Understanding of pediatric bipolar disorder is hampered by questions about diagnostic criteria and limited pathophysiological research. Despite data suggesting that euphoria is common in pediatric bipolar disorder
(1 –
5) and that child and adult mania have similar clinical presentations
(3,
6), disagreement continues over 1) the importance of irritability as a symptom of mania and 2) whether manic symptoms in pediatric bipolar disorder present episodically. To facilitate research on these questions, we suggested a classification system differentiating children with strictly defined DSM-IV bipolar disorder (i.e., narrow phenotype) from those with nonepisodic irritability and hyperarousal (i.e., broad phenotype)
(7 –
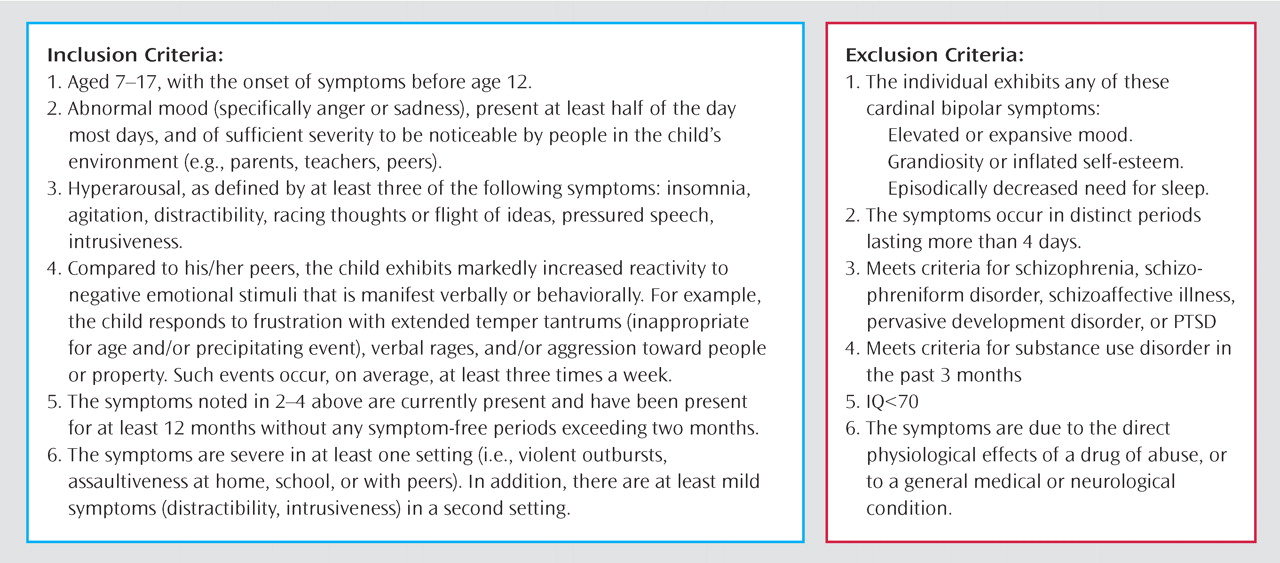
11) . Patients with narrow-phenotype bipolar disorder have a lifetime history of at least one episode of mania or hypomania that includes elevated mood or grandiosity. Patients with the broad phenotype, designated as severe mood dysregulation, exhibit nonepisodic irritability accompanied by hyperarousal and hyperreactivity to negative emotional stimuli, without elation or grandiosity (
Figure 1 ).
Most children who meet severe mood dysregulation criteria also meet DSM-IV criteria for attention deficit hyperactivity disorder (ADHD) and oppositional defiant disorder, since the severe mood dysregulation category captures many symptoms of these diagnoses. However, when studying pediatric bipolar disorder, there are two advantages to recruiting children with severe mood dysregulation as opposed to ADHD and oppositional defiant disorder. First, because the role of irritability in the diagnosis of pediatric bipolar disorder is controversial
(12), the severe mood dysregulation criteria for irritability are operationalized explicitly (inclusion criteria 2 and 4 in
Figure 1 ). Second, the overlap between ADHD symptoms and the symptoms listed under criterion “B” for a manic episode in DSM-IV creates diagnostic questions, and those overlapping symptoms are used to identify hyperarousal in severe mood dysregulation (inclusion criterion 3,
Figure 1 ). Thus, children with severe mood dysregulation are the specific focus of debate among bipolar disorder researchers.
Our classification system was designed to facilitate research on the pathophysiology of narrow-phenotype bipolar disorder and severe mood dysregulation. Because low frustration tolerance and irritability are prominent in both syndromes, it is crucial to develop research paradigms that elicit frustration so that its pathophysiology can be studied
(13) . The affective Posner task
(14,
15) assesses attention in different emotional contexts, including frustration. Using the affective Posner task, we found that in children with narrow-phenotype bipolar disorder, frustration is associated with attentional dysfunction, perhaps because their attention is drawn to their negative emotional state
(16) . Here we compare the pathophysiology of irritability in severe mood dysregulation and narrow-phenotype bipolar disorder, thus bringing physiological data to bear on the debate regarding diagnostic criteria for pediatric bipolar disorder. We use newly acquired data to compare the behavioral and psychophysiological correlates of frustration in children with severe mood dysregulation and children with narrow-phenotype bipolar disorder along with a group of healthy comparison children.
Method
Participants
We enrolled subjects with severe mood dysregulation (N=21), narrow-phenotype bipolar disorder (N=35), and no diagnosis (N=26) in an institutional review board-approved study at the National Institute of Mental Health (NIMH). Parents and children gave written informed consent/assent. Data collection in the narrow-phenotype and comparison subjects was completed before testing the severe mood dysregulation subjects
(16) .
The narrow-phenotype bipolar subjects met strict DSM-IV criteria: at least one hypomanic or manic episode (≥ 4 days of hypomania or ≥7 days for mania) with abnormally elevated mood or grandiosity and at least three symptoms listed under criterion “B” for a manic episode
(17) . Subjects with bipolar I and bipolar II disorder were included—provided they met narrow-phenotype bipolar disorder criteria—since our goal was to compare narrow-phenotype bipolar disorder and severe mood dysregulation. The severe mood dysregulation subjects were youth with nonepisodic irritability, overreactivity to negative emotional stimuli at least three times weekly, and hyperarousal (at least three of the following: insomnia, intrusiveness, pressured speech, flight of ideas/racing thoughts, distractibility, psychomotor agitation). Symptoms had to begin before age 12 and be present for at least 1 year without remission ≥ 2 months. Symptoms had to cause severe impairment (i.e., hospitalization, marked family discord) in at least one setting (home, school, peers) and mild impairment (i.e., school disciplinary problems, disrupted family activities) in another. Euphoric mood or distinct episodes lasting ≥4 days were exclusionary
(7) .
Diagnoses were made by using the Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version (K-SADS-PL), administered to parents and children separately. Comorbid diagnoses, also assessed using the K-SADS-PL, were present during euthymia and met DSM-IV criteria for impairment. Diagnosis of severe mood dysregulation was made using a K-SADS supplementary module (kappa ≥ 0.9). Exclusion criteria for patients were IQ<70, pervasive development disorder, unstable medical illness, or substance abuse within 2 months.
Comparison subjects had normal physical and neurological examination results. They and a parent completed the K-SADS to ensure that the subject had no psychiatric history.
Clinicians with interrater reliability administered to patients and their parents the Children’s Depression Rating Scale, the Young Mania Rating Scale, and the Children’s Global Assessment Scale. Patients also completed the Manifest Anxiety Scale for Children
(18) .
Posner Task
The Posner paradigm consisted of three tasks, with 100, 50, and 51 trials respectively. Tasks involved the same stimuli and instructions but differed in feedback and contingencies. On all tasks, a fixation cross appeared in the center of the screen, followed by three boxes arranged horizontally. Cues consisted of one box illuminating blue; cues appeared in the central box on 20% of trials, and in the right and left boxes on 40% each. Following cue presentation, a target square appeared inside either the left or right box. Subjects were instructed to press the button corresponding to the target location. Stimuli presentation was controlled by the STIM system (James Long Company, Caroga Lake, NY).
Task 1 was the nonemotional baseline; subjects were told their response accuracy (“Good job!” or “Incorrect!”) without contingencies. On task 2, subjects won or lost 10 cents on each trial, based on performance (“Great Job! Win 10 Cents” or “Wrong! Lose 10 Cents”). Task 3 had the same contingencies as task 2, but rigged feedback was added, making this a frustrating task. On 44% of trials, correct responses resulted in accurate feedback and monetary reward (“You are Quick! Win 10 Cents”). However, on 56% of correct responses, rigged feedback informed the subject that he or she was too slow and lost 10 cents (“Too Slow! Lose 10 Cents”). Incorrect responses always resulted in punishment feedback (“Wrong! Lose 10 Cents”). Task order was fixed to heighten arousal progressively and avoid carry-over arousal from the frustration task preceding other tasks. To examine the impact of reward and punishment on performance, trials were classified as post-reward or post-punishment based on the feedback preceding the trial.
Clinical Data
After each task, subjects rated their response to that task, reward, and punishment using the Self-Assessment Manikin
(19) : line-drawings with extremes of happy/unhappy (valence) or calm/aroused (arousal).
EEG signals were recorded with an electrode cap from temporal (T3, T4), frontal (Fz, F3, F4), central (C3, C4, Cz), and parietal (Pz, P3, P4) sites using the international 10/20 system, referenced to right earlobe. As in other developmental event-related potential studies
(15), we used average referencing (for sampling rate and filtering, see Rich et al.
[16] ).
Event-related potentials were collected to each target presentation. Peak amplitude within the designated time window was analyzed. Given prior results
(16) and a priori hypotheses, we focused on P3 (200–400 msec following target presentation) and N1 and P1 (50–150 msec).
We measured reaction time and response accuracy (i.e., percentage of responses matching target location).
Statistical Analysis
Repeated measures ANOVAs were conducted on P3, N1, and P1 amplitude, with group as the between-group variable and task and electrode site as within-subject factors. Each site (i.e., parietal, temporal, frontal, central) was analyzed separately. For reaction time and accuracy, separate 3×3 ANOVAs were conducted using group and task as factors. Greenhouse-Geisser correction was applied when appropriate, and post hoc comparisons employed the Tukey’s honestly significant difference test.
We conducted post hoc ANCOVAs to explore the impact of ADHD, oppositional defiant disorder, and major depressive disorder on the psychophysiological results. We used K-SADS-PL responses to create a continuous variable assessing symptom severity for each diagnosis; the measures on which our groups differed (Pz P3 amplitude and N1 temporal and central amplitude) were outcome variables. Given their proximity, we combined central and temporal N1 amplitude into one score to reduce the number of analyses and provide a more stable estimate of between-group differences. The presence or absence of bipolar disorder served as a categorical independent variable; ADHD or oppositional defiant disorder symptoms were covaried. Severe mood dysregulation designation could not be included due to multicollinearity among ADHD, oppositional defiant disorder, and severe mood dysregulation. Given the high correlation between ADHD and oppositional defiant disorder symptom scores (r=0.71, p<0.001), two ANCOVAs were conducted, one with ADHD and major depressive disorder symptoms as covariates, and one with oppositional defiant disorder and major depressive disorder as covariates.
Discussion
To investigate the pathophysiology of pediatric bipolar disorder phenotypes, we compared children with severe mood dysregulation (i.e., nonepisodic irritability, marked reactivity, and hyperarousal, but no episodic euphoric mania) to those with narrow-phenotype bipolar disorder (i.e., discrete episodes of mania with elevated mood)
(7) . Our results using the affective Posner paradigm (an attention task with emotional manipulations) suggest differences between these phenotypes in the behavioral manifestations and psychophysiological mechanisms of frustration.
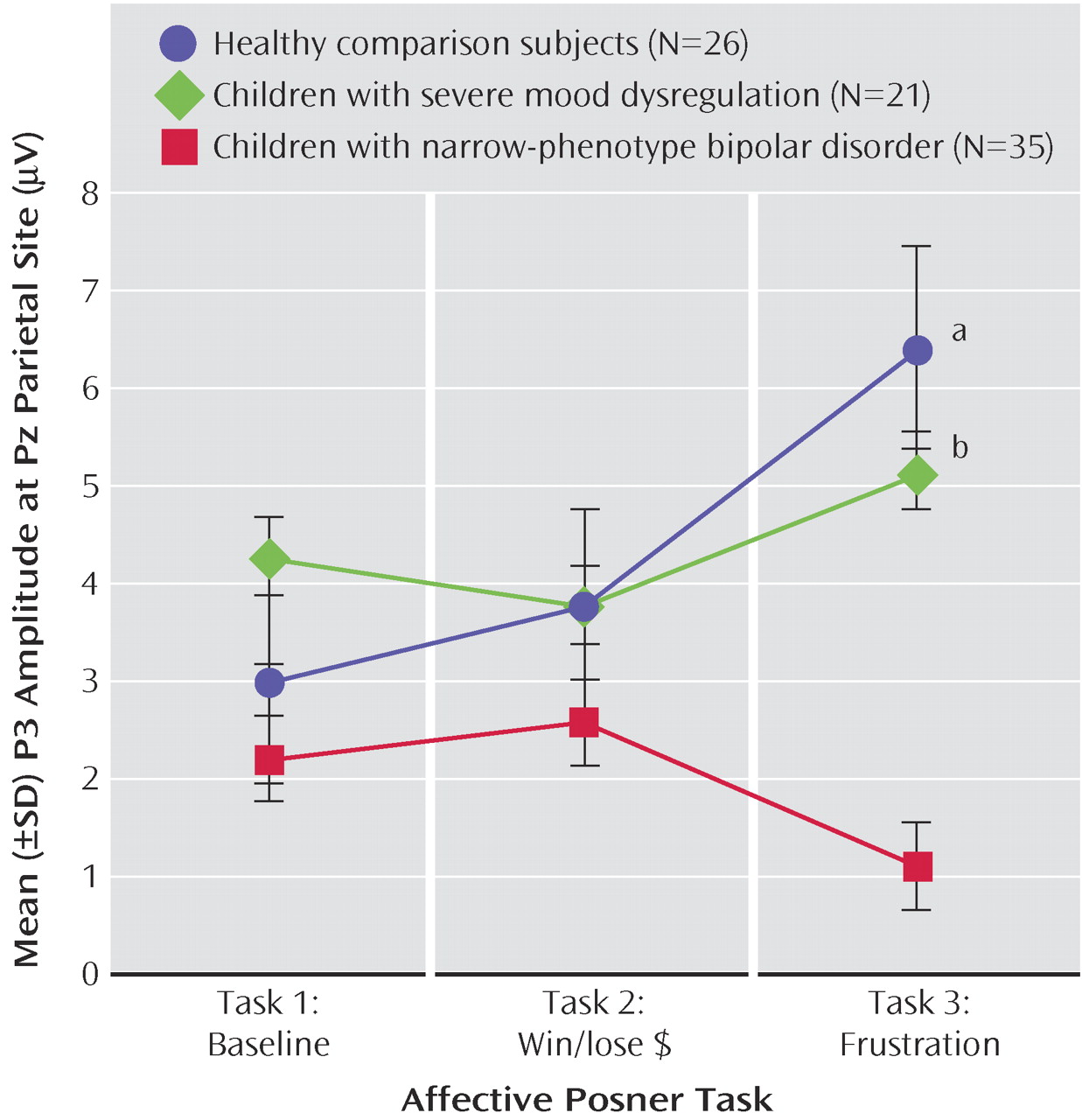
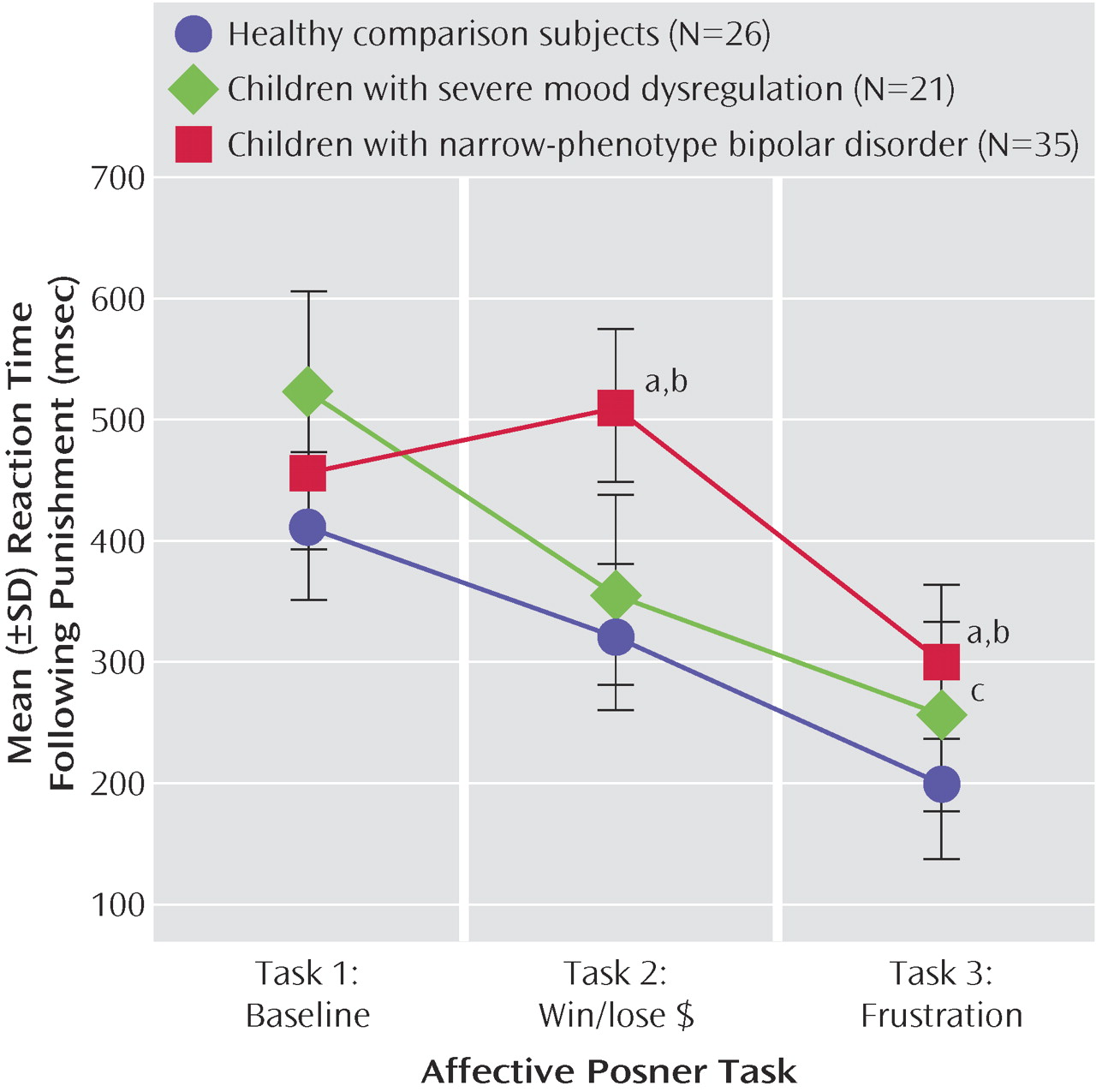
Participant reports indicated that the paradigm achieved the desired emotional effect: relative to comparison subjects, both patient groups reported significantly greater arousal on the frustration task. However, the psychophysiological data showed a double dissociation. Specifically, patients with narrow-phenotype bipolar disorder had decreased P3 amplitude when frustrated (suggesting executive attention deficits), but exhibited no N1 amplitude deficit. In contrast, subjects with severe mood dysregulation were unimpaired on P3 amplitude but had decreased N1 amplitude on all three tasks. Thus, the psychophysiological correlates of frustration differed between these two patient groups: comparable perturbations in subjective reports of affect (e.g., increased frustration, relative to comparison subjects) were associated with different physiology.
Attenuated N1/P1 amplitude, previously documented in ADHD
(20), suggests that children with severe mood dysregulation have deficits in initial attention regardless of emotional context, possibly accounting for their low accuracy. Whereas narrow-phenotype bipolar subjects displayed decreased P3 amplitude when frustrated, the children with severe mood dysregulation displayed normal P3 amplitude, suggesting that they can modulate their attention properly in the context of increased emotional demands
(21) . P3 deficits, seen here in narrow-phenotype bipolar disorder, have been associated with depression
(22) and can co-occur with slow reaction time in anhedonia patients
(23) .
Since approximately 90% of patients in both groups were euthymic when tested, the observed deficits may be trait based. Also, the significant correlations between outcome variables and impairment measures in both patient groups indicate that these behavioral and psychophysiological measures may indeed assess processes related to illness severity.
Our primary aim in this study was to move the debate regarding the boundaries of bipolar disorder in children beyond clinical descriptors by supplementing these with measures of brain function. Thus, we compared children with unequivocal bipolar disorder with children whose diagnostic status is controversial; these comparisons were not just on clinical features but also on brain-based measures. Since our narrow-phenotype bipolar disorder criteria are stricter than DSM-IV in that children with irritability only are excluded, an important question is the extent to which our findings are generalizable to other pediatric bipolar disorder samples in the literature. It is notable that the age at onset and level of impairment here are comparable to that in other reported samples
(1,
2,
4,
24) . However, direct comparisons to these samples are limited by our lack of data regarding longitudinal course, cycle frequency, or rapid-cycling rates. Further research is needed to ascertain the generalizability of our results to children with bipolar disorder assessed through other techniques.
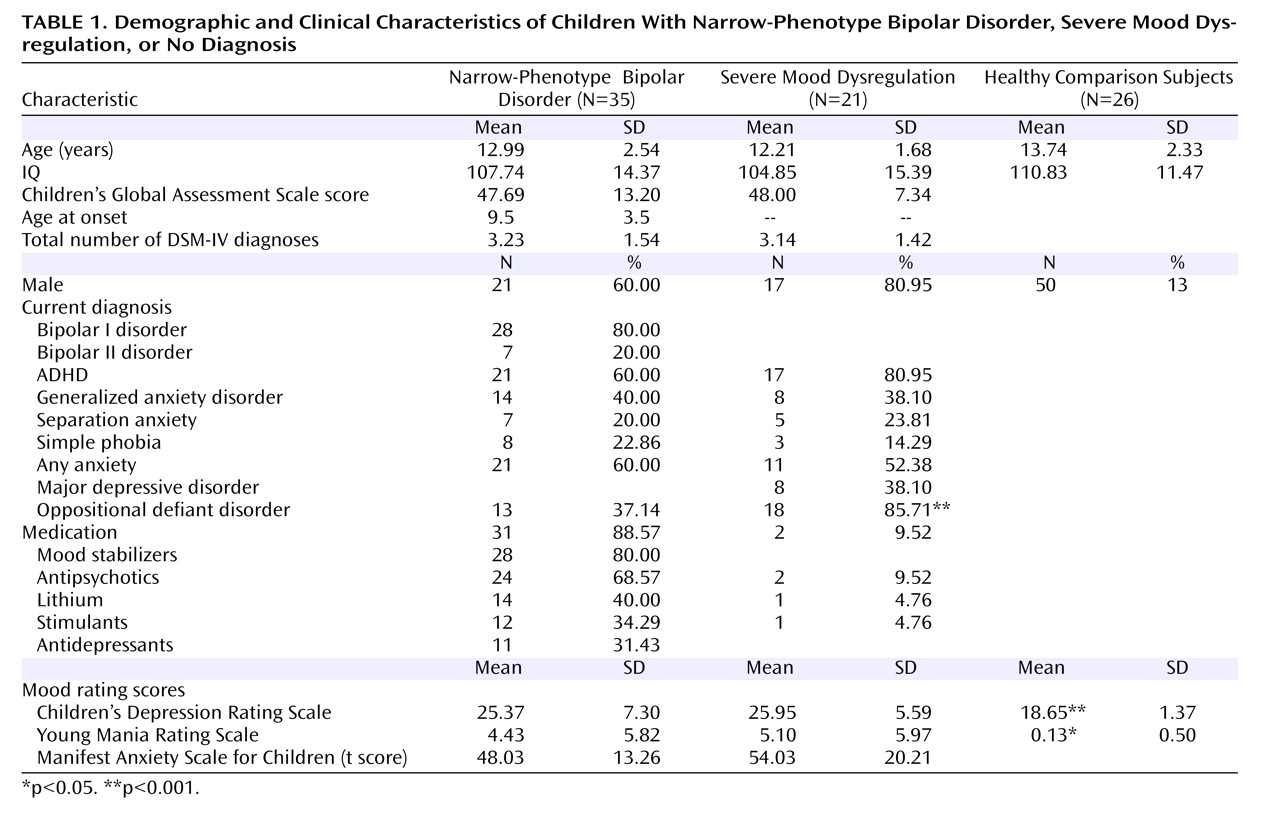
One important question is the utility of using the term severe mood dysregulation rather than describing our cohort as ADHD and oppositional defiant disorder youth with depression-like irritability. Most important, many children with oppositional defiant disorder or ADHD do not meet severe mood dysregulation criteria because, as noted earlier, the criteria for irritability and impairment secondary to irritability are particularly strict and clearly operationalized. Conversely, not all children with severe mood dysregulation met criteria for both ADHD and oppositional defiant disorder (
Table 1 ). Further, only 38% of the severe mood dysregulation subjects had a history of major depressive disorder. Nonetheless, recruiting children who meet severe mood dysregulation criteria presents challenges in relating findings to severe mood dysregulation as opposed to ADHD or oppositional defiant disorder. Severe mood dysregulation, oppositional defiant disorder, and ADHD are not easily dissociable, and to some extent represent alternative ways to classify a common group of children. Consistent with this possibility, we found that N1 amplitude was related to severity of oppositional defiant disorder symptoms as well as to severe mood dysregulation diagnosis. Regardless, our key observation is that N1 deficits, independent of emotional context, are associated with either oppositional defiant disorder or severe mood dysregulation but not bipolar disorder, whereas P3 deficits, present only during frustration, are associated with bipolar disorder but neither oppositional defiant disorder nor severe mood dysregulation.
The association between N1 amplitude and oppositional defiant disorder symptoms suggests that, whereas the diagnostic controversy in pediatric bipolar disorder has largely focused on the boundary between bipolar disorder and ADHD, the boundary between oppositional defiant disorder and bipolar disorder may be as important. Although usually conceptualized as a disruptive behavior disorder, oppositional defiant disorder has prominent mood components, specifically irritability. Longitudinal studies indicate an association between childhood oppositional defiant disorder and young adult major depressive disorder
(25) and between family history of major depressive disorder and childhood oppositional defiant disorder
(26) . Thus, whereas several studies compare children with ADHD to those with bipolar disorder
(27,
28), studies comparing children with oppositional defiant disorder to those with bipolar disorder or severe mood dysregulation would also be helpful. Because of comorbidity in these diagnoses, large patient groups will be required.
A major confound was that the narrow-phenotype bipolar disorder patients were predominantly medicated but the severe mood dysregulation subjects were predominantly unmedicated. Some studies have found that P3 amplitude normalizes (i.e., increases) in adults with schizophrenia treated with antipsychotic medications
(29) and in children with ADHD treated with stimulants
(30) . Other studies have failed to find such normalization with antipsychotics
(31), hypnotic medications
(32), or multipharmacology
(33) . No studies have suggested that medication decreases P3 amplitude. Furthermore, detailed studies of P3 amplitude and medication suggest that, whereas frontal P3 amplitude may be normalized by medications, parietal P3 amplitude, which was deficient in narrow-phenotype bipolar subjects, may be unaffected by medication
(34) . Finally, in this study, behavior and psychophysiology were comparable between narrow-phenotype bipolar patients and comparison subjects in nonemotional conditions; differences emerged only in emotional contexts. We are unaware of any reports of medications impacting P3 amplitude differentially based on the emotionality of the context. However, it is possible that our results reflect the interaction of medication effects and task demands. Future studies with unmedicated bipolar disorder patients, and direct comparisons of medicated and unmedicated cohorts, would be informative. Finally, because of the limited number of trials, we were unable to examine habituation or trends in behavior or psychophysiology within each task, which could potentially impact the interpretation of our results.
In conclusion, our results indicate that there may be different psychophysiological mechanisms and behavioral correlates associated with frustration between children with narrow-phenotype bipolar disorder and those with severe mood dysregulation. Whereas the deficits in the narrow-phenotype subjects indicated impaired allocation of attention in the context of frustration, those in the severe mood dysregulation group indicated impairments in the initial stages of attention across emotional and nonemotional tasks. Finally, whereas the deficits in the narrow-phenotype cohort are consistent with those seen in mood disorders, deficits in children with severe mood dysregulation may reflect concurrent oppositional defiant disorder. The current study is the first to provide evidence of behavioral and psychophysiological differences between possible phenotypes of pediatric bipolar disorder.