The contribution of drugs of abuse to the human immunodeficiency virus (HIV) epidemic has been traditionally associated with the use of contaminated needles by injecting drug abusers
(1) . However, increased risk for HIV infection also occurs in noninjection drug users
(2) . Facilitation of risky sexual behaviors during drug intoxication appears to be another mechanism by which drugs of abuse contribute to the HIV epidemic as well as to other sexually transmitted diseases
(3) . Indeed, the recent methamphetamine epidemic, which has led to a significant increase in HIV seroconversion among injecting as well as noninjecting abusers (particularly among homosexual men), highlights the importance of this mechanism
(4) . The mechanisms underlying facilitation of risky sexual behaviors during intoxication with stimulant drugs are not properly understood, but they could reflect impairment in self-control (disinhibition) and/or increases in sexual desire. Although preclinical studies have shown that stimulant drugs (including amphetamine, methamphetamine, and cocaine) increase sexual behavior (review
[5] ) and drug abusers report that they become more sexually excited when on stimulant drugs
(6), this has not been properly evaluated in humans. In this study, we evaluated the effects of the stimulant drug methylphenidate when administered intravenously on “sexual desire” of healthy comparison subjects and of cocaine abusers. The drug methylphenidate was chosen, since it is pharmacologically similar to cocaine
(7), and cocaine abusers report the effects of intravenous methylphenidate to be similar to those of intravenous cocaine
(8) . Moreover, as for methamphetamine, the abuse of cocaine is also associated with increases in risky sexual behaviors
(9) . However, we recognize that methylphenidate, which is a drug that, like cocaine, increases dopamine by blocking dopamine transporters
(9), is a weaker stimulant than methamphetamine, which is a drug that increases dopamine by releasing dopamine from the terminals
(10) .
For this purpose, we performed secondary analysis on behavioral data previously obtained during imaging studies that evaluated the effects of intravenous methylphenidate (0.5 mg/kg) in comparison subjects and in cocaine abusers and compared it with the effects of placebo. In parallel, we also performed secondary analysis for studies of oral methylphenidate (20 mg), since we wanted to determine if methylphenidate, at the doses and route used therapeutically for ADHD, would also enhance sexual desire.
Method
For the intravenous methylphenidate experiment, participants were 39 healthy male comparison subjects (35 [SD=7] years old) and 39 male cocaine abusers (39 [SD=5] years old). Comparison subjects were screened for a lack of history of drug or alcohol abuse (excluding nicotine). Exclusion criteria were current or past psychiatric, neurological, cardiovascular, or endocrinological disease and dependence on any substance other than nicotine. Cocaine abusers included 19 current abusers and 20 cocaine abusers tested 3–6 weeks after cocaine discontinuation. Subjects fulfilled DSM-IV diagnostic criteria for cocaine dependence. Exclusion criteria were the same as for comparison subjects except for the exclusion for cocaine dependence.
For the oral methylphenidate experiment, subjects were 21 healthy male comparison subjects (34 [SD=8] years old) and 18 male current cocaine abusers (43 [SD=6] years old). Inclusion and exclusion criteria were the same as for the intravenous methylphenidate experiment. Toxicological drug screens were performed on the day of the study. Written informed consent was obtained for all subjects.
Subjects were tested on two different days; they received placebo on one day and methylphenidate on the other. The order was randomly assigned, and subjects were blind to whether placebo or methylphenidate was administered.
Subjects were asked to rate their sexual desire using an analogue scale from 0 (none) to 10 (very intense)
(8) . For the intravenous methylphenidate experiment, ratings were obtained 5 minutes prior to and 27 minutes after intravenous methylphenidate (0.5 mg/kg) or placebo (3 cc saline intravenous). For the oral methylphenidate experiment, ratings were obtained prior to and 130 minutes after oral methylphenidate (20 mg) or oral placebo (sugar tablet).
A factorial (comparison subjects versus cocaine abusers) repeated-measure (baseline versus placebo and baseline versus methylphenidate) design was used to assess the effects of intravenous placebo and of intravenous methylphenidate. Post hoc t tests were then used to assess the direction of the effects. A similar analysis was performed for the oral methylphenidate experiment.
Results
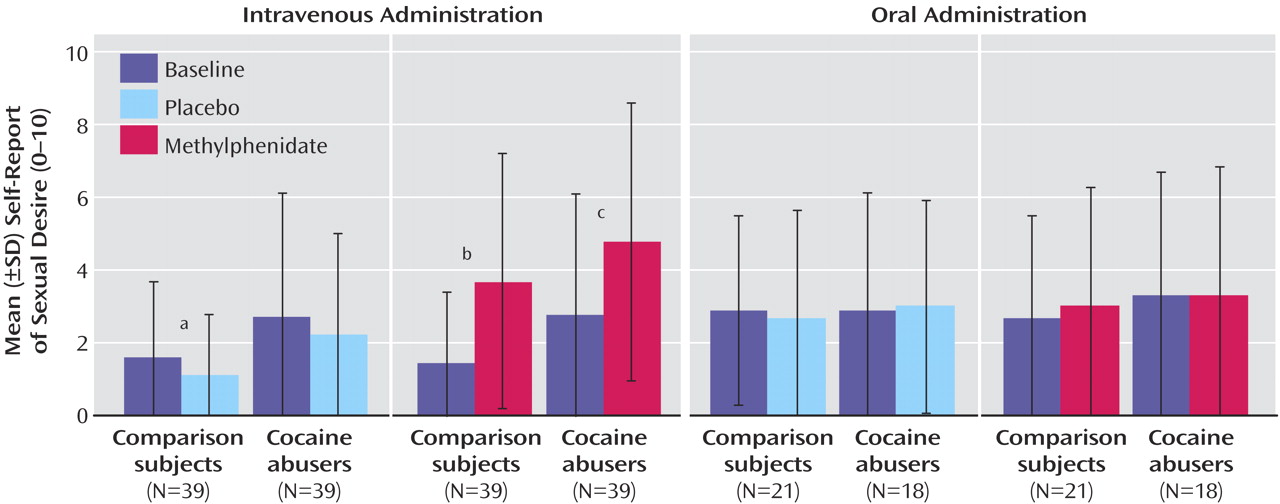
For the placebo condition, the analysis of variance (ANOVA) revealed a significant group (F=4.27, df=1, 76, p<0.05) and treatment effect (F=4.32, df=1, 76, p<0.05), but no interaction (p=0.91). Post hoc t test showed higher values for “sexual desire” in cocaine abusers than in comparison subjects (t=2.03, df=76, p<0.05) and showed that “sexual desire” was lower after the placebo than at baseline (t=2.52, df=38, p<0.02) in comparison subjects, but it did not differ in abusers (
Figure 1 ).
For the methylphenidate condition, the ANOVA revealed a significant group (F=4.76, df=1, 76, p<0.05) and treatment effect (F=25, df=1, 76, p<0.0001) (
Figure 1 ). The interaction was not significant, indicating that the response to methylphenidate did not differ between comparison subjects and abusers. Post hoc t tests showed higher baseline scores for sexual desire in cocaine abusers than in comparison subjects (t=2.28, df=76, p<0.03) and showed that methylphenidate increased sexual desire in comparison subjects (t=3.88, df=38, p<0.0004) and in abusers (t=3.19, df=38, p<0.003). A separate comparison between current and detoxified cocaine abusers revealed a significant treatment effect (F=10, df=1, 37, p=0.003), but neither the group nor the interaction effects were significant, indicating that the response to methylphenidate did not differ between detoxified and current cocaine abusers.
For the oral placebo as well as for the oral methylphenidate conditions, the ANOVA revealed no significant effect for group, treatment, or interaction. This indicates that oral methylphenidate (and oral placebo) did not increase sexual desire (
Figure 1 ).
Discussion
Intravenous methylphenidate increased sexual desire in comparison subjects and in cocaine abusers. These increases occurred even though the environment in which methylphenidate was given was devoid of sexual stimuli. Indeed, 27 minutes after the placebo, sexual desire was lower than prior to its injection, which most likely reflects the lack of stimulation in the testing environment (lying in the positron emission tomography scanner in a quiet, dimly lit room). The increase in sexual desire after intravenous methylphenidate is likely to reflect in part the large increases in dopamine induced by the drug when injected intravenously, since dopamine, through the mesolimbic-mesocortical system, regulates sexual arousal and motivation
(5) . Moreover, dopamine-enhancing medications can increase sexual libido
(11), and a common side effect for antipsychotic medications (dopamine receptor antagonists) is a reduction of sexual desire
(12) . In this respect, stimulant drugs such as amphetamine and methamphetamine, which induce much larger dopamine increases than methylphenidate or cocaine
(13), are likely to have an even greater effect on sexual desire than those reported in this study for methylphenidate. Although we emphasize dopamine in this study, it is likely that the noradrenergic effects of methylphenidate also contribute to its sexual arousal effects
(14) .
In contrast to the findings with intravenous methylphenidate, we did not find an effect of oral methylphenidate on sexual desire. This is likely to reflect the small dopamine increases induced by 20 mg of oral methylphenidate
(15) . However, because methylphenidate (by blocking dopamine transporters and amplifying dopamine signals) enhances the saliency of reinforcers
(15), we cannot rule out the possibility that oral methylphenidate could enhance the saliency of the sexual reinforcer in a sexually charged environment.
There was no difference in the increase in sexual desire induced by intravenous methylphenidate between comparison subjects and cocaine abusers, which indicates that this effect occurs both in stimulant abusers as well as in nondrug users. On the other hand, for the intravenous methylphenidate experiment, baseline levels of sexual desire for the cocaine abusers were higher than for comparison subjects. This is likely to reflect the overall arousal in the cocaine abusers who were expecting to receive a drug that they had been told was similar to cocaine; for this, difference was not evident when they were expecting oral methylphenidate.
Limitations for this study include the fact that the measure used to quantify sexual desire has not been validated. Additionally, what we document is an increase in sexual desire, which we assume would predict a greater probability to engage in sexual behaviors, but may not necessarily predict an increase in risky sexual behaviors. Since increases in risky sexual behaviors could reflect not only an enhancement of sexual desire but also a disruption in inhibition, it would have been desirable to have measured the effects of methylphenidate on decision making and on inhibitory control, particularly since studies in laboratory animals have shown that the large dopamine increases induced by amphetamine attenuate prefrontal suppression of limbic activity
(16) .
Recognizing that stimulant drugs increase sexual desire highlights one factor underlying why intoxication with stimulant drugs is a risk factor for HIV infection (and other sexually transmitted diseases) and why interventions to prevent and treat drug abuse are effective in preventing HIV transmission
(17) .