Children suffer from generalized anxiety disorder, social phobia, obsessive-compulsive disorder (OCD), and panic disorder, which are recognizable by syndromal characteristics and phenomenology equivalent to those found in adult disorders and meet DSM-IV criteria
(1,
2). Anxiety disorders persist throughout childhood
(3,
4), may worsen over time
(5), and may become essentially stable during early adolescence to young adulthood
(6). Separation anxiety disorder, the most common anxiety disorder of childhood
(7), often proceeds the onset of adult anxiety disorders, particularly panic disorder
(8,
9). It is thought that a childhood history of separation anxiety disorder identifies a particularly heritable early-onset form of panic disorder
(10). Evidence for childhood separation anxiety disorder as an antecedent to adult panic disorder includes 1) retrospective reports of childhood anxiety from adults with panic disorder
(11); 2) longitudinal studies of childhood separation anxiety disorder documenting abnormalities of ventilatory physiology similar to those of adults with panic disorder and predicting the onset of panic attacks
(12); and 3) the responsiveness of separation anxiety disorder to pharmacotherapies recommended for panic disorder
(8). Alternative views of this proposed linkage cite the high prevalence rate of separation anxiety disorder coupled with selective recall among adults
(13), such that separation anxiety disorder may be a nonspecific precursor to adult anxiety disorders
(14). Neurobiologic diatheses of childhood anxiety disorders have recently been elucidated by using adult experimental paradigms following the most robust of findings in adults with panic disorder as a guide
(12,
15). The most productive paradigms for this strategy, although controversial, have been either physiologic (e.g., CO
2)
(12) or pharmacologic (e.g., clonidine) challenges in children with anxiety disorders
(15) uncovering biologic abnormalities implicated in adult panic disorder. The noradrenergic system, central to the monitoring and interpretation of suffocation cues
(16) in both adult panic disorder and childhood anxiety disorders, exhibits heightened sensitivity to noradrenergic agents
(17,
18). This enhanced sensitivity suggests dysregulation of noradrenergic pathways and may play a role in the pathophysiology of childhood anxiety disorders and may be a biological precursor to panic disorder.
Preclinical
(19) and clinical studies
(20–
22) have provided evidence of dysregulation in the noradrenergic pathway in the development of anxiety disorders. Stimulation of central a
2 adrenergic receptors with clonidine normally results in elevated growth hormone (GH) output, but this response appears to be blunted in adults with panic disorder
(20), generalized anxiety disorder
(23), and perhaps OCD
(24). The response of patients with anxiety disorders to a clonidine challenge is cited as evidence of the subsensitivity of central a
2 adrenergic postsynaptic receptors. This subsensitivity is potentially the result of long-term locus ceruleus activity, which, over time, leads to a down-regulation of the hypothalamic a
2 adrenergic postsynaptic receptors that mediate GH release. Our laboratory was the first to demonstrate that a clonidine challenge in children with anxiety disorders is not characterized by GH blunting
(15). This finding implies that the early onset of anxiety disorders may not involve a
2 adrenoceptor down-regulation and argues for further exploration.
Yohimbine, an a
2 adrenergic antagonist, increases the release of norepinephrine in the hippocampus and other brain areas through increased firing of the locus ceruleus, resulting in behavioral and biologic correlates of anxiety in patients with panic disorder. Interpretation of data from yohimbine challenges is complicated by mixed drug effects due to blockade of both pre- and postsynaptic a
2 adrenergic receptors in the hypothalamus and presynaptic D
2 dopaminergic autoreceptors in the pituitary
(25,
26). The quick onset and limited duration of yohimbine effects on plasma concentrations of the norepinephrine metabolite 3-methoxy-4-hydroxyphenylglycol (MHPG), diastolic blood pressure, and patient ratings of anxiety suggest that the sum total of effect is largely reflective of presynaptic norepinephrine activity. It is hypothesized that diminished presynaptic sensitivity of the a
2 adrenergic autoreceptor is related to presynaptic norepinephrine hyperactivity (evidenced by increased sensitivity to yohimbine)
(27). Yohimbine in children with anxiety disorders should be consistent with presynaptic norepinephrine overactivity, but to our knowledge, such studies are absent from the literature.
Response to a norepinephrine challenge may vary not only by anxiety diagnosis but also by developmental stage. Pine et al.
(18) performed clonidine challenges in a heterogenous group of children with anxiety disorders and found enhanced MHPG response, the opposite of exaggerated decreases in MHPG reported in adult panic disorder. Sallee et al.
(15), using the same challenge in a similar population, documented hypersecretion of GH in relation to normal age-matched comparison subjects where blunting would be expected in adults. Mindful of developmental influences, we set out to evaluate children with anxiety disorders who had previously been characterized by an intravenous clonidine challenge
(15) by means of oral yohimbine and in comparison to age-matched comparison children. Although the importance of adrenergic dysregulation is assumed to vary across adult anxiety disorders (i.e., panic disorder versus OCD), for this exploratory study, no a priori assumptions were made, and broad inclusion criteria covering many common childhood anxiety disorders were used. Separate analyses across childhood anxiety disorders were then performed to determine the importance of norepinephrine sensitivity in the pathogenesis of specific disorders of interest (i.e., separation anxiety disorder). The hypothesis to be tested was whether children with anxiety disorders would demonstrate yohimbine responses similar to those of adults with anxiety disorders (i.e., panic disorder), either by enhanced self-ratings of anxiety and/or attenuated neurohormonal output (e.g., GH blunting).
Method
Subjects
Children seen at a tertiary psychiatric outpatient service of the Medical University of South Carolina from 1994 to 1996 with a primary DSM-IV diagnosis of an anxiety disorder (N=17) were matched by sex and age to normal comparison children (N=15) who were chosen from a general clinical research center pool from which they had been selected for use as comparison subjects for metabolism and endocrinologic evaluations. Patients with anxiety disorders represented a subset of children (17 of 24) who were previously evaluated by means of a clonidine challenge
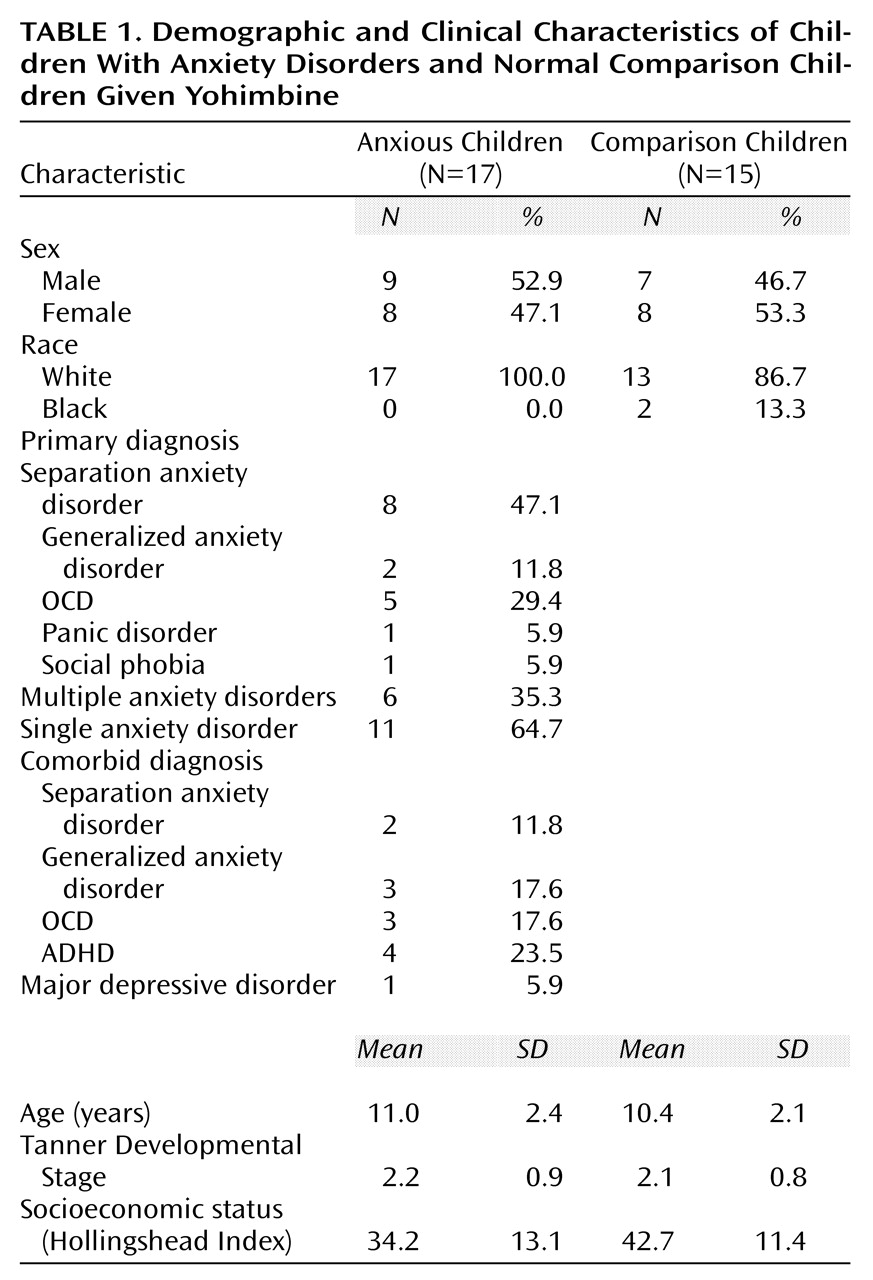
(15). Demographic characteristics of children with anxiety disorders and comparison children are presented in
Table 1. Patients received a structured clinical interview (Schedule for Affective Disorders and Schizophrenia for School-Age Children) modified for enhanced recognition of anxiety disorders
(28), which involved both parent and child interviews. Normal comparison subjects received a brief screening for lifetime psychiatric disorders. Comparison subjects were physically healthy and without anxiety, depression, or substance abuse and had a negative family history for affective or anxiety disorders. Diagnoses were derived from all available clinical information by consensus between a clinical psychologist and child psychiatrist.
Inclusion criteria were as follows: 1) male and female outpatients ranging in age from 7 to 14 years; 2) DSM-IV primary diagnosis of an anxiety disorder (e.g., separation anxiety disorder, panic disorder, generalized anxiety disorder, OCD, social phobia); 3) normal baseline laboratory results, negative urine drug screening, and normal physical examination; and 4) medication free for at least 2 weeks before the challenge (4 weeks for fluoxetine).
Exclusion criteria were as follows: 1) diagnosis of primary posttraumatic stress disorder or specific phobia; 2) meeting DSM-IV criteria for bipolar disorder, schizophrenia, anorexia or bulimia nervosa, or autism; 3) currently (within 6 months) known to abuse or to be dependent on any drug, including alcohol, or testing positive on a urine drug screening; 4) obese (weight for height greater than 95% on the National Center for Health Statistics curve) or severely malnourished (weight for height less than third percentile); or 5) unable to complete the required self-report measures or visual analog mood scale ratings.
Parents and/or guardians gave consent, and the children gave their assent in written form, as approved by the institutional review board of the Medical University of South Carolina, before study participation.
Assessments
Patients and comparison subjects received at baseline a battery of mood and anxiety ratings, including the Hamilton Anxiety Rating Scale
(29), the Revised Children’s Manifest Anxiety Scale
(30), the Childhood Anxiety Sensitivity Index
(31), and the Fear Survey Schedule for Children
(32). Subjects at baseline also received a physical examination (including Tanner staging) and an ECG. Immediately before and during the yohimbine challenge, children were instructed to complete a visual analog rating of mood states. The visual analog measure of mood states has the subject place a mark on a 100-millimeter line at a point between two opposing descriptors (i.e., not at all anxious to extremely anxious). Scores are measured in millimeters and range from 0 to 100. The measures of visual analog mood states used in this study were happy/cheerful, calm/relaxed, sad/depressed, energized/restless, and tense/anxious. The visual analog measure of mood states is highly reliable over short time frames, with correlations of repeated baseline measures ranging from 0.69 to 0.82 (p<0.0001)
(15).
Yohimbine Challenge
Children were admitted to a general clinical research center and maintained on a low monoamine diet for standardization before the initiation of the study. Meals were standardized and served at noon and 6:00 p.m. Activity was limited to bed rest during yohimbine administration, from 2:00 p.m. to 4:30 p.m. The evening before the yohimbine challenge, a 20–22-gauge cannulae was inserted into the child’s nondominant arm. Beginning at 2:00 p.m. and at 30-minute intervals through 4:30 p.m., 4.5 cc of blood was sampled (four samples) for hormonal analysis. At the same times, heart rate and blood pressure were recorded. Children completed the visual analog measure of mood states at 2:30 p.m. (just before yohimbine administration) and at 60, 90, and 120 minutes (after yohimbine administration). At 2:30 p.m., in the attendance of a parent or guardian, children were orally administered yohimbine, 0.1 mg/kg, in tablet form with 100 cc water. Dose was to the nearest 2.7 mg, rounding up to a maximum dose of 8.1 mg.
Hormone Determinations
Neuroendocrine blood samples were taken with disposable polypropylene syringes and immediately transferred to EDTA-containing tubes on ice. Those samples were transferred within 5 minutes to a polypropylene tube containing 650 trypsin inhibitor units of aprotinin and centrifuged at 1000 g for 5 minutes at 4°C; the plasma was transferred to a 1.5 ml tube containing n-ethylmaleimide and stored at –70°C until assay. (Aprotinin and n-ethylmaleimide were provided by Sigma, St. Louis). Plasma prolactin, GH, and cortisol were all obtained by using commercially available reagents from Nichols Institute Diagnostics (San Juan Capistrano, Calif.) by means of a chemiluminescence immunometric procedure. High, low, and mid-range external controls from Bio-Rad (Hercules, Calif.) were used in each run. The sensitivities of the prolactin, GH, and cortisol assays were 0.1 ng/ml, 0.02 ng/ml, and 0.8 mg/dl, respectively. The intraassay variabilities for prolactin, GH, and cortisol were 4%, 5%, and 8%, respectively; the interassay variances were 7.5%, 8.3%, and 7.8%, respectively.
Data Analysis
The visual analog measures of mood states and physiological and hormone data were analyzed by means of repeated measures analysis of variance (ANOVA) evaluating the effects of group, time, and interaction of group and time (incorporating the Greenhouse-Geisser adjustment for autocorrelation [33]). This analysis was applied directly to the postyohimbine change scores from baseline. In addition, for the visual analog measures of mood states and hormonal values, the index of maximum change (Δmax) from baseline was compared by using one-way ANOVA. Baseline for all analyses was considered as the last value collected before the administration of yohimbine. Type 1 errors for all analyses were controlled at 5%. Also, Bonferroni corrections for multiple comparisons
(34) were used for repeated measures ANOVA when the groups were broken down by primary diagnostic category. The Newman-Keuls test for multiple comparisons
(35) was used when comparing Δmax scores between groups broken down by primary diagnosis.
Results
Subject Baseline
The group with anxiety disorders, largely composed of children with a primary diagnosis of separation anxiety disorder, was similar to the group of comparison subjects in age, sex ratio, racial composition, and pubertal status (
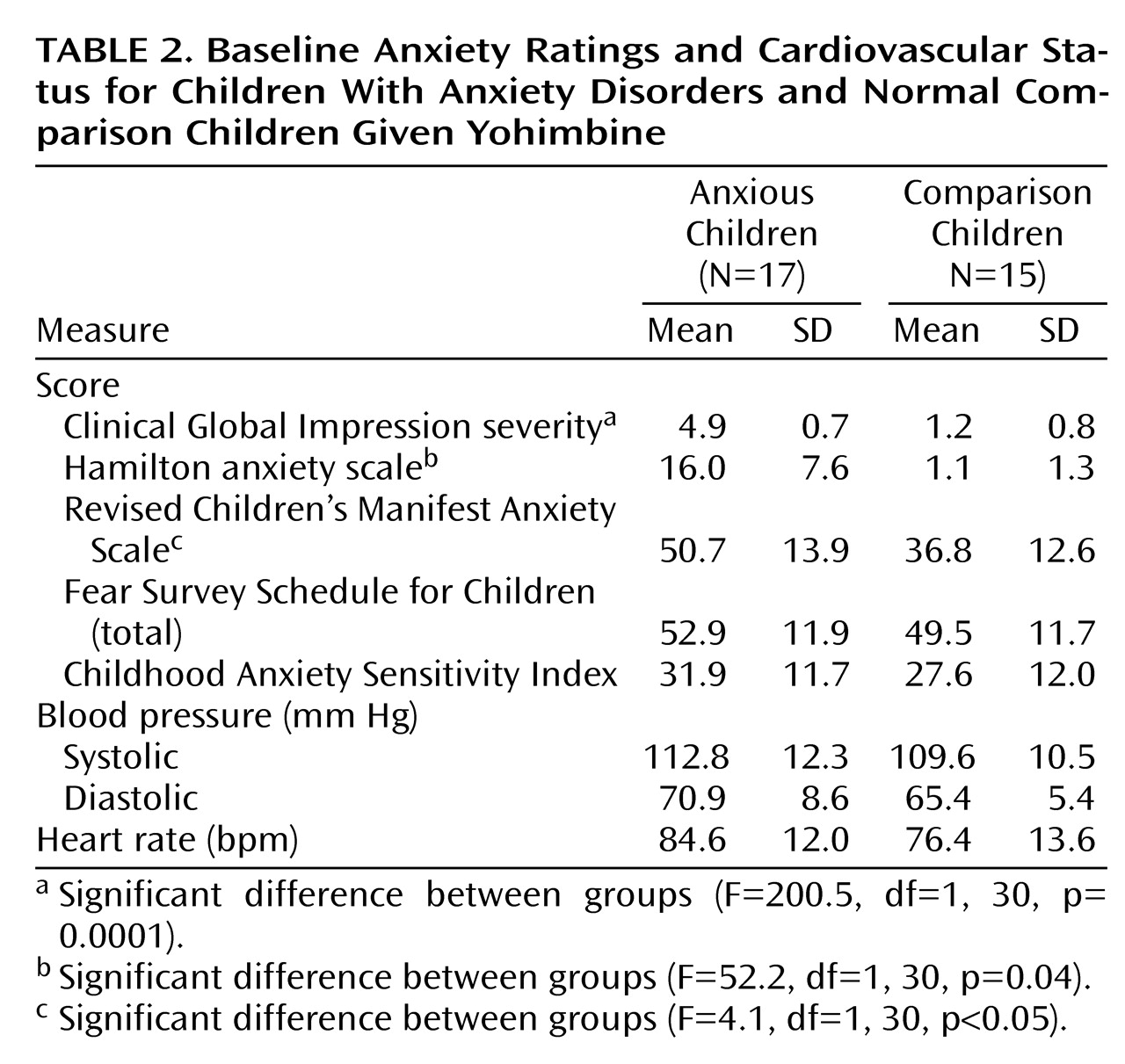
Table 1). The comparison group, however, scored higher on the Hollingshead Index of socioeconomic status (mean=42.7, SD=11.4) than the group with anxiety disorders (mean=34.2, SD=13.1), although this difference did not approach statistical significance. Distinguishing features between the children with anxiety disorders and comparison children were primarily the clinical and self-report measures of anxiety (
Table 2). The clinician-rated Clinical Global Impression (CGI) of anxiety severity and Hamilton anxiety scale scores differed markedly between children with anxiety disorders and comparison children. Self-ratings on the Revised Children’s Manifest Anxiety Scale also differentiated the two groups. Other self-ratings such as the Fear Survey Schedule for Children and the Childhood Anxiety Sensitivity Index, although elevated in the children with anxiety disorders, failed to approach statistical significance. Physiologic measures such as resting heart rate and blood pressure were not significantly different between groups. Baseline morning hormone plasma concentrations were not different between the groups for any hormone. Prolactin level for children with anxiety disorders (mean=7.7 ng/ml, SD=5.2) was comparable to that of comparison children (mean=7.6 ng/ml, SD=5.1). There was also no significant difference in baseline cortisol level for comparison children (mean=6.5 mg/ml, SD=2.8) compared to children with anxiety disorders (mean=9.1 mg/ml, SD=8.4). GH plasma concentration for comparison children (mean=1.9 ng/ml, SD=2.9) was also similar to that of children with anxiety disorders (mean=2.0 ng/ml, SD=3.4).
Yohimbine Challenge
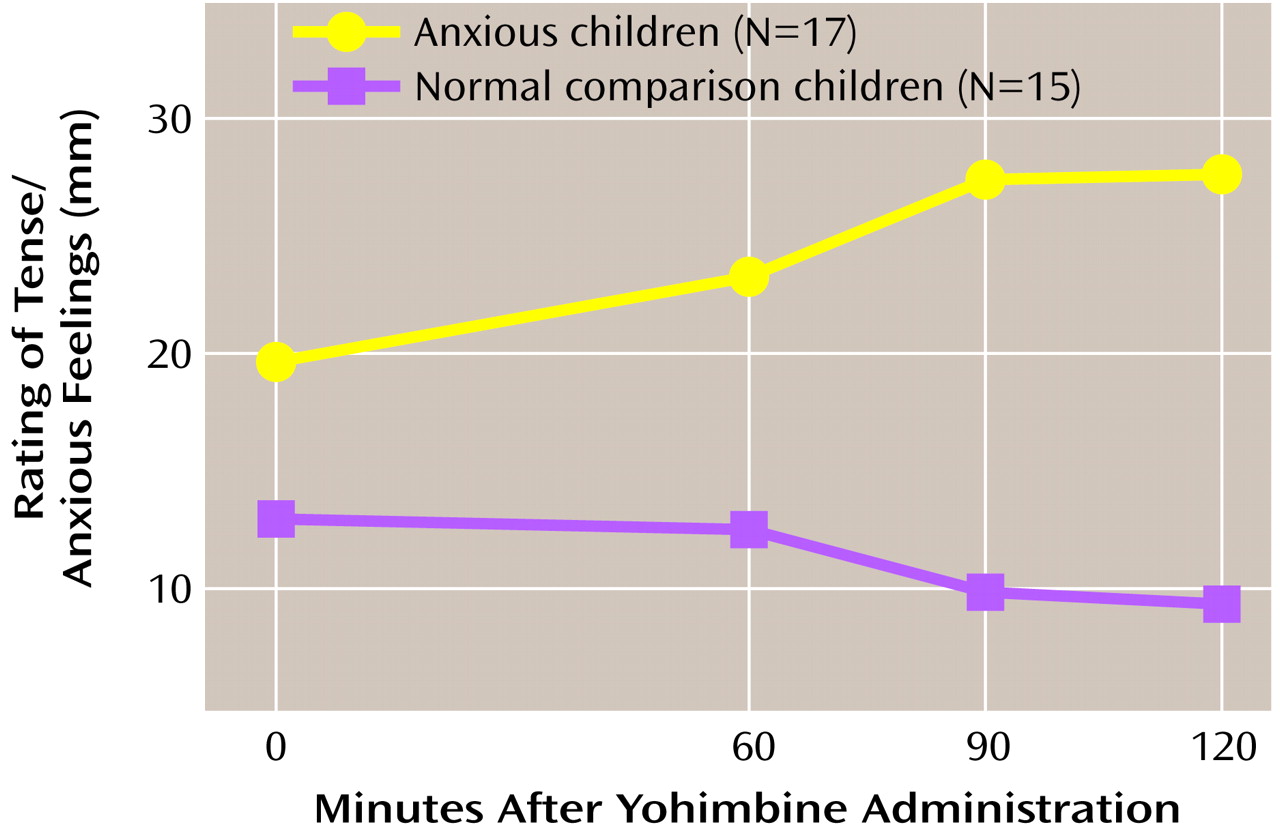
The mean administered dose of yohimbine was 4.4 mg (SD=1.6), with a median dose of 5.4 mg. Five subjects (three patients and two comparison subjects) experienced adverse events of dizziness (N=2) and stomachache (N=4) attributed to yohimbine. No child experienced a panic attack, but children with anxiety disorders did report increases in self-rated anxiety. The repeated measures ANOVA for tense/anxious ratings showed a significant group effect (F=4.1, df=1, 30, p=0.05, Greenhouse-Geisser corrected) (
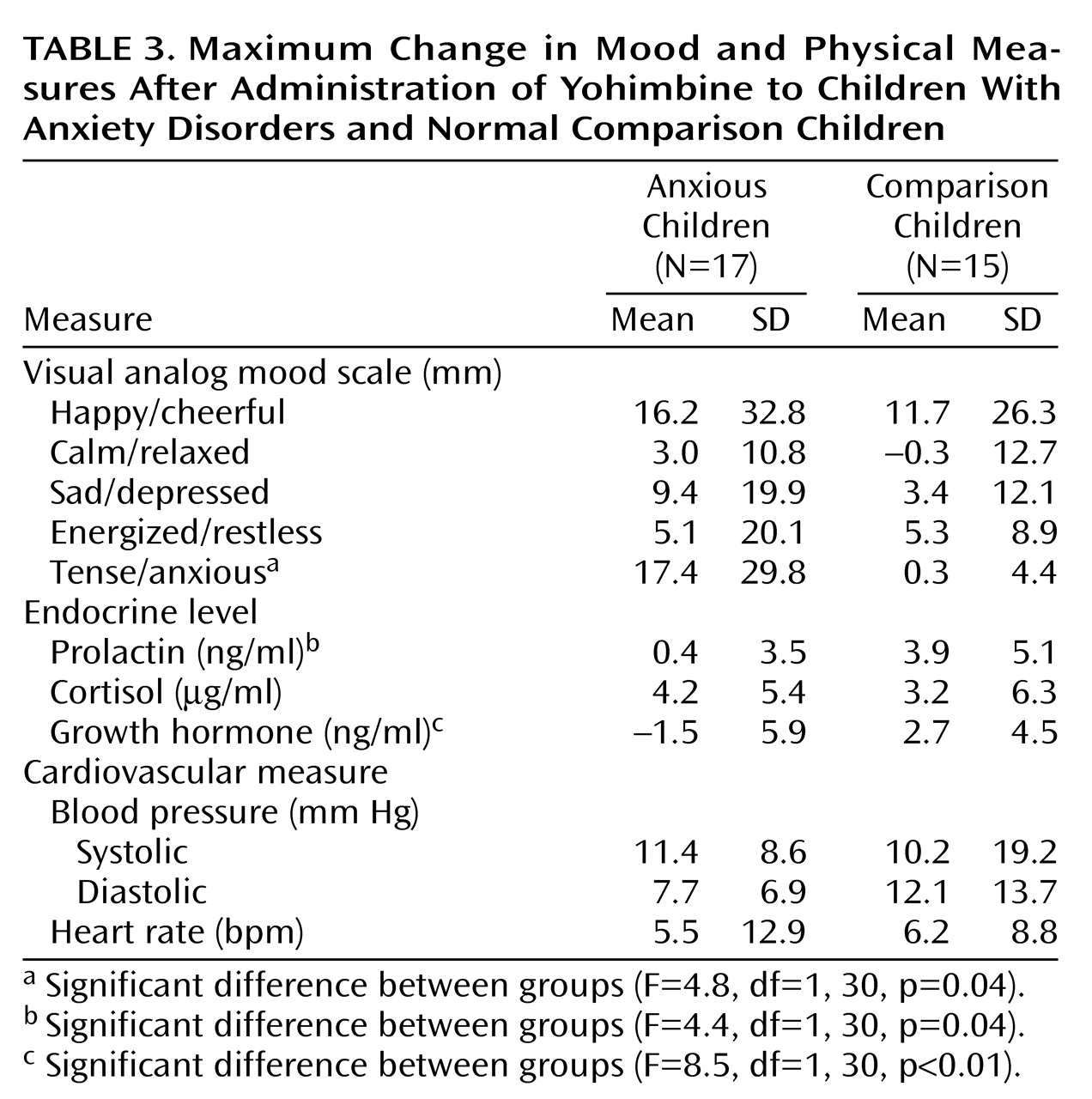
Figure 1). Neither the time effect nor the interaction of group and time was significant. The Δmax for tense/anxious ratings was also significantly different between groups (F=4.8, df=1, 30, p=0.04), with the children with anxiety disorders exhibiting greater Δmax than the comparison subjects (
Table 3). These yohimbine-related anxiety change ratings were not influenced by anxiety symptom severity (i.e., CGI and Hamilton anxiety scale scores). Loading for multiple anxiety disorders (N=6) did produce tense/anxious Δmax ratings twice that for children with a single anxiety disorder and tenfold higher than that of comparison subjects
Examining the largest subgroup of children with an anxiety disorder (i.e., separation anxiety disorder) by parceling out the OCD subset still demonstrated a robust group effect on tense/anxious scale scores (F=4.8, df=2, 29, p=0.02, repeated measures ANOVA, Greenhouse-Geisser corrected). Neither the time effect nor the interaction of group and time was significant. The group with separation anxiety disorder exhibited higher tense/anxious ratings than the comparison subjects (F=4.8, df=1, 20, p=0.04), but this was not significant after use of the Bonferroni correction for multiple comparisons. The tense/anxious Δmax value for children with separation anxiety disorder (mean=28.1 mm, SD=36.8) was also dramatically higher than that found in children with OCD (mean=3.6 mm, SD=4.9) (Newman-Keuls post hoc test p<0.05).
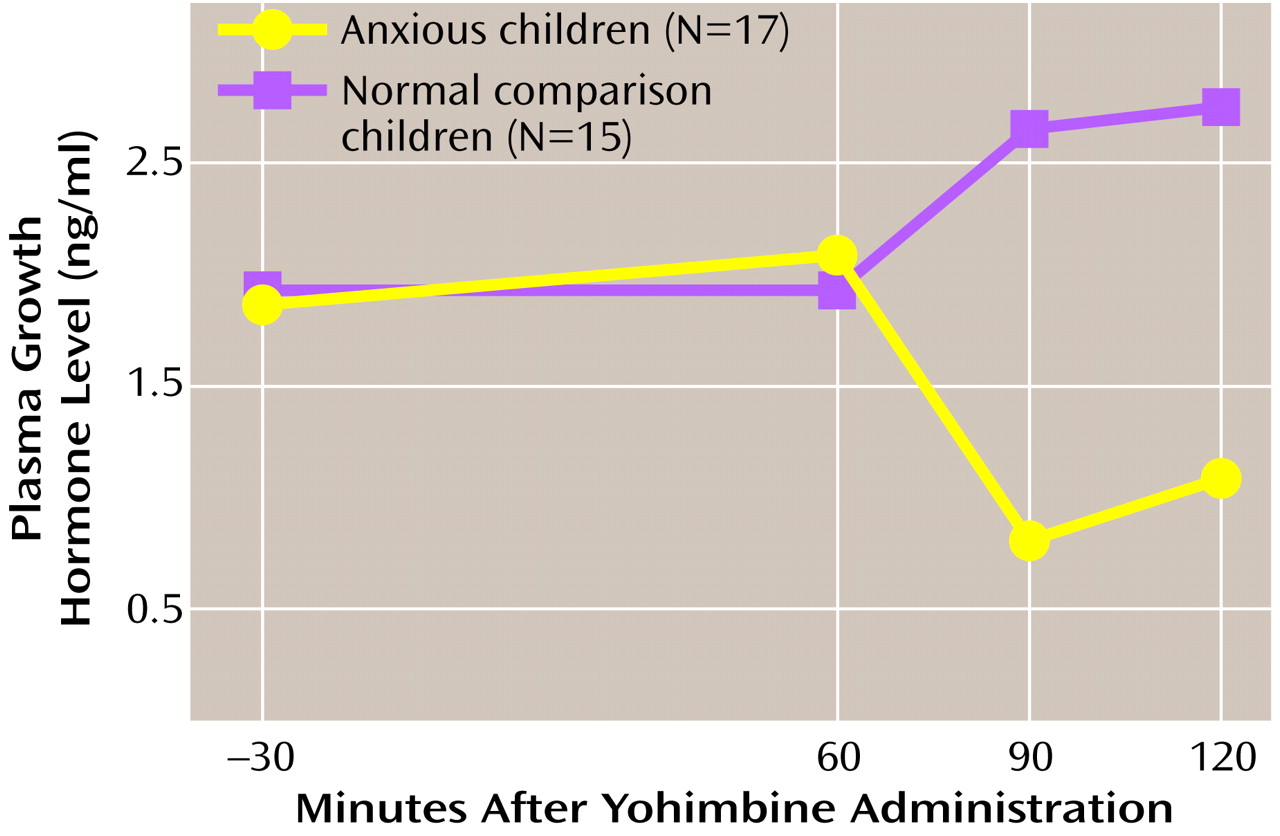
The repeated measures ANOVA of GH response to yohimbine for children with anxiety disorders versus that of comparison children revealed a significant group effect (F=4.2, df=1, 30, p=0.05, Greenhouse-Geisser corrected) (
Figure 2). Neither the time effect nor the interaction of group and time was significant. The associated Δmax GH levels were also significantly different between groups (F=4.1, df=1, 30, p=0.05), with the children with anxiety disorders demonstrating blunting relative to the comparison children (
Table 3). Blunting of GH was not different between subgroups with separation anxiety disorder (mean=–1.8 ng/ml, SD=6.5) and OCD (mean=–1.1 ng/ml, SD=5.5). Neither anxiety symptom severity nor loading for anxiety disorders had any effect on yohimbine-related GH response. Yohimbine-related cortisol output did not differentiate between groups. Prolactin Δmax did distinguish the children with anxiety disorders (mean=0.4 ng/ml, SD=3.5) from comparison children (mean=3.9 ng/ml, SD=5.1) (F=4.4, df=1, 30, p=0.04) (
Table 3), but the repeated measures analysis did not demonstrate a significant difference between the groups.
Heart rates revealed an effect of time by repeated measures analysis, with all subjects showing an increased heart rate (F=3.6, df=2, 60, p=0.03). Neither the group effect nor the interaction of group and time was significant for heart rate. An effect of time on diastolic blood pressure was also evident, with elevations in all subjects (F=3.3, df=2, 60, p=0.03). Neither the group effect nor the interaction of group and time was significant for diastolic blood pressure. Repeated measures analysis of heart rate and blood pressure and Δmax relative to baseline did not distinguish between groups. High intersubject variability in both systolic and diastolic blood pressure change after yohimbine administration was encountered, however, in the comparison group.
Discussion
Previous findings related to a clonidine challenge in children with anxiety disorders
(15) are now supplemented with data from this yohimbine challenge, which demonstrated increased sensitivity in the same patients. This increased responsivity to yohimbine is further magnified in separation anxiety disorder relative to other anxiety disorders such as OCD. Prepubertal children with separation anxiety disorder exhibited an enhanced response to a range of unconditional stimuli, including yohimbine, before the developmental period encompassing risk for spontaneous panic attacks
(6,
12). The response of children with anxiety disorders to yohimbine is consistent with the overactivity of noradrenergic outflow. This overactivity has been attributed to decreased sensitivity of the a
2 adrenergic autoreceptor, which may leave the system less adaptable to inhibitory feedback of norepinephrine in the synapse
(22). The present finding of yohimbine-related GH blunting in children with anxiety disorders is consistent with the literature for the same challenge in adults with anxiety disorders
(22,
36). The apparent absence of GH blunting on challenge with clonidine in childhood anxiety disorders, however, differs substantially from the findings in adult anxiety disorders
(21,
23,
27,
37). The two challenge findings together suggest that presynaptic norepinephrine sensitivity is present in early-onset anxiety disorders, but an overactive noradrenergic system is not necessarily accompanied by a
2 adrenoceptor down-regulation. Speculation regarding the developmental trajectory for a
2 adrenoceptor down-regulation cannot be supported, however, by any of the child challenge studies because of their cross-sectional design.
Studies profiling a wide variety of challenges, including those using clonidine, yohimbine, caffeine, glucose, GH-releasing factor, and thyrotropin-releasing hormone, have suggested a hypothalamo-GH dysfunction in adult panic disorder
(36,
38). Uhde et al.
(36) have raised the possibility that panic disorder may be associated with previously unrecognized disturbances of growth in prepubertal children. The authors cite the convergence of childhood panic disorder with disturbances of stature. From another perspective, adults who had been GH deficient as children demonstrated an increased incidence of anxiety disorders such as social phobia
(39). Pine et al.
(40) have provided some support for this concept from a prospective study in which various childhood anxiety disorders predicted a 1–2-inch decrement in adult stature in women but not in men. The present yohimbine-related GH data in childhood anxiety disorders is also consistent with hypothalamo-GH dysfunction, but clonidine challenge data
(15) do not support this hypothesis.
From a developmental perspective, characteristic behavioral and neuroendocrine responses to a yohimbine challenge appear to be present early in the onset of anxiety disorders. These responses do not appear to be state related because neither is correlated with symptom severity or Hamilton anxiety scale scores. The behavioral response to yohimbine administration does demonstrate diagnostic specificity because the response in children with separation anxiety disorder is far more robust than in children with OCD. Furthermore, yohimbine sensitivity reflected by self-reported anxiety is heightened in the presence of multiple anxiety disorder diagnoses. Loading for anxiety disorder (i.e., multiple anxiety diagnoses) tends to track with genetic loading and family history of anxiety disorders. Fully 33% of the group with anxiety disorders had a first-degree relative (i.e., mother, father, or sibling) with an anxiety disorder diagnosis. Just as CO
2 sensitivity varies by family loading, demonstrates diagnostic specificity for panic disorder, and may confer risk for the development of panic disorder in children with separation anxiety disorder
(15), yohimbine appears to define another physiologic continuum by which this phenotype can be characterized. Because the most frequent diagnosis in the anxiety group was separation anxiety disorder, characteristic enhanced sensitivity to yohimbine and other unconditioned stimuli in separation anxiety disorder may antedate the onset of panic disorder and potentially constitute a necessary but not sufficient precursor for the development of panic disorder. It should be reiterated that no child in this study, including the lone subject with panic disorder, experienced a panic attack. Yohimbine sensitivity, however, was indicated by the perception in even prepubertal children of increased tension/anxiety.
Several factors may account for protection from panic attacks in our study group, the most obvious of which is prepubertal status
(1). Another protective factor is attendance of an attachment figure during the challenge (i.e., proximity to a “safe person”
[41]). Finally, the stage of cognitive development appears to be critical
(1,
42). The construct of “anxiety sensitivity” (fear of bodily sensations perceived as heralding a catastrophic event), a risk factor for adult anxiety disorders, is only evident in children 12 years and older in concert with cognitive developmental predictions
(31). Although norepinephrine sensitivity in children with anxiety disorders, demonstrated by a yohimbine challenge, is a biological vulnerability, interaction with environmental and constitutional factors such as attachment milieu
(43) and temperament
(1) must be present for the development of panic disorder or anxiety disorders.
Although challenge strategies are controversial, the performance of the yohimbine challenge was well tolerated in both the children with anxiety disorders and the comparison children. Subjects and their guardians who elected to participate in the yohimbine challenge had the advantage of extensive informational meetings, prior positive experience by the child in a clonidine infusion paradigm, and close monitoring as well as supervision during and after the challenge. Challenge studies remain vitally important in defining a phenotype, in elucidating biological diatheses amenable to therapeutic manipulation, and for identifying risk factors potentially influencing developmental progression of the disease from separation anxiety disorder to panic disorder. From this perspective, intervention and prevention strategies may be directed at those factors necessary and specific to this progression. If we speculate with the present yohimbine findings along with clonidine challenge data in children with anxiety disorders, it would be those factors crucial to the development of a2 adrenoceptor down-regulation that should be the focus of future studies.