Subjects were recruited by consecutive new-case ascertainment from pediatric and psychiatric sites
(3,
4). A method for differentiating prepubertal and early adolescent bipolar disorder phenotype from attention deficit hyperactivity disorder (ADHD) was needed, because symptoms such as hyperactivity and distractibility are criteria for both mania and ADHD. To address this need, the prepubertal and early adolescent bipolar disorder phenotype required current mania or hypomania with elation and/or grandiosity as one criterion
(3–
5). Use of this phenotype permitted a diagnosis of mania without the use of the criteria that overlapped with those for ADHD, ensured that subjects had at least one of the two cardinal features of mania (i.e., elation and grandiosity), and allowed investigation of a child phenotype that was most likely to be continuous with adult bipolar disorder
(3–
5).
A comprehensive battery was given at baseline and at 6 and 12 months to mothers and children separately. Research nurses were blinded to the subjects’ diagnosis at baseline because the subjects with the prepubertal and early adolescent bipolar disorder phenotype were interviewed concurrently with two comparison groups without bipolar disorder
(3,
4). Psychopathology was assessed with a semi-structured interview, the Washington University in St. Louis Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U-KSADS)
(4,
6), and in consensus conferences that examined all research, school, and medical records. Research nurses were trained to 100% interrater reliability on five consecutive interviews (as both interviewer and observer) for each WASH-U-KSADS item
(6). In addition, interrater reliability between on-site WASH-U-KSADS mania ratings and off-site blind ratings (made on the basis of the narrative documentation that accompanies each WASH-U-KSADS mania item) were excellent (kappa=0.74–1.00)
(6). Six-month stability of both bipolar disorder diagnoses (85.7%) and individual mania criteria were also very high
(5). Furthermore, the WASH-U-KSADS has been validated in comparison with parent and teacher reports
(6). Subjects needed to have a Children’s Global Assessment Scale
(7) score of ≤60 to ensure moderate or severe impairment. Naturalistic treatment data were collected with the Longitudinal Interval Followup Evaluation
(8), and puberty was determined with the Duke scale
(9). “Mixed mania” was identified on the basis of overlapping time periods for the WASH-U-KSADS items on mania/hypomania and major depressive disorder. Rapid cycling was defined as four episodes per year
(3,
4). Ultrarapid cycling was defined as five to 364 and ultradian as ≥365 episodes per year, respectively
(3,
4). In ultradian cycling, mania needed to occur for ≥4 hours per day
(3,
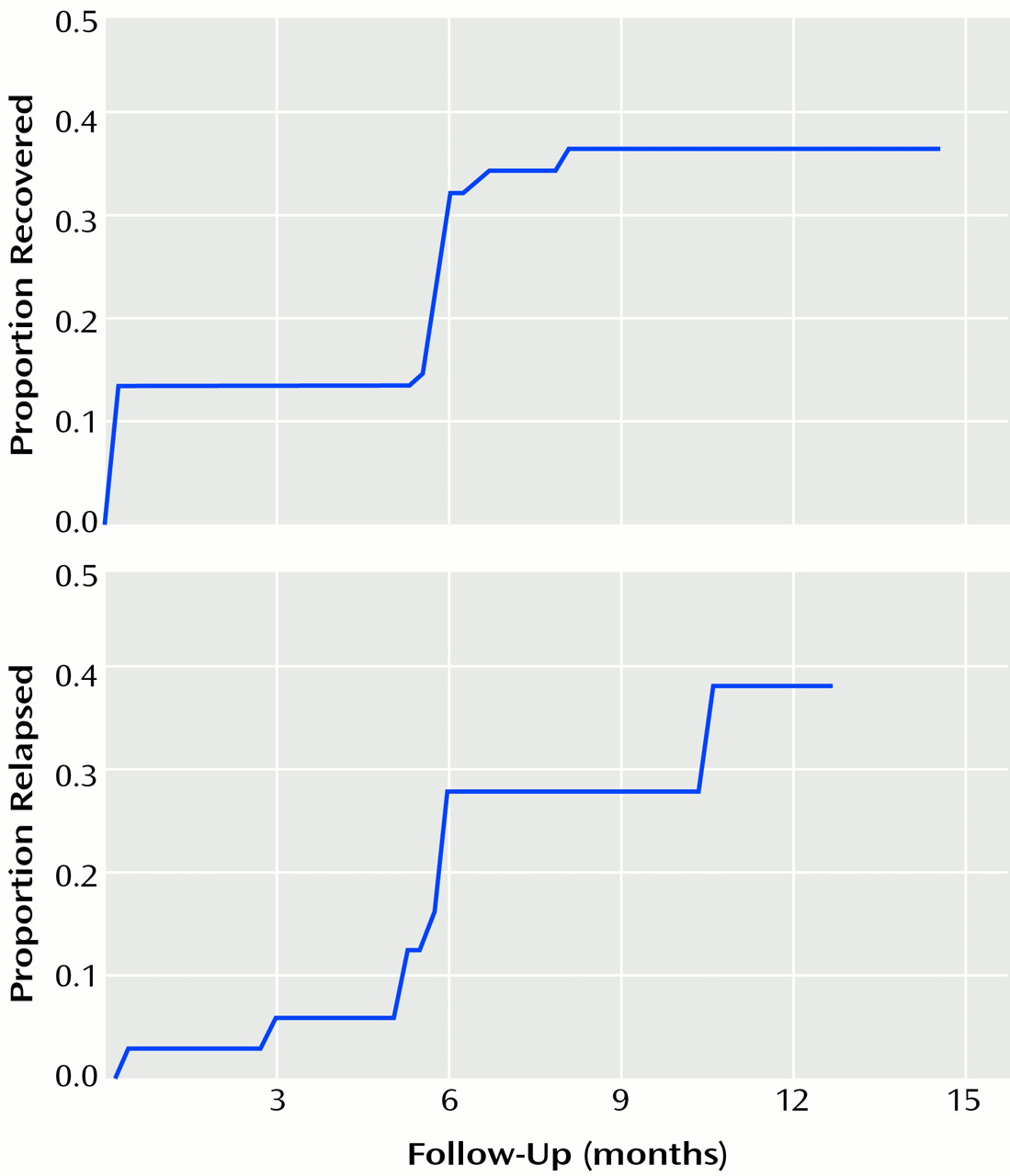
4). Recovery was defined as no syndromal DSM-IV mania or hypomania for ≥2 weeks, and relapse was defined as syndromal criteria for mania or hypomania and a Children’s Global Assessment Scale score of ≤60 for ≥2 weeks. After complete description of the study to parents and children, written informed consent was obtained from parents and written assent was obtained from children. Recovery and relapse were estimated with the Kaplan-Meier statistic. Cox modeling was used to test covariates, which included baseline age; gender; puberty status; presence of mixed mania, psychosis, ultradian rapid cycling, comorbid ADHD, comorbid oppositional defiant disorder, or comorbid conduct disorder; and use of antimanic medication. Antimanic medication was defined as neuroleptics, anticonvulsants, and lithium. Details of medication use were reported previously
(5).