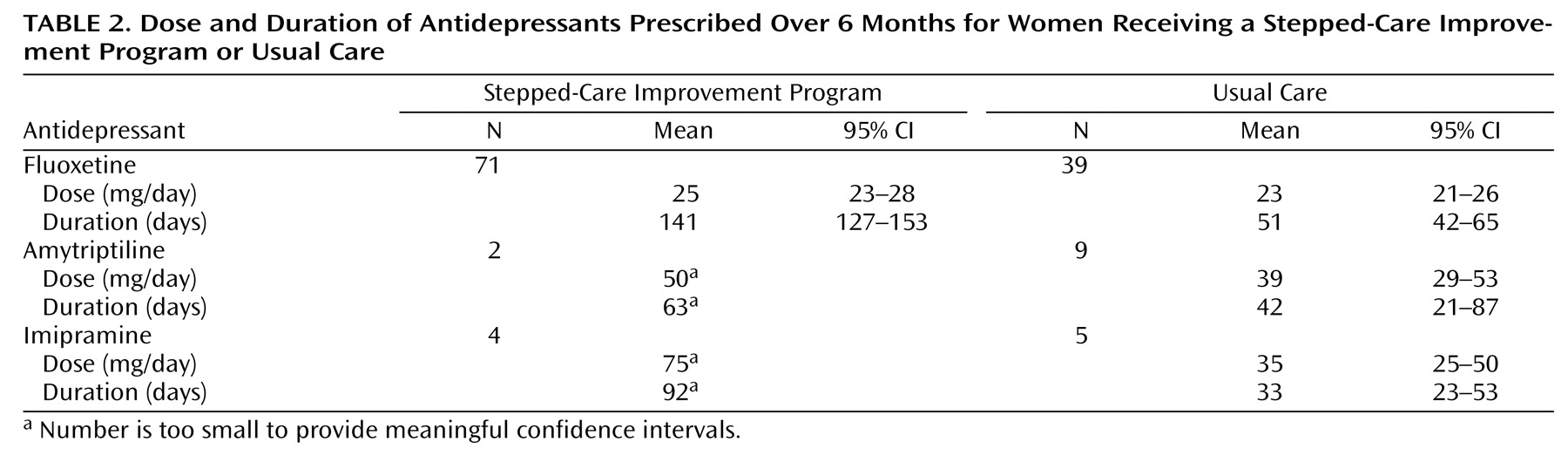
Table 1 shows that those patients who were randomly assigned to usual care and the stepped-care improvement program and included in this analysis were similar in demographic and baseline clinical characteristics. The great majority were married housewives with average Hamilton depression scale scores, suggesting moderate to severe depression with high levels of social dysfunction. Of those assigned to the stepped-care improvement program, the mean number of sessions attended was 7.27 (CI=6.76–7.78). There were notable differences in the proportion of women receiving medication, the dosage, and duration (
Table 2 ). In the stepped-care improvement program group, 80% (N=77 of 96) of patients received antidepressants, compared with 56% (N=53 of 95) in the usual care group. Generally speaking, patients in the stepped-care improvement program received similar doses of antidepressants, with the exception of imipramine, but for a much longer duration. A much larger proportion of women were receiving benzodiazepines in the usual care group (45% [N=43 of 95] versus 13% [N=12 of 96]), but the length of time on the drug was similar in both groups (30 days [95% CI=28–33] versus 31 days [95% CI=23–40]).
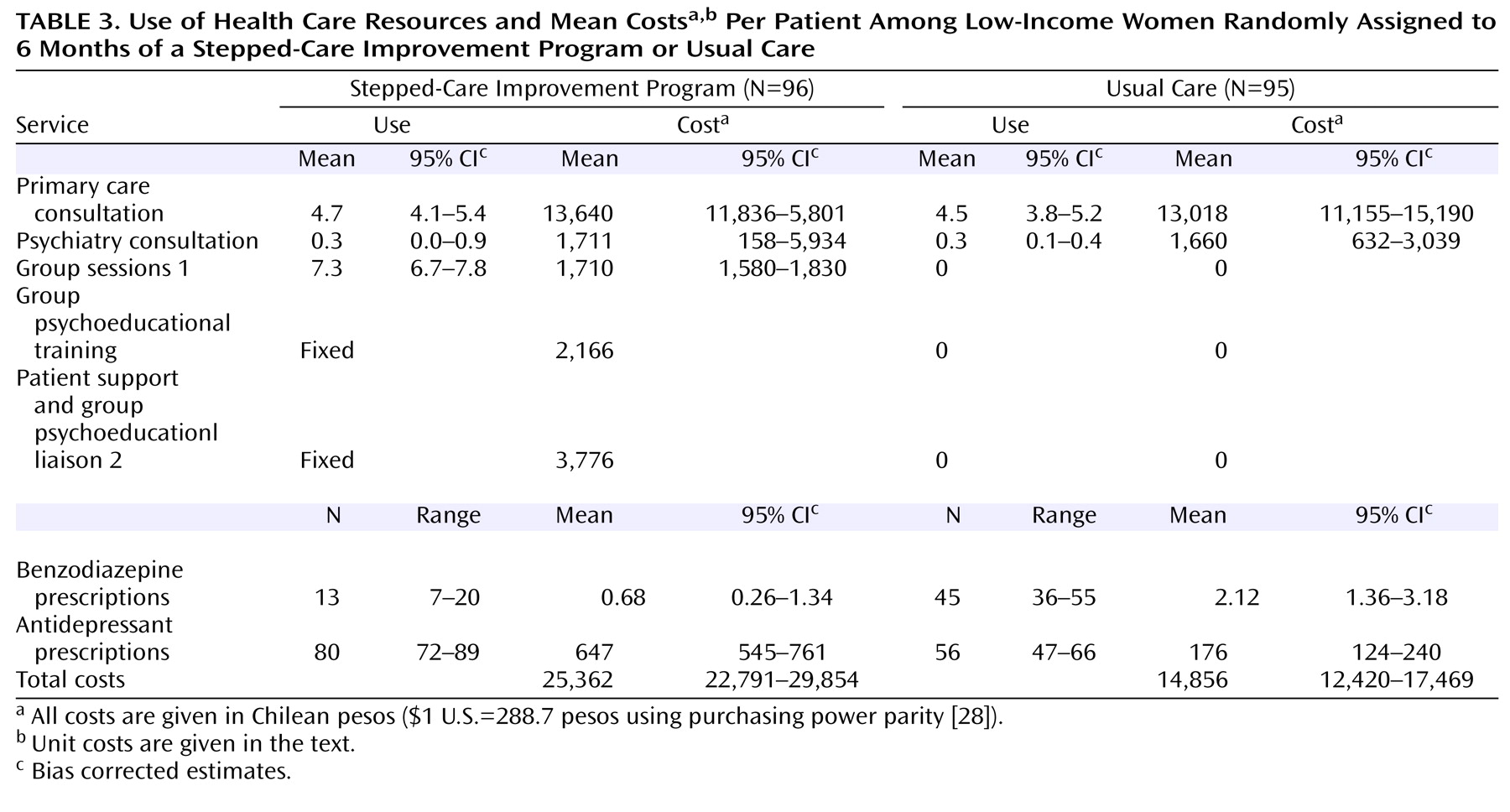
The mean (unadjusted) costs obtained with bootstrapping for the two groups is shown in
Table 3 . Additional costs for the stepped-care improvement program were mainly concentrated on group intervention, liaison with doctors, and antidepressants. The mean number of medical consultations was similar in both groups. At 6 months, total costs in the stepped-care improvement program were approximately 40% higher than for the usual care group.
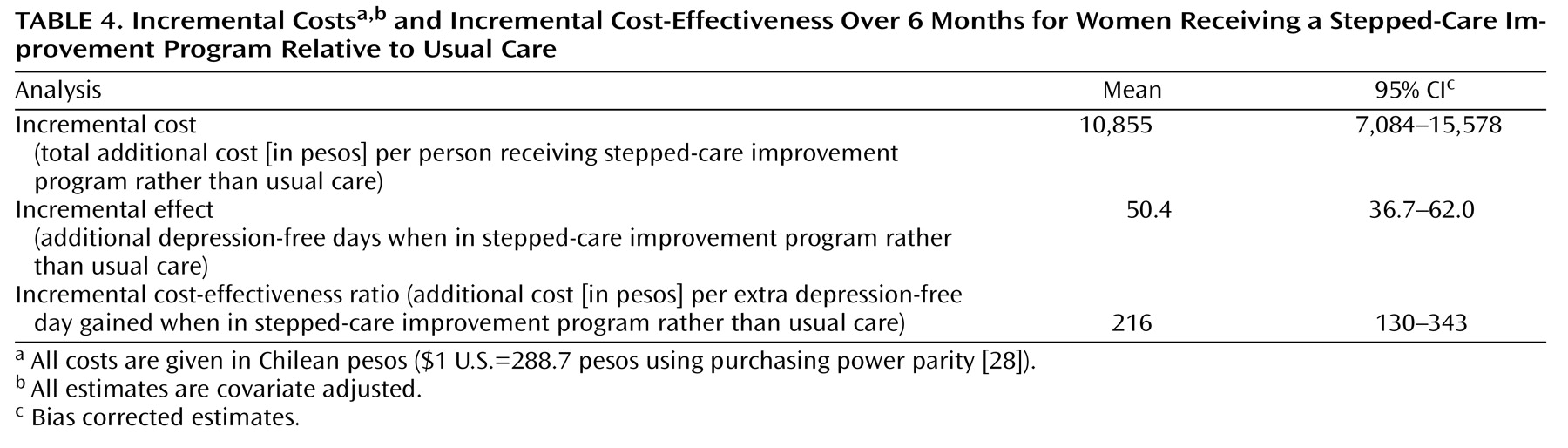
Table 4 displays the covariate-adjusted difference in depression-free days and cost-effectiveness. The stepped-care improvement program group achieved 50 more depression-free days than the usual care group after adjusting results for age, presence of chronic disease, and initial severity. This improved clinical outcome in the stepped-care improvement program group was achieved at an additional cost of 10,855 pesos ($37.6 U.S.) per person over and above the costs of usual care. The incremental cost-effectiveness ratio for the stepped-care improvement program relative to usual care was 216 pesos ($0.75 U.S.). In other words, the stepped-care improvement program was more costly but also more effective, with a cost of 216 pesos to obtain an extra depression-free day, relative to usual care.
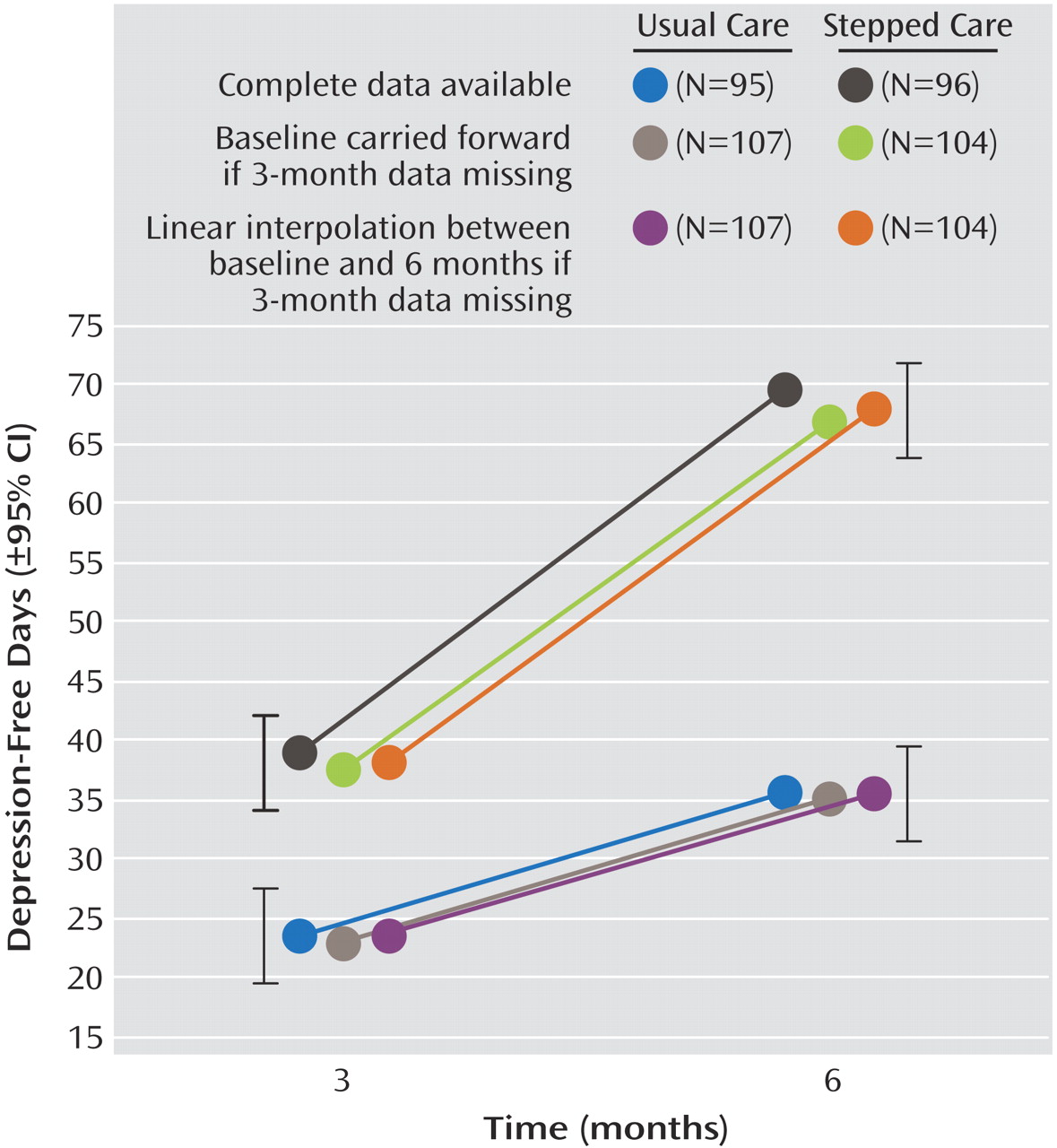
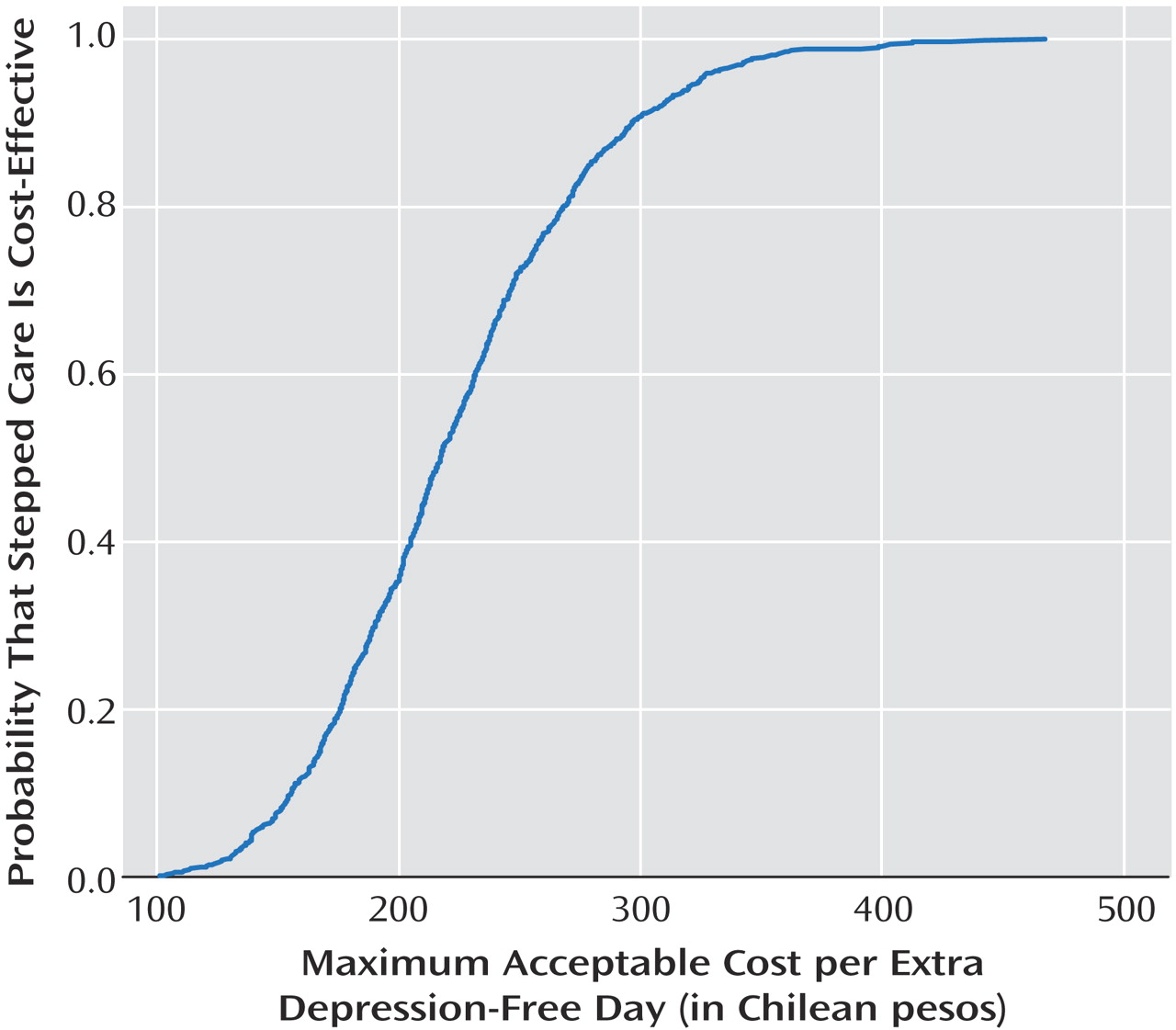
We conducted some sensitivity analysis to explore the impact of missing data. We replaced missing cost data using extreme values (lowest and highest value) and ran models with complete clinical data (N=197) and with missing clinical data replaced with the last observation carried forward (N=211). When using complete clinical and cost data (N=197), the incremental cost-effectiveness ratios per extra depression-free day fluctuated between 173 pesos (range: 67–278) and 236 pesos (range: 126–347). When using data sets with replaced missing clinical and cost data (N=211), the incremental cost-effectiveness ratios varied between 169 pesos (range: 63–275) and 245 pesos (range: 134–357). The cost-effectiveness acceptability curve for all these models showed similar patterns, with a 90% probability of a cost-effective stepped-care improvement program at 300 pesos ($1.04 U.S.).
Figure 3 shows the cost-effectiveness acceptability curve for the complete data obtained from bootstrap estimates of the incremental cost-effectiveness ratio. When the 1,000 bootstrap estimates of cost-effectiveness were ranked, there was a 90% probability that the incremental cost of obtaining an extra depression-free day by introducing the stepped-care improvement program would not exceed 300 pesos.
Discussion
To our knowledge, this is the first successful randomized controlled trial of a stepped-care program for the treatment of depression in primary care from a developing country. Our program was significantly more effective than usual care, and this was achieved with modest cost increases. A national program based on our intervention has now been introduced in Chile, turning this study into one of the few examples of research assisting a major mental health policy decision in the developing world.
Our analyses were restricted to 6 months. Several U.S. studies
(11,
13,
37) suggest that the costs of improved depression care tend to occur early and benefits continue to accrue. Cost-effectiveness ratios may be more favorable over periods of 12 months or longer. It is impossible to completely rule out some contamination between the groups, but other similar U.S. studies have found little evidence in support of this
(38,
39) and, even if it was present, it would have reduced the differences between the groups. There are difficulties when comparing cost-effectiveness studies across countries because of differences in treatments, unit costs, resources, and so on. However, common clinical outcomes, such as depression-free days, allow for some cautious comparisons. The women in our stepped-care improvement program achieved 50 incremental depression-free days over 6 months, relative to women in the usual care group, which compares favorably with the increments of 17 depression-free days or less seen in similar U.S. studies
(13) . Comparisons across countries are often of little interest for local decision making; more important seems to be the cost-effectiveness of a program in relation to local needs, resources, and political climate.
We feel that our stepped-care improvement program involved a modest increase in costs relative to usual care. Incremental costs per an extra depression-free day with the stepped-care improvement program were 216 pesos, and there was a 90% probability of achieving an extra depression-free day for 300 pesos, which is equivalent to the cost of a one-way bus fare in Santiago. We feel that the relatively low costs of our program might have been influenced by the following:
1. Delegating as much responsibility as possible to nonmedical health workers who are paid lower wages. Enlarging the role of these workers is something that developing countries have been practicing for a long time
(40) .
2. Using a group intervention rather than costly individual therapies supplied by well-trained professionals. There is little research on group interventions for depression in primary care in the more developed world, and, when tried, attendance has been poor
(41) .
3. Choosing lower-cost antidepressants without affecting effectiveness. Fluoxetine is out of patent status, and its market price is fairly low in most developing countries
(18) .
One of the most striking differences between the groups in our study was the less frequent use of antidepressants in the usual care group and, when prescribed, the shorter duration. Incidentally, physicians in both groups received similar treatment guidelines and training at the onset of the study, which is further evidence that guidelines alone are not sufficient to improve treatment practices or outcome
(42) . We were unable to establish with clarity the relative contribution of each treatment component, although our analysis suggests that antidepressants and the number of group sessions seem to have made independent contributions to recovery
(20) .
It is likely that systematic follow-up, active engagement, and support might have also contributed to the recovery rates, as found in a similar U.S. study
(4) . The likelihood of achieving clinically significant results is higher with multicomponent programs, something that must not be underestimated when local decision makers are skeptical on the merits of investing more resources toward treating depression. It is also important to recognize that treatment often involves the use of more than one component in routine clinical practice. Thus, the evaluation of practical multicomponent interventions is probably of greater importance to service providers and policy makers than the dissection of specific treatment components.
In a number of developed countries, such as the United States, there are some agreed upon thresholds ($50,000 per quality adjusted life years gained
[43] ), suggesting that it could be worthwhile to invest in an intervention. However, no such thresholds have been estimated or agreed upon in Chile, and it would be unreasonable to extrapolate thresholds across countries with clearly different socioeconomic development levels. Nonetheless, a simple calculation could shed some light onto the possible costs in Chilean pesos per quality adjusted life years gained. For instance, if we estimated that recovery from fully symptomatic depression to full remission is associated with a health utility gain of 0.2 to 0.4
(44,
45), then our cost-effectiveness ratio of 216 pesos per depression-free day would translate into a ratio of between 197,100 pesos ($683 U.S.) to 394,200 pesos ($1,365 U.S.) per quality adjusted life years gained.
Scientific knowledge tends to travel more easily from the developed world to the developing world. However, it is possible that something could be learned from studies using simple interventions with less intensively trained personnel
(46) . Some of the lessons learned from this are as follows:
1. There is no good reason to hold nihilistic views about the treatment of depression with deprived populations; these are precisely the groups that have the most to gain with modest investments to improve the treatment of depression as demonstrated in countries with various levels of development
(4,
19) .
2. It is possible to deliver affordable yet successful multicomponent stepped-care programs in poorer and richer countries.
3. Engaging patients and providers in a course of effective treatment seems to be essential, especially in deprived populations
(4) . In keeping with this, nonmedical health care workers, in our study, were responsible for systematic follow-up of patients as well as regular liaisons with treating physicians.
4. Some effective mental health interventions can be delivered in groups, which are also seen in studies for other health problems in the developing world
(47,
48) .
In resource-poor settings where there is little to treat depression, testing simple and inexpensive interventions might be more acceptable for people than in countries accustomed to more choices. The diversity in populations, health systems, resources, costs, or treatments across countries may conspire against the generalizability of findings, but these differences have not been an impediment for developing countries to learn from the experiences of the developed world.