Attention deficit hyperactivity disorder (ADHD) is characterized by pervasive and impairing symptoms of inattention, hyperactivity, and impulsivity according to DSM-IV
(1) . The World Health Organization (WHO)
(2) uses a different name—hyperkinetic disorder (HD)—but lists similar operational criteria for the disorder. Regardless of the name used, ADHD/HD is one of the most thoroughly researched disorders in medicine
(3) . It has been associated with a broad range of negative outcomes for affected subjects
(4,
5) and with a serious financial burden to families and society
(6), which characterizes it as a major public health problem
(7) .
An understanding of the epidemiological aspects of ADHD/HD may provide insight into its distribution and etiology as well as information for planning the allocation of funds for mental health services
(8) . In past decades, investigators from all regions of the world have made substantial efforts to define the prevalence of the disorder. Several literature reviews have reported highly variable rates worldwide, ranging from as low as 1% to as high as nearly 20% among school-age children
(8,
9) .
Although the reasons for variability across studies remain poorly understood, it has been hypothesized that geographical and demographic factors are associated with it
(10) . Several investigators have suggested that prevalence rates in Europe were significantly lower than rates found in North America
(8,
11,
12) . This hypothesis fueled the concern that ADHD/HD may be a product of cultural factors and promoted an enduring debate in the medical literature
(8,
11,
12) . Other experts have argued that the variability of ADHD/HD prevalence estimates may be best explained by the use of different case definitions and that no variability of the actual prevalence across geographical sites should be found when case definitions are the same
(5,
8,
13) . A similar position has been adopted by the American Academy of Child and Adolescent Psychiatry, which states that conflicting results of ADHD/HD prevalence estimates can be explained by methodological differences across studies, such as method of ascertainment, diagnostic systems and associated criteria (e.g., situational versus pervasive, degree of impairment), assessment methods, informants, and the population studied
(4) . Unfortunately, no empirical evidence to date supports these assumptions, which led the American Medical Association
(3), the National Institute of Mental Health
(6), and the Centers for Disease Control and Prevention
(7) to call for further research on this issue.
Therefore, the main purpose of this study was to conduct an extensive review of the literature on the prevalence of ADHD/HD to 1) calculate a worldwide-pooled prevalence estimate and 2) determine factors implicated in the variability of estimates by examining the assumptions of different estimates based on geographic location of studies. Since some studies suggest that ADHD/HD prevalence is higher in North America, cross-national comparisons were conducted to investigate differences between North American studies and those conducted elsewhere. The main hypothesis was that geographic location would not significantly explain the variability of worldwide ADHD/HD prevalence estimates after adjustment for methodological differences across studies.
Method
Data Sources
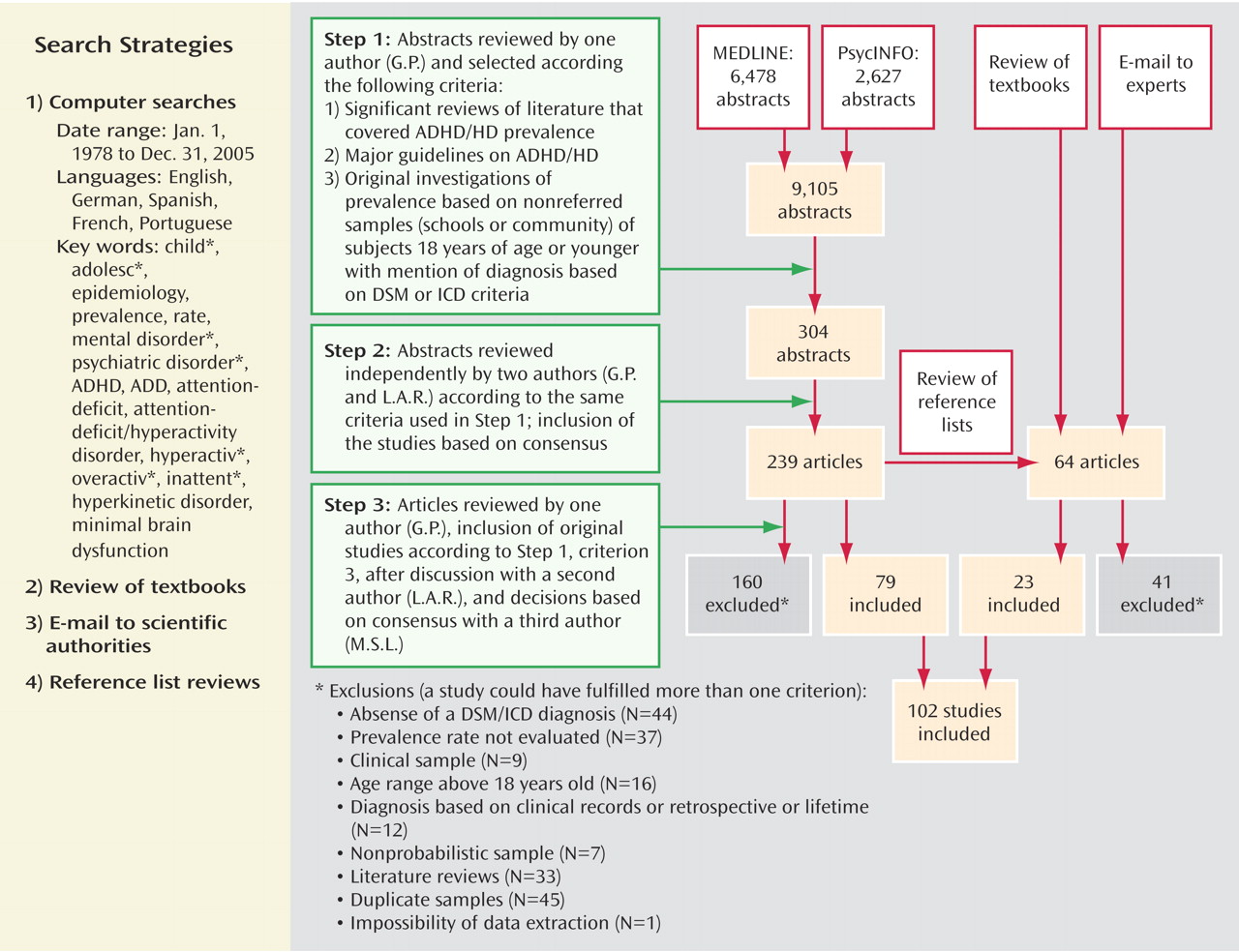
The following four search strategies were used for this systematic review of the literature: 1) computer search of databases, 2) review of specialized textbooks, 3) review of reference lists of all articles retrieved, and 4) contact with authors and experts on ADHD/HD epidemiology. This search strategy is in accordance with expert recommendations on the subject
(14) .
Computer search
We searched MEDLINE and PsycINFO from Jan. 1978 to Dec. 2005 for articles in English, German, French, Spanish, and Portuguese. Search words/terms were as follows: child*, adolesc*, epidemiology, prevalence, rate, mental disorder*, psychiatric disorder*, ADHD, ADD, attention-deficit, attention-deficit/hyperactivity disorder, hyperactiv*, overactiv*, inattent*, hyperkinetic disorder, and minimal brain dysfunction. An asterisk after a term means that all terms that begin with that root were included in the search.
Step 1 . Abstracts were reviewed by the first author (Dr. Polanczyk) and selected for further review if they met one of the following three criteria: 1) significant reviews of literature that covered ADHD/HD prevalence, 2) major guidelines on ADHD/HD, or 3) original investigation of prevalence based on nonreferred samples (schools or community) of subjects 18 years of age or younger diagnosed according to criteria established by any DSM (III, III-R, or IV)
(1) or ICD (9 or 10) versions
(2) . If a criterion was not met because not enough information was provided, the abstract was set aside for further evaluation.
Step 2. Abstracts were reviewed independently by two authors (Drs. Polanczyk and Rohde) and were selected based on their consensus according to the same criteria used in Step 1. If consensus was not reached, the abstract was set aside for further evaluation.
Step 3. Full-text articles of abstracts selected in Step 2 were retrieved and reviewed by one author (Dr. Polanczyk). Inclusion was based on consensus between two investigators (Drs. Polanczyk and Rohde). Disagreements were discussed with a third author (Dr. de Lima). Studies were included if they met the following criteria: 1) original surveys on ADHD/HD prevalence (point prevalence), 2) diagnoses based on any DSM (III, III-R, or IV) or ICD (9 or 10) versions, 3) probabilistic sample from the general population (e.g., households, birth registers) or from schools, and 4) subjects 18 years of age or younger. Twin studies and data from the first evaluation of longitudinal studies were included. The exclusion criteria were 1) studies that did not report confidence intervals (CI) or standard errors (SE) and that did not report data that allowed the calculation of these parameters and whose authors did not provide such data upon request and 2) studies that adopted a retrospective diagnostic approach based on subjects’ records. Authors were contacted via e-mail if data were missing.
Review of specialized textbooks
The ADHD/HD sections of five major textbooks on child and adolescent psychiatry and on general psychiatry were reviewed to identify references to original surveys that might meet Step 1 criteria.
Contact with experts
Forty-five scientific authorities in the field of ADHD/HD from North America, South America, Europe, Africa, Asia, Oceania, and the Middle East were contacted via e-mail and asked whether they were aware of unpublished or ongoing studies, and 28 experts returned responses.
Review of reference lists
The reference lists of all articles selected in Step 3 were reviewed, and the full texts of potentially interesting studies were examined.
Data Extraction
A protocol for data extraction was defined and evaluated by two authors (Drs. Polanczyk and Rohde) (available from authors upon request). Data were extracted from full-text articles by one author (Dr. Polanczyk) and reviewed by a second author (Dr. Rohde). Disagreements were discussed with a third author (Dr. de Lima).
To determine pooled estimates, each study contributed with only one estimate. Whenever a study generated multiple estimates according to different diagnostic or methodological definitions, one estimate was selected according to a previously defined protocol. This protocol ensured that data on each subject were extracted only once.
The computer program Epi Info version 6.04d
(15) was used to calculate CIs if they were not reported in the study.
Data Analyses
The first step of our previously defined strategy of data analysis was to determine an overall pooled-prevalence estimate of ADHD/HD based on all studies. A test of heterogeneity (Q test) was used to determine whether the differences in prevalence estimates across studies were greater than expected by chance. Significant heterogeneity was detected for the pooled estimate. At this point, sensitivity analysis was also performed, and findings showed that no study had skewed the overall result.
Since significant heterogeneity was found across studies, the second step was to conduct univariate analyses to test the individual association of each variable (methodological variables + geographic location of the studies) with the overall pooled-prevalence estimate of ADHD/HD using metaregression analyses
(16) . This analytical strategy evaluated which variables affected the results. Methodological variables were method of ascertainment of the sample (community or school), sample size, diagnostic criteria (DSM-III, -III-R, or -IV; ICD-9 or -10), source of information (best-estimate procedure, parents, “and rule,” “or rule,” teachers, or subjects), requirement of impairment for the diagnosis (yes or no), number of stages, and response rate (1-attrition rate).
We also tested the association between geographic location and variability of the overall pooled-prevalence estimate of ADHD/HD. Studies were divided into seven groups according to their geographic location: Africa, Asia, Europe, the Middle East, North America, Oceania, and South America. Three studies were fully conducted in Central America (Costa Rica), and one was a multisite study conducted in the United States and Costa Rica. These studies were grouped with those from North America.
In the third step, a random-effects regression model was used to evaluate sources of variability in the overall pooled-prevalence estimate of ADHD/HD. All covariates associated with ADHD/HD prevalence rates for a flexible p≤0.2
(17) in univariate analyses were included in the final multivariate metaregression model. For these analyses, a significance level of 5% was established.
Age and gender were not included in the final multivariate metaregression model because less than 50% of the studies reported findings stratified by these variables, but individual estimates were computed according to these strata (age was stratified into the following ranges: 6–11 and 12–18). At this stage, we also determined pooled estimates for each geographic region. All analyses were performed using Stata 9.0 (Stata Corp, College Station, Tex.).
Results
We screened 9,105 abstracts published in the last 27 years. A total of 303 full-text articles were reviewed, and 102 studies comprising 171,756 subjects were included in this systematic review (
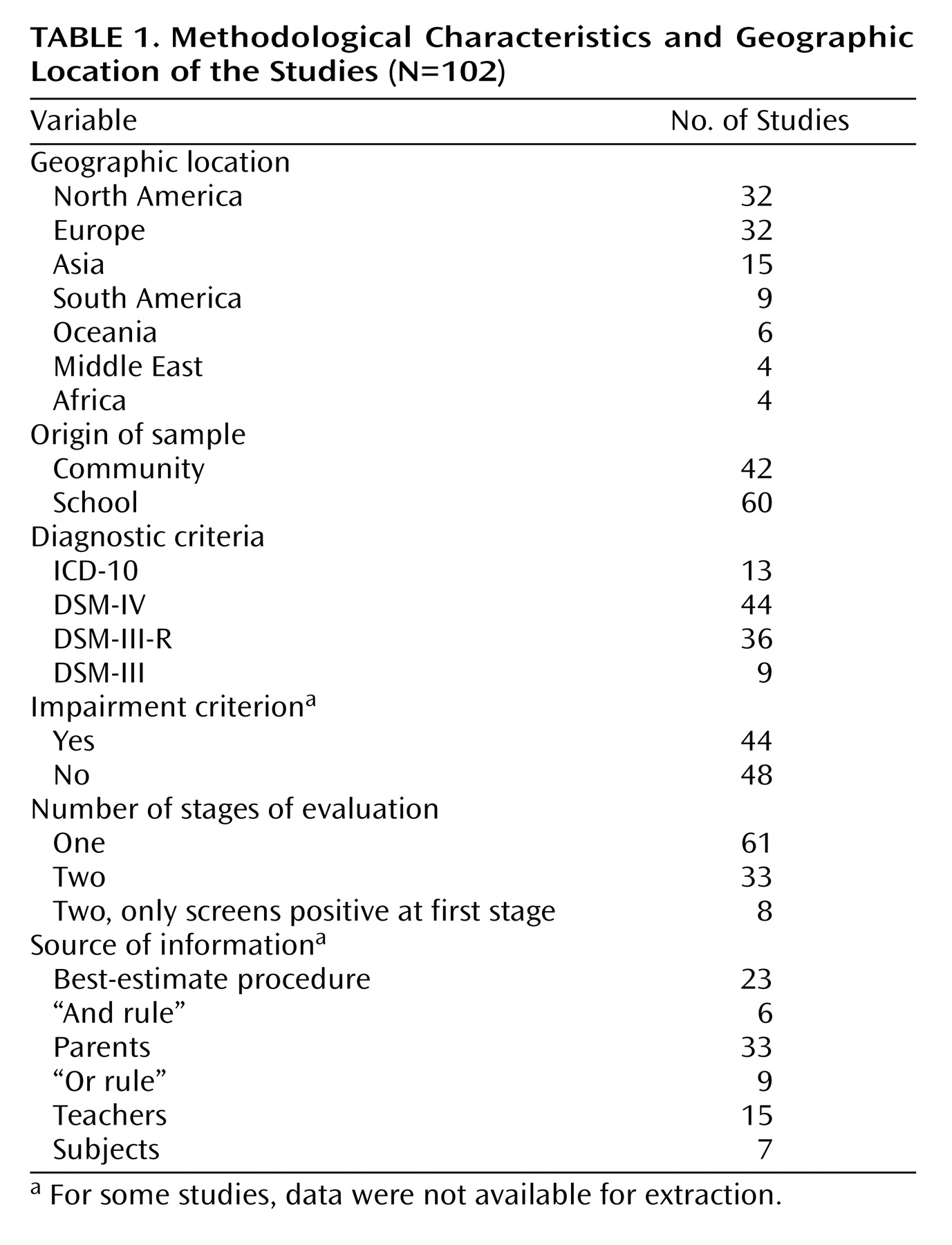
Figure 1 ). The list of reviewed references is available at http://www.ufrgs.br/psiq/prodah-e.html. Studies from all continents were retrieved. Of the 102 studies included, 32 were conducted in North America and 32 in Europe. The most frequent diagnostic system was DSM-IV. Characteristics of studies included in the analyses are described in
Table 1.Overall, the pooled prevalence of ADHD/HD was 5.29% (95% CI=5.01–5.56). This analysis revealed significant heterogeneity across studies (p<0.001). In univariate metaregression analyses (
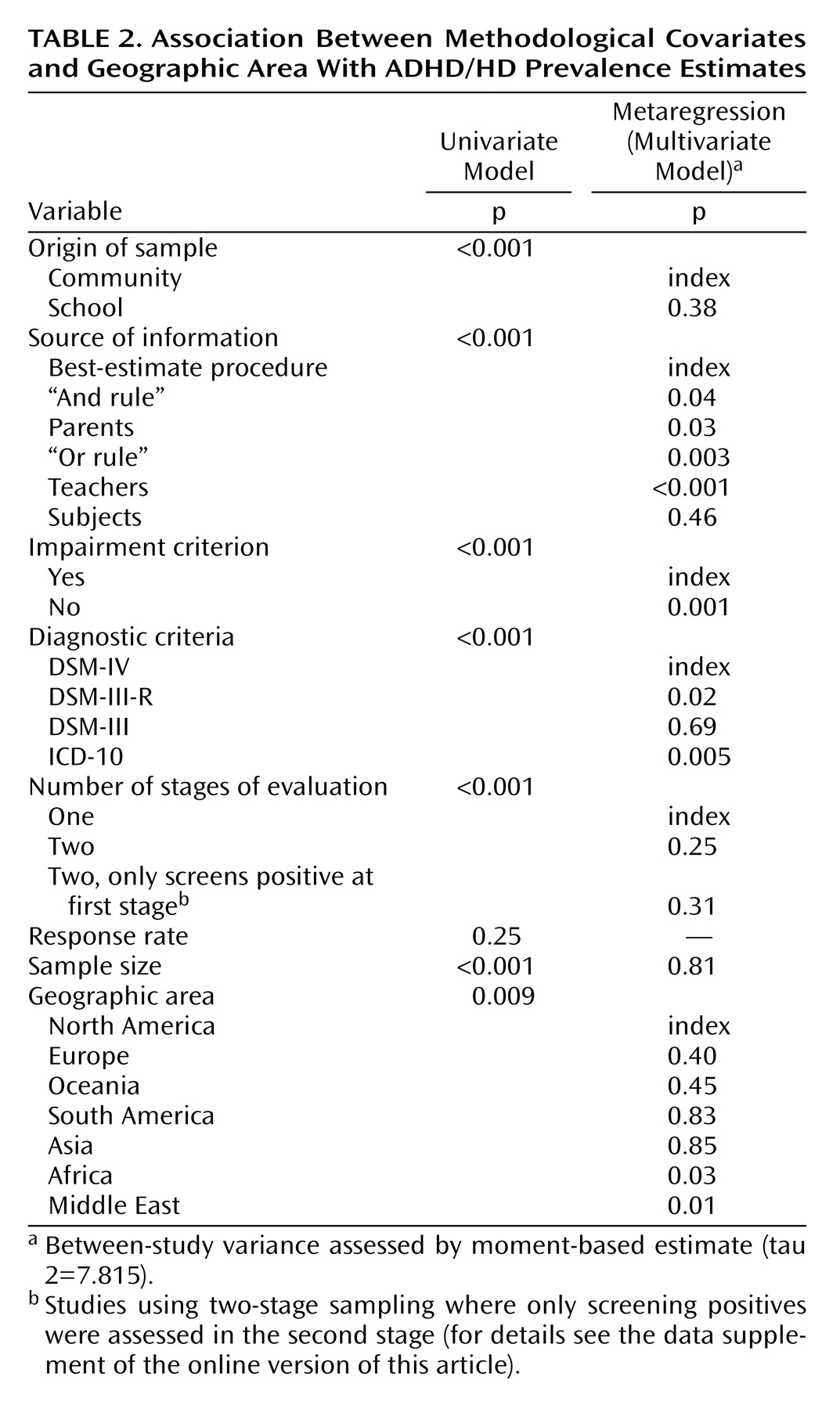
Table 2 ), all methodological variables evaluated were significantly associated with ADHD/HD prevalence rates, except response rate (p=0.25). The geographic location of studies was also significantly associated with the variability of ADHD/HD prevalence rates and was included in the final metaregression model.
In the final multivariate metaregression model (
Table 2 ), the methodological variables that remained significantly associated with the prevalence rates were the requirement of impairment for the diagnosis, diagnostic criteria, and source of information. As expected, studies without a definition of impairment had significantly higher ADHD/HD prevalence rates than those with a definition of impairment (p<0.001). Studies based on DSM-III-R or ICD-10 criteria, respectively, had significantly lower ADHD/HD prevalence rates than those using DSM-IV criteria (p=0.02 and p=0.005, respectively). Studies that relied on information provided by parents, teachers, and “or rule,” respectively, were associated with significantly higher ADHD/HD prevalence rates than those relying on a best-estimate procedure (p=0.02, p<0.001, and p=0.003, respectively), whereas those relying on information provided using the “and rule” criterion were associated with significantly lower ADHD/HD prevalence estimates (p=0.04) (
Table 2 ).
Geographic location was associated with significant variability between estimates from North America and both Africa (p=0.03) and the Middle East (p=0.01). Estimates from these areas were significantly lower than estimates from North America. No significant differences were found in prevalence rates between North America and Europe (p=0.40), South America (p=0.83), Asia (p=0.85), or Oceania (p=0.45) (
Table 2 ).
The multivariate metaregression model using Europe for the comparison yielded similar findings. Impairment, diagnostic criteria, and source of information remained significantly associated with prevalence rates. Significant differences were found only between Europe and both Africa (p=0.05) and the Middle East (p=0.03).
To increase power by decreasing degrees of freedom, an additional model was run using only methodological variables initially. Methodological variables associated with the prevalence rate for a p≤0.20 in univariate analyses were initially included and progressively deleted from the model using a backward procedure. Then, the geographic location of the studies was entered. In this multivariate model, geographic location was not significantly associated with prevalence rates after adjustment for methodological variables (data available from authors upon request).
Finally, since most studies were conducted in Europe and North America (N=64), the same data analysis strategy was applied using only these two regions. In the final multivariate metaregression model, the same methodological variables remained significantly associated with prevalence rates: impairment, diagnostic criteria, and source of information. Again, geographical location (Europe versus North America) was not significantly associated with ADHD/HD prevalence rates (p=0.61).
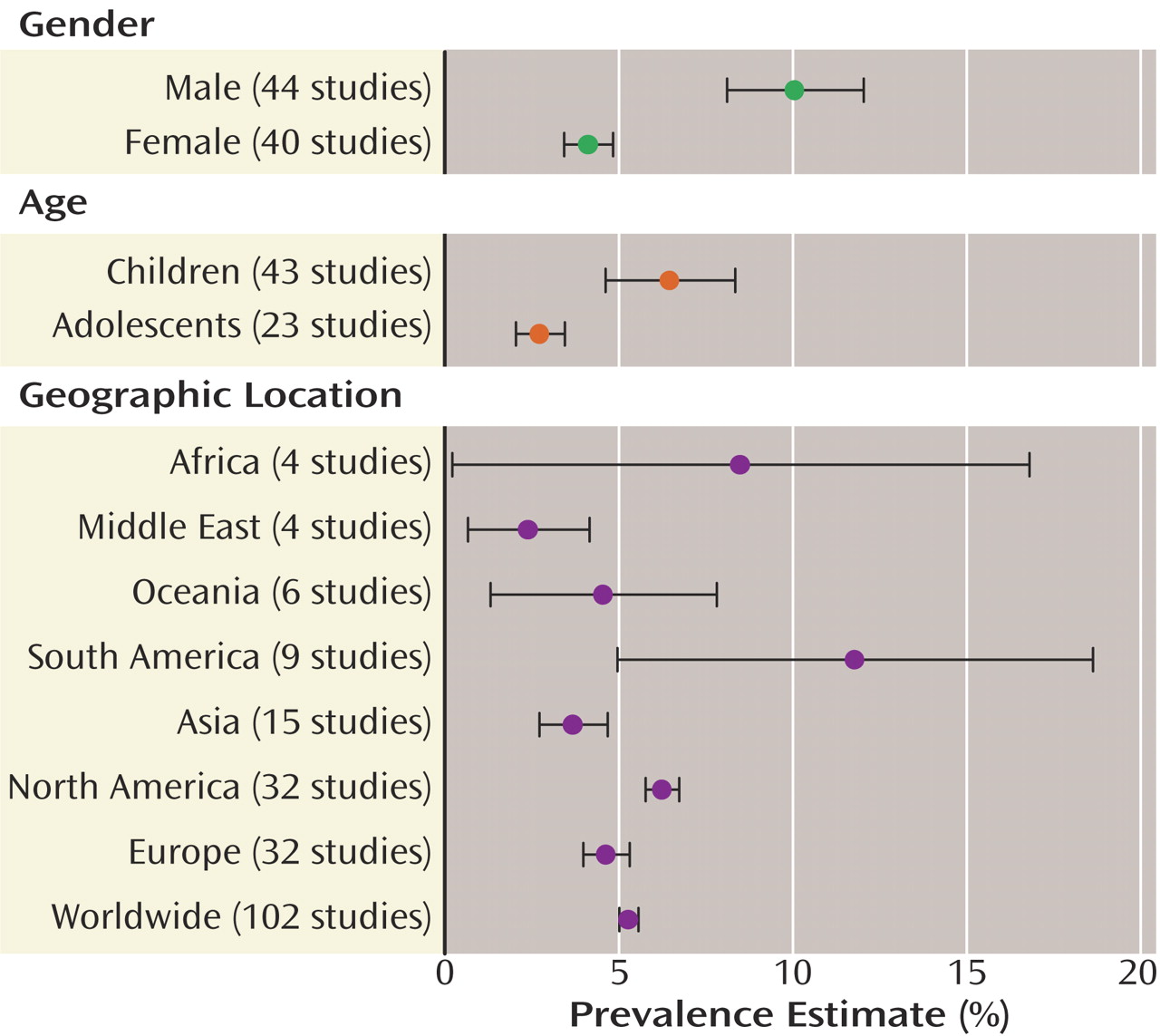
ADHD/HD prevalence rates were stratified by age in 43 studies and by gender in 44 studies. In these studies, both age and gender were significantly associated with prevalence rates (p<0.001). The pooled prevalence of ADHD/HD stratified by gender and age can be found in
Figure 2. The pooled prevalence in the seven geographic areas assessed is also shown in
Figure 2 . These analyses revealed significant heterogeneity across studies (p<0.001).
Discussion
We have conducted a comprehensive systematic review of studies addressing prevalence rates of ADHD/HD worldwide and a metaregression analysis to understand the reasons of estimate variability. Our findings show that 1) the ADHD/HD worldwide-pooled prevalence is 5.29% (95% CI=5.01–5.56); 2) the large variability of ADHD/HD prevalence rates worldwide resulted mainly from methodological differences across studies; and 3) adjusting for methodological differences, prevalence rate variability was only detected between studies conducted in North America and those conducted in Africa and the Middle East. Moreover, no significant differences in ADHD/HD prevalence rates between North America and Europe were detected in the overall metaregression analysis and in the analysis restricted to studies conducted on these two continents. To our knowledge, this is the broadest systematic review of this subject to date.
Our search strategy identified original studies of ADHD/HD prevalence conducted on all continents. Despite the higher number of studies conducted in North America and Europe, our literature search showed that ADHD/HD is a well-studied disorder and that its prevalence rate has been estimated in several different cultures.
Although the ADHD/HD worldwide-pooled prevalence is consistent with results reported in most previous reviews
(9,
18,
19), our results should be interpreted with caution because of the large variability found in all analyses. Our metaregression analysis reports, for the first time, on the critical role that methodological variables (i.e., impairment criterion, diagnostic criteria, and source of information) play in the large variability of ADHD/HD prevalence estimates in different geographic locations. This finding empirically supports assumptions previously discussed in the literature
(8,
9) . For instance, applying the same methodological procedures and diagnostic criterion, very similar rates of ADHD/HD were found in Russia
(20) and Britain
(21) (1.3% and 1.4%, respectively). However, when the diagnosis of ADHD/HD was made in the same geographic location but according to a different methodological criterion (i.e., with or without the requirement of functional impairment) estimates ranged from 3.7% to 8.9%
(22) .
ADHD/HD terminology has undergone significant changes over the past decades. The current ICD-10 and DSM-IV criteria provide very similar lists of symptoms but recommend different ways of establishing a diagnosis. The ICD-10 requires a minimum number of symptoms in all three dimensions (inattention, overactivity, and impulsivity). The DSM-IV defines only two dimensions (with hyperactivity and impulsivity symptoms included in the same dimension), and a diagnosis can be made if there is a minimum number of symptoms in only one dimension. The ICD-10 requires that all criteria be met in at least two different situational contexts, whereas DSM-IV requires the presence of some impairment in more than one setting. The ICD-10 includes mood, anxiety, and developmental disorders as exclusion diagnoses. In DSM-IV, these diagnoses may be classified as comorbid conditions. Therefore, ADHD prevalence rates based on DSM-IV are expected to be higher than those based on ICD-10, which was demonstrated by individual studies
(23) and corroborated by our analyses.
Our finding of lower ADHD/HD prevalence rates in Africa and the Middle East than in North America should be carefully interpreted. These geographic areas contributed with only a few studies to the overall analysis, and therefore we cannot rule out the possibility of lower accuracy of the adjustment for methodological aspects of these studies. Nevertheless, data concerning the lack of significant differences in ADHD/HD prevalence rates between North America and Europe in all sets of metaregression analyses are extremely relevant. This finding argues against the view that ADHD/HD is a culturally-based construct peculiar to the North American culture
(12) . It is important to note, however, that we do not suggest that culture has no influence on the prevalence of this disorder in a given population. Environmental and cultural aspects should play a role in the etiology of ADHD/HD, since the estimates of heritability in the disorder are approximately 80%
(24,
25) .
Our findings should be understood in the context of some limitations. First, characteristics of the subjects (age and gender) were not included in the final metaregression model because less than 50% of the studies reported results stratified by age or gender or provided data that allowed us to calculate these distributions. Second, other characteristics of the countries, besides geographic location, could not be assessed. However, the geographic location of a country is conceptually relevant for the purpose of this study and is often cited as a factor that may explain the variability of ADHD/HD prevalence rates. Finally, we did not provide estimates of ADHD/HD prevalence among adults, an emerging new area of research
(26) that should be addressed in future studies.
Despite these limitations, we found a large variability in ADHD/HD prevalence rates worldwide. Results suggest that geographic location may play a limited role in the explanation of this variability. The many methodological differences in the 102 studies assessed may be the most important source of variability in the pooled estimate of ADHD/HD prevalence. These results indicate that international efforts from institutions such as WHO should be directed to the standardization of epidemiological studies so that comparable epidemiological data from all regions of the world are made available for the study of relevant mental disorders such as ADHD/HD.