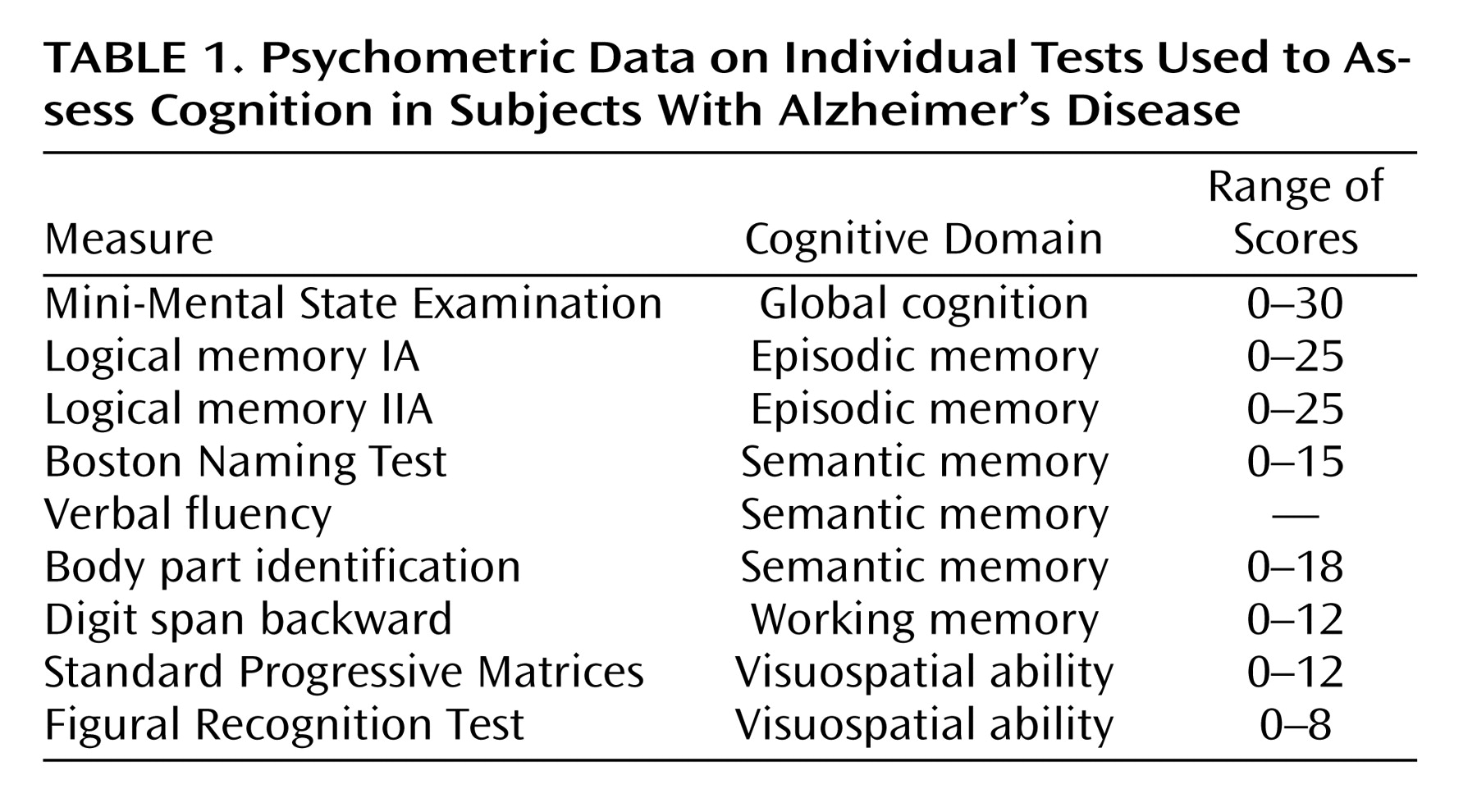
Day Care Use and Nursing Home Placement
At the time of the baseline evaluation, 196 participants (45.4%) were using day care services from 2 to 6 days a week for an overall mean of 1.7 days per week (SD=2.1) in the group as a whole. Use of day care was associated with older age (t=4.0, df=430, p<0.001), less education (t=4.8, df=377, p<0.001), and belonging to a racial or ethnic minority group (χ 2 =6.0, df=2, p=0.05) but not with sex (χ 2 =0.4, df=1, p=0.51).
During up to 4 years of follow-up (mean=2.2, SD=0.9), 155 persons (35.9%) were placed in a nursing home for a mean period of 0.54 years (SD=0.81, range=0.00–3.25). Nursing home placement was not associated with age (t=1.7, df=430, p=0.08), education (t=0.5, df=430, p=0.59), or sex (χ 2 =0.0, df=1, p=0.86). White non-Hispanic persons were slightly more likely to be institutionalized than African Americans and other racial or ethnic minorities (40.5% versus 28.2% and 6.3%; χ 2 =11.8, df=2, p=0.003).
Day Care Use, Nursing Home Placement, and Cognitive Decline
At baseline the composite measure of global cognition ranged from –1.662 to 2.361 (mean=0.063, SD=0.726), with higher scores indicating better function. We examined the relation of day care and nursing home use with individual patterns of change in cognitive function in a series of mixed-effects models adjusted for age, sex, race, and education.
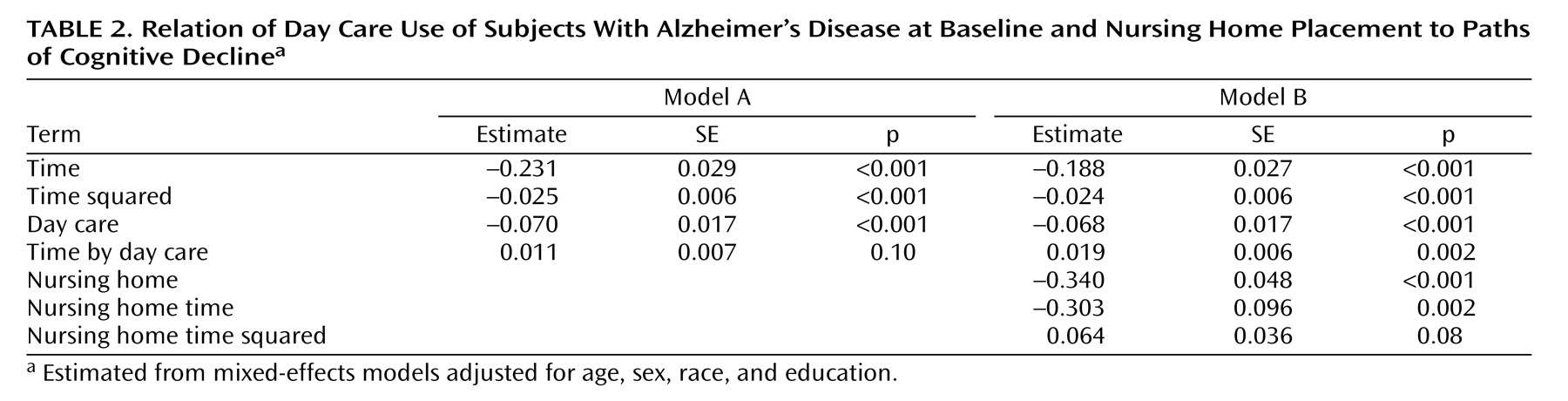
The initial analysis (
Table 2, model A) included terms for study time (in years since baseline) and study time squared to account for linear and nonlinear change in cognitive function and for day care use (in days per week at baseline) and its interaction with study time to test the association of day care use with initial level of cognition and rate of change. The effects for study time and study time squared indicate a gradually accelerating rate of global cognitive decline in the group as a whole. Higher level of day care use at baseline was associated with a lower level of cognitive function, as shown by the term for day care use but not with the rate of cognitive decline, as shown by the interaction term.
To examine the effects of nursing home placement, we repeated the analysis with a term to indicate whether or not the participant was in a nursing home at the time of testing and with terms for time since placement and time since placement squared (
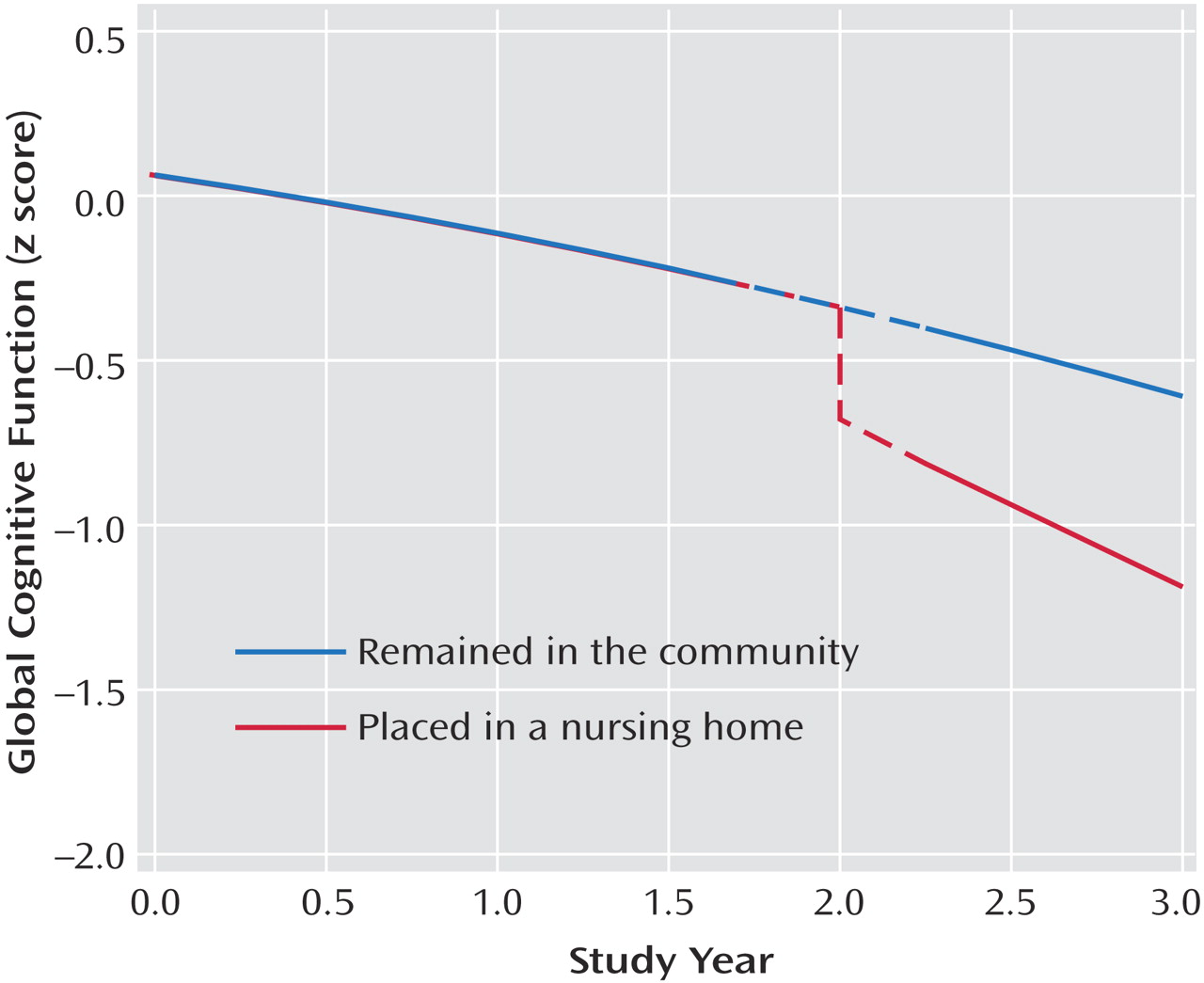
Table 2, model B). Placement in a nursing home was associated with a lower level of cognition and an accelerated rate of cognitive decline.
Figure 1 shows the predicted 3-year paths of change for two typical participants: with nursing home placement, both level of cognitive impairment and rate of cognitive decline increased.
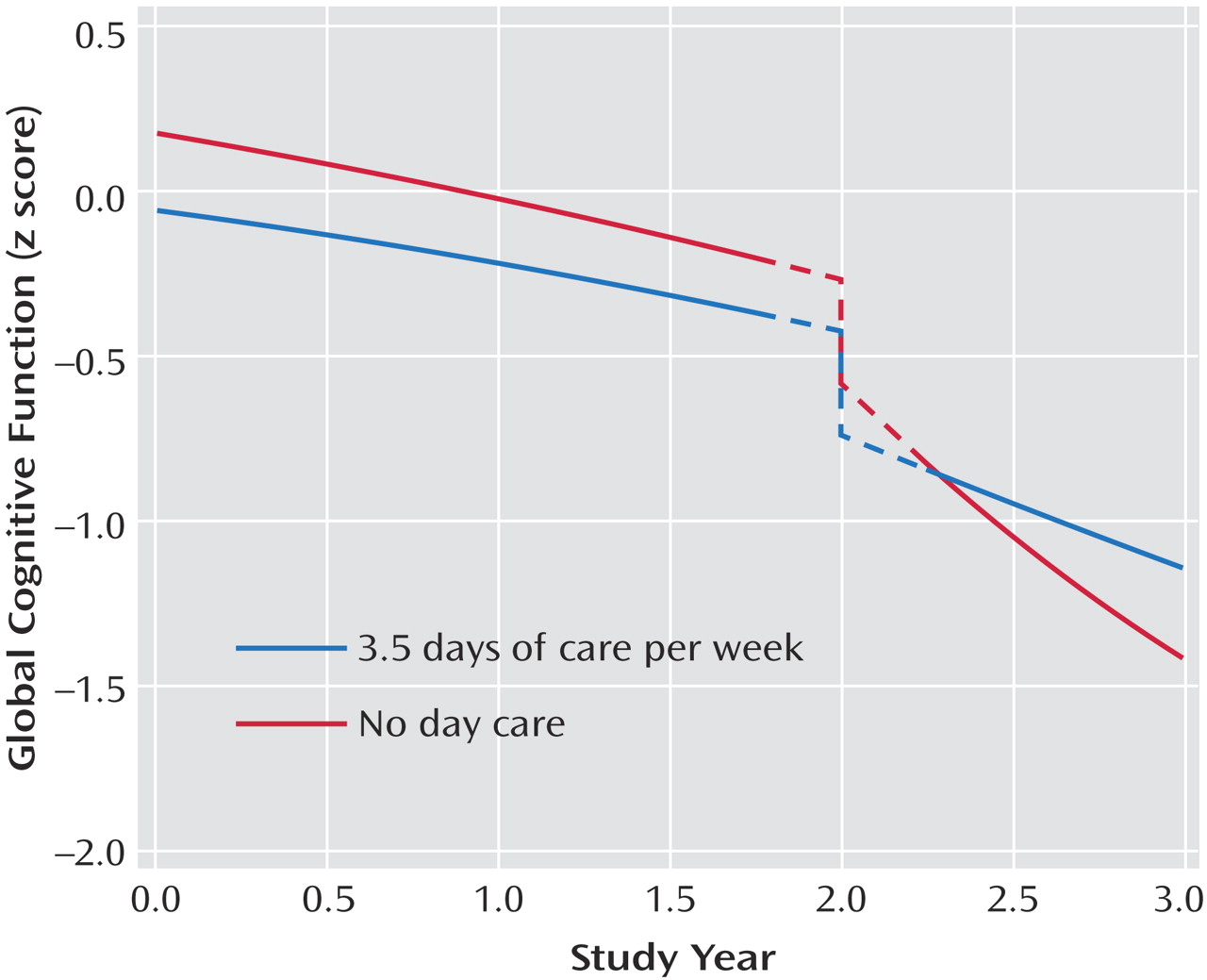
With nursing home placement accounted for in the model, higher level of day care use was associated with a slower rate of cognitive decline (
Table 2, model B). To determine whether day care use modified the association of nursing home placement with cognition, we repeated the analysis with terms for the interaction of day care use with nursing home placement. Day care use interacted with both nursing home time (estimate=0.158, SE=0.037, p<0.001) and nursing home time squared (estimate= –0.046, SE=0.016, p=0.005). To illustrate these results, we plotted the 3-year paths of decline predicted by the model for two typical participants who each entered a nursing home after 2 years in the study: one with no day care use at study onset and the other with high use (3.5 days per week); prior day care use markedly attenuated the association of nursing home placement with accelerated cognitive decline (
Figure 2 ).
To determine whether the associations among day care use, nursing home placement, and cognitive decline depended on noncognitive features of Alzheimer’s disease, we repeated the analysis, controlling for three variables at the time of nursing home placement: depressed mood (present in 5.8%) and two characteristics previously associated with nursing home placement, cognitive decline, and death in this cohort
(5,
16) : hallucinations (present in 39.1%) and physical disability (45.4% with substantial mobility limitation). In this analysis, nursing home entry continued to be related to more rapid cognitive decline, and the interactions of day care with placement time (estimate=0.156, SE=0.037, p<0.001) and placement time squared (estimate=–0.046, SE=0.016, p=0.006) were unchanged.
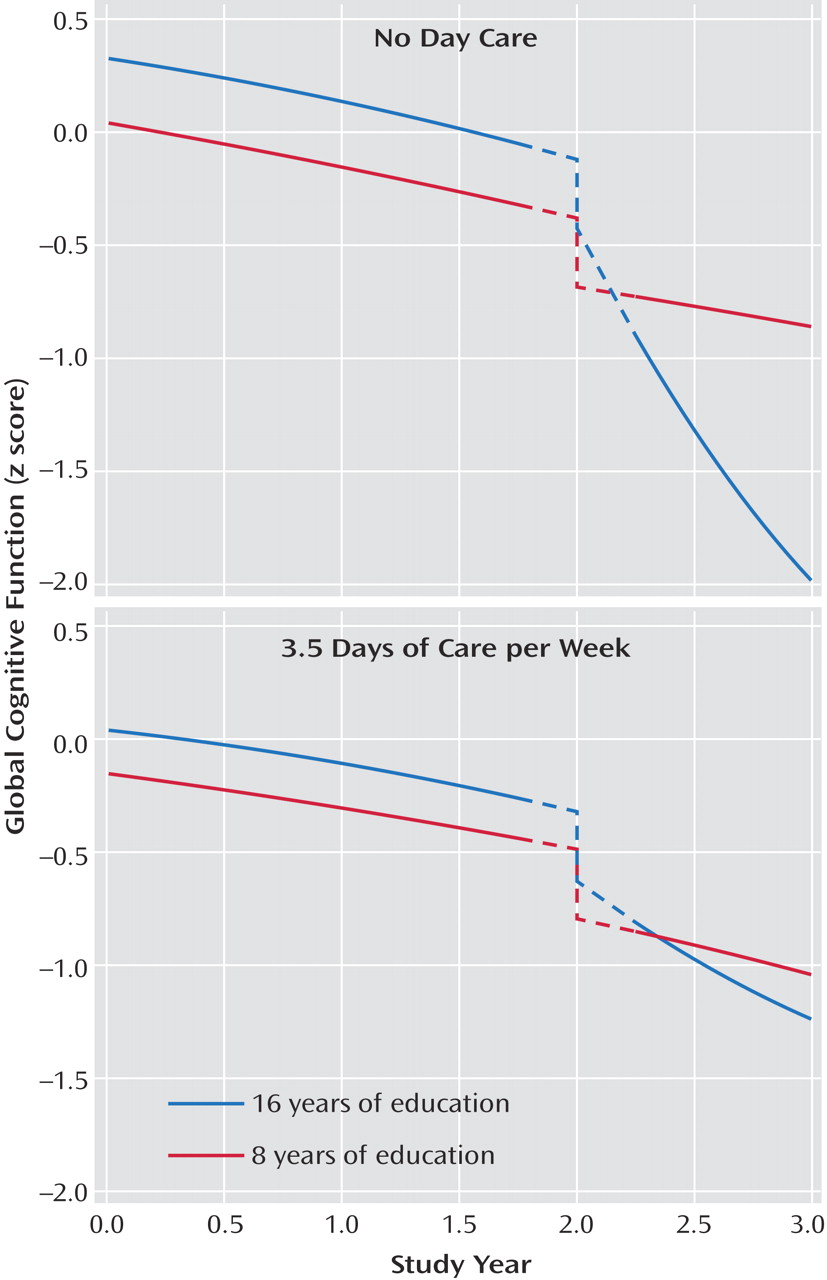
We next assessed whether the association of nursing home placement with cognitive decline varied along demographic lines. Education had a robust interaction with both nursing home time (estimate=–0.088, SE=0.021, p<0.001) and nursing home time squared (estimate=0.032, SE=0.008, p<0.001). The association of nursing home placement with accelerated cognitive decline was stronger at higher levels of education compared to lower levels. In another analysis, there were three-way interactions of education and day care with nursing home time (estimate=0.046, SE=0.011, p<0.001) and nursing home time squared (estimate=–0.010, SE=0.005, p=0.04). As shown in
Figure 3, among those with no day care at baseline, education strongly modified the association of nursing home placement with cognitive decline (upper panel), whereas among those with high day care use (3.5 days per week), education had little modifying effect (lower panel). In subsequent analyses, the association of nursing home placement did not strongly vary by gender or race, but there was an interaction of age with nursing home time (estimate=0.026, SE=0.007, p<0.001), indicating less of a nursing-home-related acceleration in decline for older compared to younger patients.