Many studies, using a variety of scales, have assessed body image perception in women
(1). A well-known finding of these studies is that women with eating disorders, such as anorexia nervosa and bulimia nervosa, typically perceive themselves to be fatter than they actually are and often aspire to unrealistic levels of thinness
(2). By contrast, the literature on body image perception in men is far more limited, and the available scales are less well developed
(3–
6). However, accumulating evidence suggests that many men also suffer from disorders characterized by altered perceptions of their bodies. For example, in two studies, both American men
(7) and European men
(8) with eating disorders rated themselves as feeling significantly fatter than subjects without eating disorders. Also, recent studies of athletes have described a converse syndrome: men who perceive themselves as small and frail when in fact they are large and muscular. We have previously called this syndrome “reverse anorexia nervosa”
(9) and have subsequently renamed it “muscle dysmorphia”
(10). Individuals with muscle dysmorphia may exhibit striking psychiatric morbidity. For example, they may refuse to allow their bodies to be seen in public settings; they may relinquish important social, recreational, or occupational activities to work out compulsively at the gym; and they may abuse anabolic steroids in an attempt to overcome their chronic preoccupation that they look too small.
Given these observations of men with various forms of body image pathology, it is of interest to assess body image perception in unselected groups of men. In recent decades, men in Western societies have been exposed through the media to an increasingly lean and muscular male body ideal
(11,
12). Therefore, we hypothesized that in both the United States and Europe, men would desire to have a body much leaner and more muscular than the body that they actually had or the body that they perceived themselves to have. We also hypothesized that men would think that women in their societies preferred a very lean and muscular male body. We believed, however, that men’s estimates of women’s preferences might differ from women’s actual preferences.
To test these hypotheses, we developed a computerized instrument, the somatomorphic matrix, to measure body image perception in both general and clinical populations. We developed both male and female versions of this instrument, as described in detail elsewhere
(13). The male version of the test contains a computerized library of 100 images of men, arranged in a 10 × 10 matrix, representing 10 degrees of fatness and 10 degrees of muscularity. A graphic artist constructed the images, using reference photographs of actual men whom we had carefully measured. On the fatness axis, the images begin at a percentage of body fat of 4% (approximately the minimum figure attainable in men) and increase in increments of 4% to a maximum of 40% (a very obese man). On the axis of muscularity, the images are calibrated on the basis of a fat-free mass index (FFMI), an index of muscularity that we developed and have described elsewhere
(14). Briefly, a typical 30-year-old man has an FFMI of approximately 20 kg/m
2; a man with an FFMI of 18 kg/m
2 would appear somewhat frail, whereas a man with an FFMI of 22 kg/m
2 would appear distinctly muscular. An FFMI of 25–26 kg/m
2 represents approximately the upper limit of muscularity that can be achieved by a lean individual without the use of anabolic steroids or similar drugs. With anabolic steroids, however, the FFMI may extend much higher, reaching well into the 30s for some competition bodybuilders
(14). In the somatomorphic matrix, the images begin at an FFMI of 16.5 kg/m
2 and increase in increments of 1.5 kg/m
2 to a maximum FFMI of 30.0 kg/m
2. The resulting 10 × 10 matrix of images thus spans a wide range of body shapes from which a subject may select when using this instrument. A major advantage of the somatomorphic matrix is that the images vary along axes of both fat and muscularity, rather than along a single nonspecific axis of increasing size, as has been the case with most earlier scales measuring body image perception.
The somatomorphic matrix runs on a laptop computer. The instrument first asks the subject to indicate his gender and to select the language of his choice (English, French, German, or Spanish) and then requests basic demographic information. The computer then presents the subject with a sample male body image from the middle of its library (with 20% body fat and an FFMI of 22.5 kg/m2). Nearby “buttons” on the screen allow the subject to vary the fat and muscularity of the image upward or downward independently. The computer then poses four standard questions: 1) choose the image that best represents your own body, 2) choose the image that represents the body that you ideally would like to have, 3) choose the image that represents the body of an average man of your age, and 4) choose the image that represents the body most desired by the opposite sex. In each case, the subject scrolls through the images until he has chosen the image that he feels best answers the question. At that point, he clicks a button entitled “select this image.” The computer then stores his answer to the question, restores the median image to the screen, and poses the next question in the series.
In a pilot study using the somatomorphic matrix, we examined 44 men at a gymnasium in suburban Boston in the United States
(13). Because these men were regular weightlifters, they were quite muscular, with a mean FFMI of 22.7 kg/m
2. Remarkably, however, their mean desired degree of muscularity was much higher, at 24.6 kg/m
2. In other words, these men wanted to have about 16 lb (7 kg) of additional muscle beyond the substantial amount that they already possessed.
It was not clear, however, whether this striking discrepancy would extend to ordinary men not selected for weightlifting, and whether there might be differences between American men and European men in measures of body image perception. Accordingly, we administered the somatomorphic matrix to unselected samples of college men in three countries.
Method
We conducted the study at three sites: the University of Innsbruck in Innsbruck, Austria; the Salpêtrière Hospital in Paris, France; and an urban university in Boston. At each site, we recruited undergraduate college students using posted advertisements, by announcements in classes, and by word of mouth. We told students that we were conducting a study examining perceptions of body image by using a brief computerized test. We informed them that we would also measure their height, weight, and body fat. We required all students to sign informed consent for the study. The study and the original consent form in English were approved by the McLean Hospital institutional review board; the consent form was then translated into German and French, respectively, and reviewed for accuracy by native speakers of each language. Subjects at all three sites were asked to sign the informed consent form in their native language. For participation in the study, which required approximately 10–15 minutes, we gave students in Austria 100 Austrian shillings, students in France 100 French francs, and students in the United States 10 American dollars. All college men who wished to participate in the study were accepted; subjects were not screened for the presence or absence of body image disorders or other psychopathology.
Students reporting to the test location were first seen by one of the investigators to measure their height, weight, and body fat. We determined body fat by measuring six skinfolds with calipers (triceps, subscapular, chest, suprailiac, abdomen, and thigh) and then entering the sum of these six skinfolds into the equation developed by Jackson and Pollock
(15):

where BF is body fat,
x is the sum of the six skinfolds, and
y is the subject’s age in years. Because all of the body images in the computer were standardized to an assumed age of 30 years
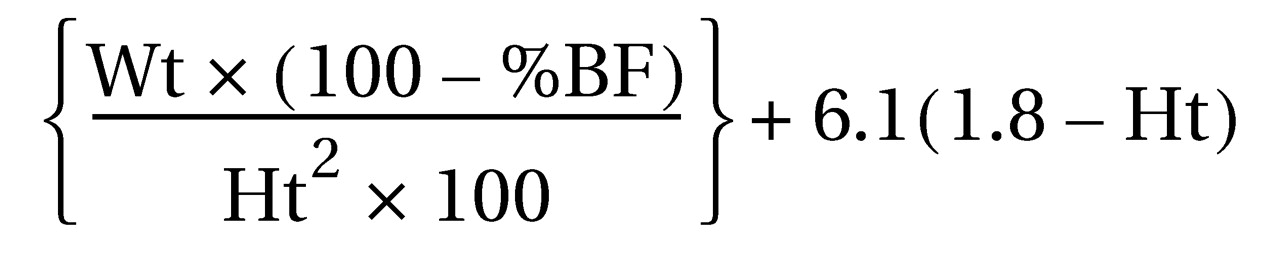
(1), we adjusted the body fat calculation of all students to an assumed age of 30 years for the purposes of uniformity. To do this, we set y in the above equation to 30 for all men, yielding the following simplified formula for adjusted body fat:

For example, if a 22-year-old student had a true measured body fat of 13%, his adjusted body fat for the purposes of this paper would be quoted as 14.1%. The reason for this adjustment is that older individuals carry a smaller proportion of their fat on the surface of their bodies than younger individuals
(15). Thus, the body outline of a 22-year-old student with a body fat of 13% would appear similar to that of a 30-year-old individual with a body fat of 14.1%, even though the latter individual was technically fatter. By adjusting the body fat of all subjects to age 30, we insured uniformity among the subjects and the computer images with regard to the body’s surface appearance.
Next, using each subject’s height, weight, and percentage of body fat, we calculated his FFMI by using an equation that we developed previously
(14):
where Ht=height in m, Wt=weight in kg, and %BF=percentage of body fat (again adjusted to age 30).
After these measurements, each subject took the somatomorphic matrix test, where he was asked to choose images in response to each of the four questions listed earlier. Thus, for each subject, we obtained five measures: 1) his actual body fat and muscularity (as expressed by FFMI), 2) his perception of what he thought his fat and muscularity looked like, 3) the level of fat and muscularity that he ideally desired to have, 4) his judgment of the level of fat and muscularity of an average man of his age in his society, and 5) his judgment of the level of fat and muscularity of the male body that women would prefer. It should be noted that this last question was asked regardless of the subject’s sexual orientation; thus, although most of the subjects were presumably heterosexual, occasionally a homosexual subject was also asked to estimate women’s preferences for the male body.
We evaluated the differences in means for demographic measures among the three countries using ANOVA, with Tukey’s post hoc test for pairwise comparisons. We then evaluated the differences in means for the five indices of percentage of body fat and FFMI (measured, perceived, average man, desired ideal, and women’s preference) using a random effects regression model
(16) in SAS PROC MIXED
(17). In these two regression analyses, the model for the mean used percentage of body fat and FFMI, respectively, as the two outcomes. Specifically, the main effects model for an individual subject was:
E(Yij)=β0 + β1 PERi + β2 AVEi + β3 DESi + β4 WPRi + β5 FRAj + β6 AUSj
where E(Yij) is the expected value of the outcome of interest (body fat or FFMI) of the ith observation (i=1,…5) of a subject from country j (j=1, 2, 3), the coefficients of the parameters β1 – β4 are indicator variables for body fat indices of the ith observation (PER=perceived, AVE=average man, DES=desired ideal, WPR=women’s preference), and the coefficients of β5 and β6 are indicators for the individual’s country (AUS=Austria, FRA=France).
In this model, β0 represents the expected value of measured body fat or FFMI in an American subject, and β1 represents the increase in perceived body fat or FFMI relative to measured body fat or FFMI in an American subject.
Because observations within individuals are correlated, we used PROC MIXED to model the structure of this correlation. We used the method of empirical variances
(16) to estimate the standard errors, with compound symmetry as the working covariance structure. We first fitted a model with eight additional terms for the interaction of index and country. In cases where this interaction was significant (by the likelihood ratio test by using maximum likelihood estimation), we tested the significance of the main effect of index, using the chi-square test, for each country separately. If this interaction was not significant, we used a final model without interaction terms and tested the significance of the main effects of country and index by the chi-square test. In reporting the results, we have presented estimates of the increase in the outcome measure (percentage of body fat or FFMI) and their associated 95% confidence intervals (by using the standard error calculated by the method of empirical variances) relative to the measured category (that is, measured percentage of body fat or measured FFMI). We evaluated the significance of differences between individual indices using Tukey’s method to adjust for multiple pairwise comparisons.
Results
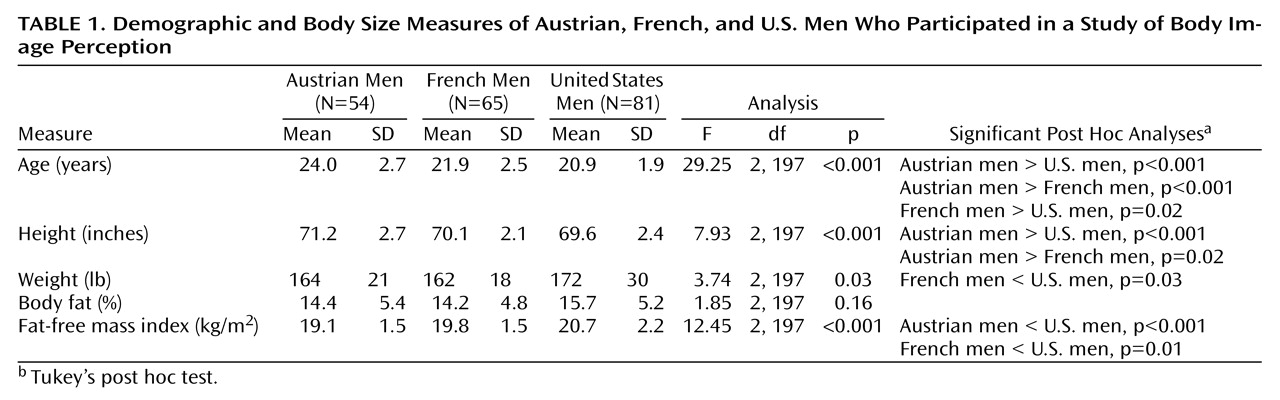
Study participants included 54 men in Austria, 65 men in France, and 81 men in United States. The demographic and body size features of these three groups are shown in
Table 1. The Austrians were notably older than the other two groups, because many Austrians do not graduate from college until their mid 20s. The Americans were somewhat shorter, fatter, and more muscular than their European counterparts (
Table 1).
In general, subjects commented that they had little difficulty distinguishing between serial images in the computer’s library and that they could easily choose suitable images in response to the various questions. A few subjects complained that the computer offered images with only a single body type, with relatively broad shoulders, compared to the waist or hips. Thus, men whose upper body was small relative to their lower body (for example, soccer players) sometimes found that none of the images corresponded exactly to their own proportions. In such cases, we asked the subject to do his best, recognizing that the images were not ideally suited to his own body type.
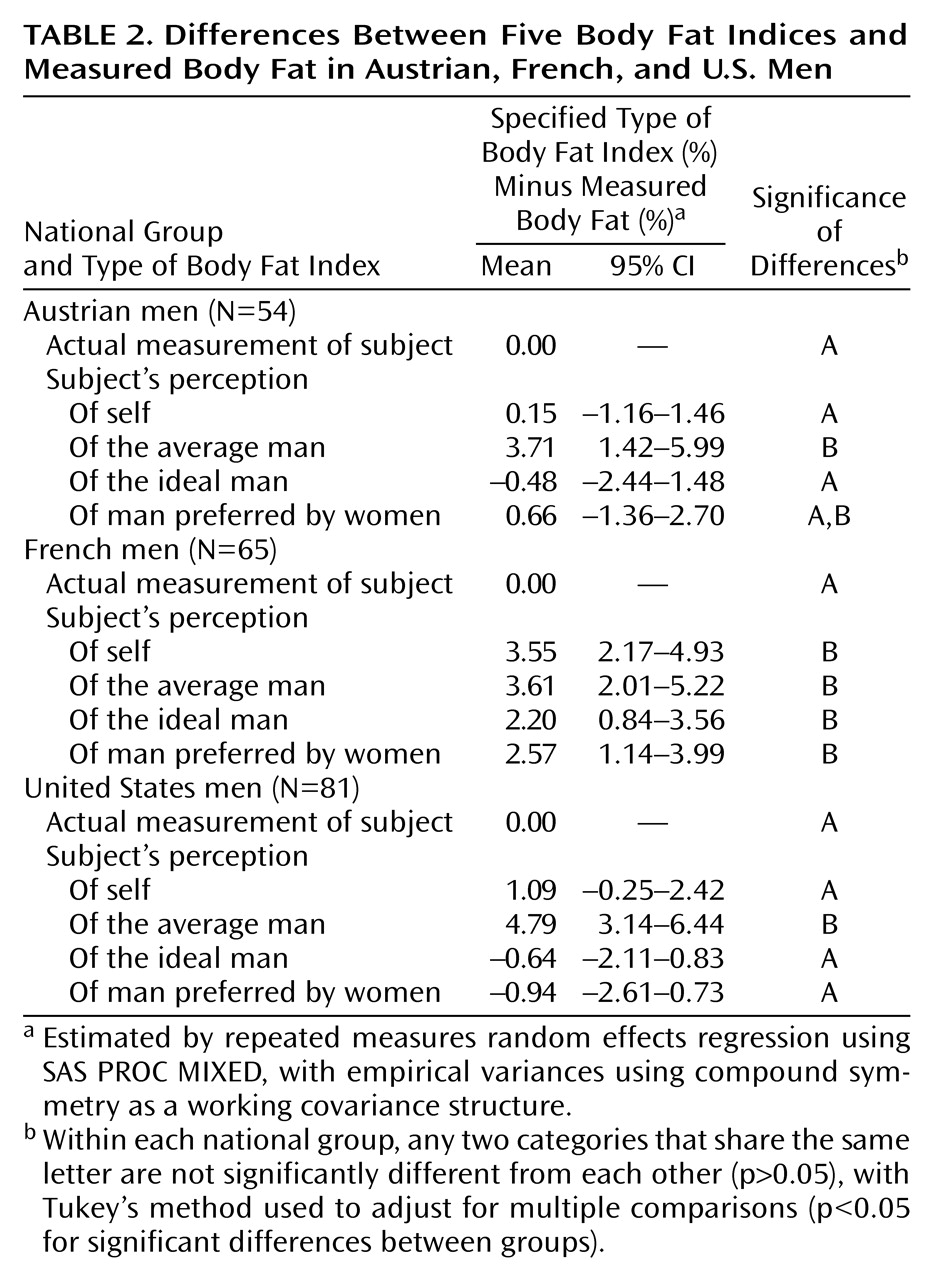
The analysis of the body fat indices yielded a significant interaction of index and country (likelihood ratio test, χ
2=23.1, df=8, p<0.001). Therefore, data from
Table 2> compares the subjects’ mean measured body fat with the mean levels of body fat chosen in response to each of the computer’s four questions for each country. In Austria and the United States, there were few differences between the subjects’ actual measured body fat and the levels of body fat chosen on the computer questions, except that both the Austrians and the Americans felt that an average man of their age was slightly, but significantly, fatter than themselves. In France, by contrast, the mean measured body fat of the subjects was significantly lower than that of the images chosen in response to the four questions. However, even the differences that achieved statistical significance in
Table 2 were modest, in that a difference of 3%–4% in body fat is quite small
(15) and often barely noticeable to the eye.
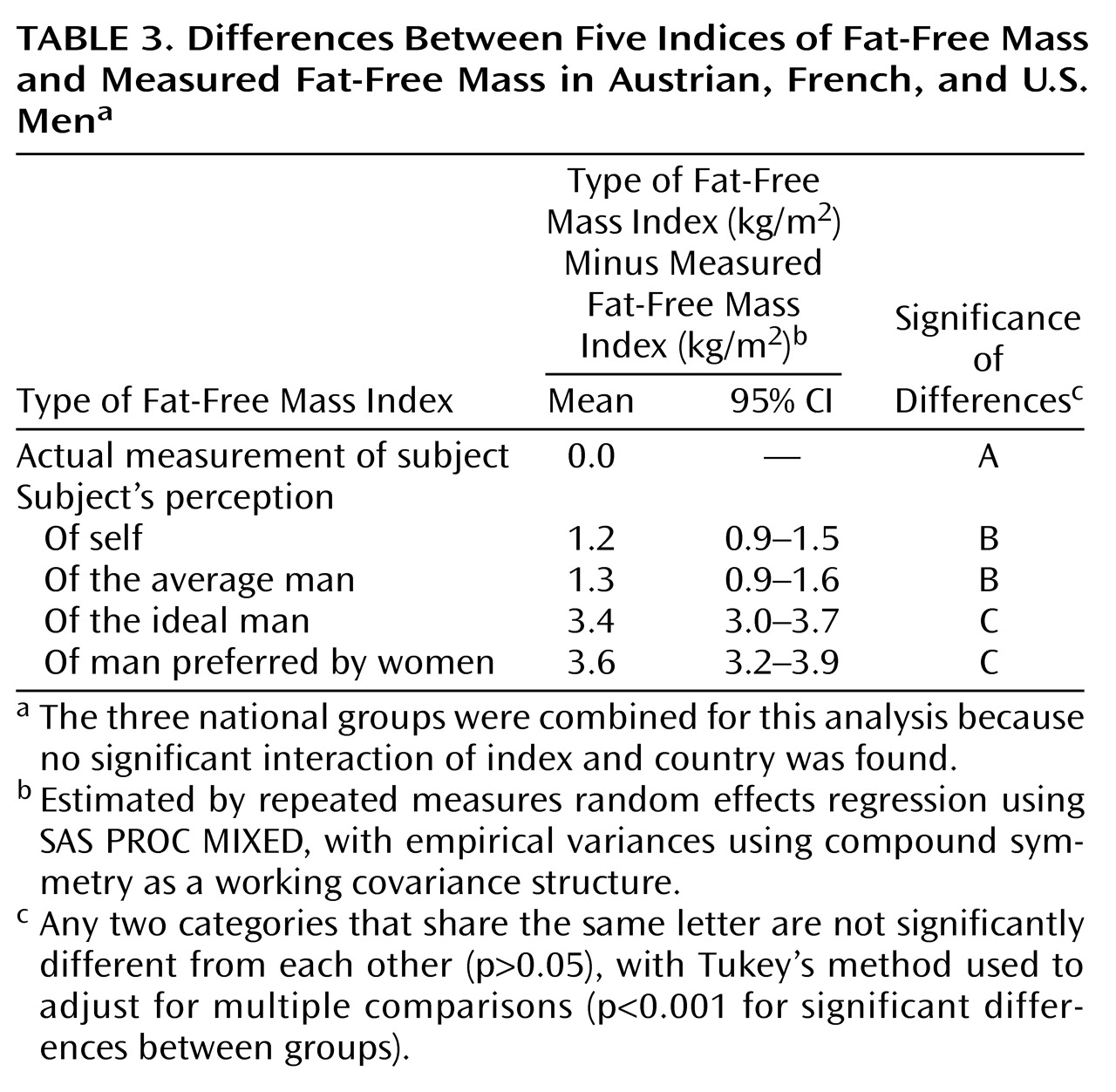
Much more striking differences emerged on measures of muscularity, as reflected by the FFMI. In this analysis, we found no significant interaction of index and country (likelihood ratio test, χ2=12.5, df=8, p=0.13) and therefore we fitted a final model without terms for the interaction. We observed significant main effects for country (χ2=17.4, df=2, p<0.001) and for index (χ2=141.0, df=4, p<0.001). Examining the country effect, Austrian men had significantly lower measures of FFMI across all indices than French men (p=0.003, Tukey’s test), who in turn had significantly lower measures of FFMI than American men (p=0.01, Tukey’s test). The estimated decrease in FFMI across all categories, relative to American men, was 1.8 kg/m2 (95% confidence interval [CI]=1.2–2.3) for Austrian men and 0.7 kg/m2 (95% CI=0.2–1.3) for French men.
Turning to an analysis of the index effect, the men in all three countries perceived themselves to be significantly, but only modestly, more muscular than they actually were (
Table 3). However, these differences were small in comparison to the differences elicited by the questions regarding the degree of muscularity that these men would ideally like to have. As can be seen from the fourth row of
Table 3, the three groups of men ideally wanted to have an FFMI of 3.4 kg/m
2 greater than they actually had. This means that they wanted to have an additional 27–29 lb (12–13 kg) of muscle on their bodies. Even more remarkably, as indicated in the fifth row of
Table 3, they estimated that women in their respective countries would prefer them to have 27–32 lb (12–14 kg) of additional muscle.
Intrigued by the men’s ambitious estimates of the male body that women would prefer, we presented the images in the somatomorphic matrix to 43 college women at the Austrian site and asked them to choose the male body that they liked the most. The images chosen by these women had a mean percentage of body fat of 14.9% (SD=5.3%) and an FFMI of 20.3 kg/m2 (SD=1.6). In other words, the women did not choose a muscular body image but instead preferred a man who looked very much like an actual average man in their country. Expressed in numerical terms, the body that Austrian men thought that women preferred was approximately 21 lb more muscular than the body that Austrian women actually preferred. Although we have not formally presented the somatomorphic matrix to large samples of women in Paris or Boston, our anecdotal experience with the instrument in these countries suggests that the findings would be similar to those observed in Austria.
Discussion
We developed a biaxial computerized measure of body image perception, the somatomorphic matrix, and assessed body image perception among unselected male college students in Innsbruck, Austria; Paris; and Boston. On actual body measurements and on indices of perceived body fat, only modest differences were found. Striking findings, however, emerged on indices of muscularity. In particular, the men in all three countries indicated that they would like—and they believed that women would prefer—a body with at least 27 lb (12 kg) more muscle than they actually had. By contrast, actual women indicated that they preferred a very ordinary looking male body. Thus, in both the United States and Europe, there appears to be a striking discrepancy between the body that men think women like and the body that women actually like.
Several limitations of the study should be considered. First, the college students who volunteered to participate in the study may not have been representative of college students in their countries as a whole. Probably the most likely form of selection bias was that individuals dissatisfied or embarrassed with their bodily appearance were less likely to participate. If so, then the study may actually have underestimated the true disparity between men’s actual appearance and the appearance that they ideally desired.
A second limitation of the study is that the computer images only approximated the dimensions of actual men at each level of body fat and muscularity. However, this source of error seems unlikely to have seriously biased the findings. Specifically, had the somatomorphic matrix contributed a systematic error, this error would have affected equally the subject’s choice of images in response to the various questions, so that the differences between question responses would still remain valid. Alternatively, if the somatomorphic matrix contributed random error, this error would simply tend to produce overly conservative findings, since it would introduce noise into the comparisons between various measures.
On balance, then, the marked differences between the actual muscularity of these men, the levels of muscularity that they desired, and the levels that they thought were preferred by women appear unlikely to represent artifactual findings. The reasons for these differences, however, remain unclear. One possible hypothesis is that modern Western young men are constantly exposed—through television, movies, magazines, and other sources—to an idealized male body image that is far more muscular than an average man
(12). We have offered tentative evidence for this hypothesis in an earlier investigation, where we demonstrated that action toys—the small plastic figures used by young boys in play, such as GI Joe and Star Wars figures—have grown dramatically more muscular over the last 20 to 30 years
(11). A similar evolution seems to have occurred in Hollywood movies: the most masculine male stars of the 1940s and 1950s were clearly less muscular than many of the modern action heroes of today’s films. Certainly these action toys, films, and other potential sources of cultural body image ideals are as accessible to Western European men as to American men.
If this hypothesis concerning cultural message is correct, the findings of the study reported here may warn of a widening gulf between the average Western man’s body and the more muscular ideal to which he aspires. As body ideal moves steadily away from body reality, some vulnerable men may be more likely to develop muscle dysmorphia
(10), anabolic steroid abuse or dependence
(18,
19), or other psychiatric disorders. Further research using the somatomorphic matrix, particularly in populations less influenced by Western body ideals, may be useful to test this hypothesis.