Several hypotheses that have advanced a common etiopathological background for eating disorders have linked cultural, environmental, genetic, physiological, and psychological factors to risk for these disorders
(1). Genetic predisposing factors to anorexia nervosa and bulimia nervosa have been investigated separately in twin and familial studies. Twins studies have found concordance rates for anorexia nervosa of 48.5%–71.0% among monozygotic twins and 0%–10% among dizygotic twins
(2–
4). Concordance rates for bulimia range from 22.9%–83.0% for monozygotic twins and 0%–27.0% for dizygotic twins
(5–
7).
The high prevalence of depressive symptoms in patients with eating disorders has led many researchers to focus on risk for affective disorders in the families of those patients. However, interest in the relationship between eating disorders and anxiety disorders has increased
(20). In particular, researchers have hypothesized that eating disorders are part of the obsessive-compulsive spectrum of disorders, which includes obsessive-compulsive disorder (OCD) and tic disorders/Tourette’s syndrome. Several authors have suggested that anorexia nervosa could be considered a form of OCD
(21–
26). Lilenfeld et al.
(19) found an elevated risk for obsessive-compulsive personality disorder but not for OCD among the relatives of anorexia nervosa probands.
Results
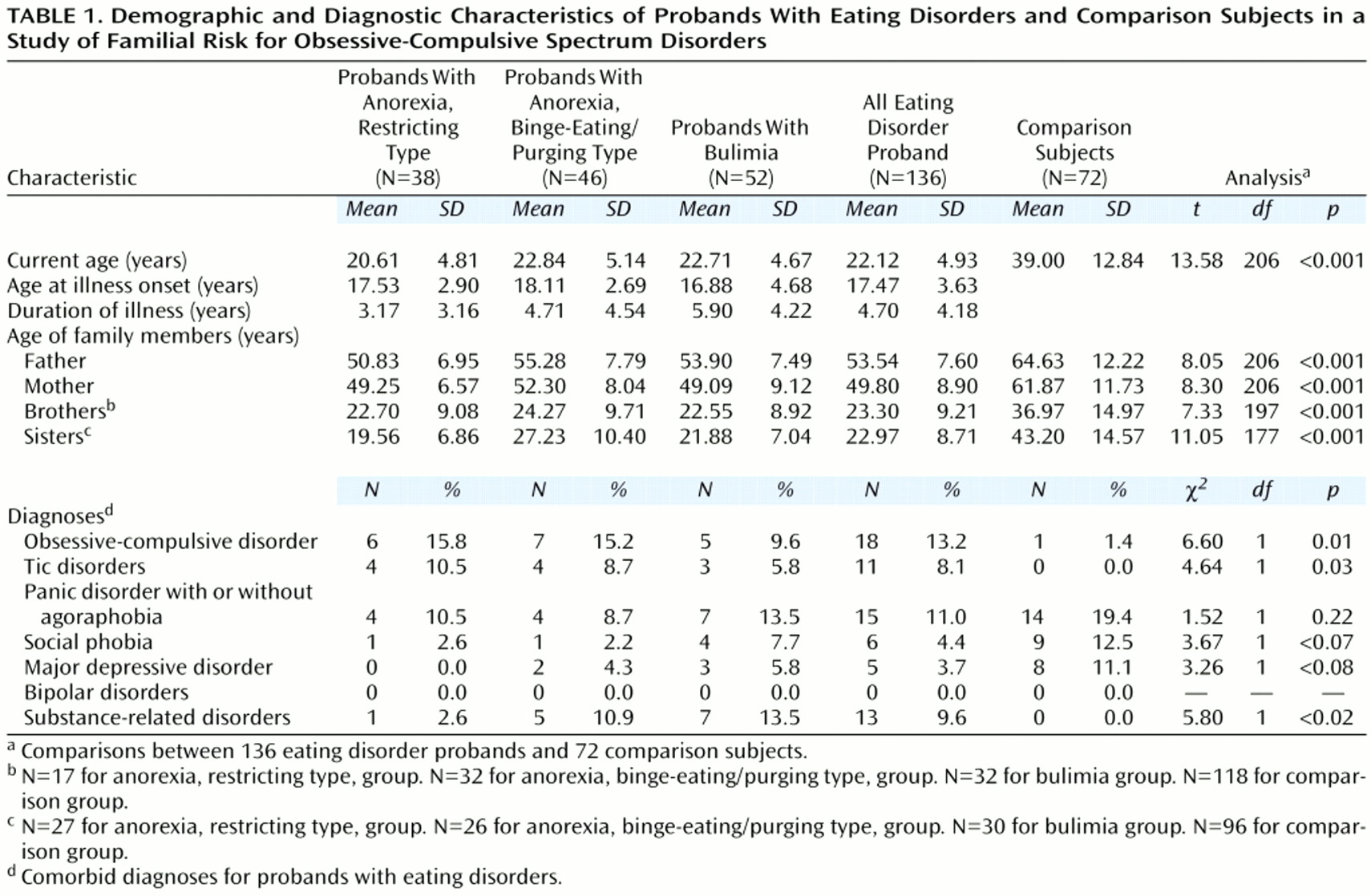
Current age and age at onset of eating disorder of the eating disorder probands did not differ significantly in the three eating disorder subgroups (
Table 1). The mean duration of illness was significantly different among the three groups (F=5.20, df=2, 135, p<0.007); the probands affected with anorexia, restricting type, had a markedly shorter duration of illness than did the probands with bulimia. This difference may have been related to the tendency of persons with the restricting type of anorexia to seek psychiatric consultation earlier, given the severity of their physical symptoms.
The eating disorder probands and the comparison subjects differed significantly in current age. The first-degree relatives of the eating disorder probands differed significantly in age from the first-degree relatives of the comparison subjects.
Analysis of the frequency of comorbid diagnoses showed that the eating disorder probands differed significantly from the comparison subjects in the proportion of subjects with a diagnosis of OCD, tic disorders, and substance-related disorders (
Table 1). No significant differences for other psychiatric diagnoses were observed.
The total study group included relatives who were directly interviewed and relatives who were not directly interviewed. The diagnoses of the relatives who were not interviewed were made on the basis of family history information. This procedure may have underestimated psychiatric morbidity. Nevertheless, the morbidity risk for obsessive-compulsive spectrum disorders and eating disorders for the interviewed relatives (9.01%) and for the relatives who were not interviewed (13.71%) was not significantly different (z test for differences between proportions=1.45, p=0.15); therefore, we grouped the interviewed relatives together with the relatives who were not interviewed in the analyses. We compared the overall group of eating disorder probands and their relatives with the comparison subjects and their relatives. We also compared each subgroup of eating disorder probands and their relatives with the comparison subjects and their relatives, introducing the Bonferroni correction for multiple testing for each set of comparisons (seven tests in each set) (significant p value=0.05/7, or p≤0.0071).
Eating Disorders
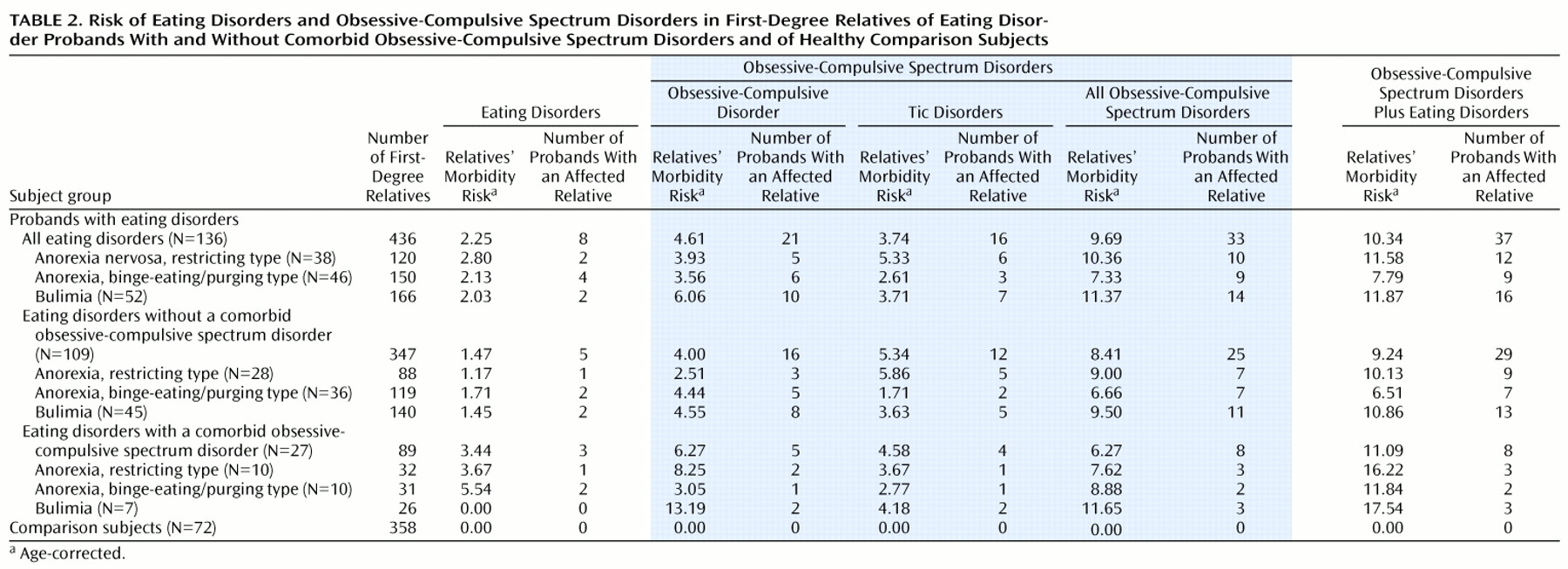
We determined the number of families in which an eating disorder occurred in a first-degree relative of the eating disorder proband or the comparison subject (
Table 2). The number of families with affected relatives was no greater in the eating disorder group than in the comparison group (χ
2=2.96, df=1, p=0.09). No differences between groups were observed in the number of families with affected parents (χ
2=0.43, df=1, p=0.51) or in the number of families with affected siblings (χ
2=1.37, df=1, p=0.24).
OCD
The morbidity risk for OCD in the first-degree relatives of the 136 eating disorder probands, corrected for age, was calculated (
Table 2).
A significant difference in the number of first-degree relatives with OCD was found between the overall group of families of eating disorder probands and the comparison families (χ2=12.37, df=2, p=0.002). There was no significant difference between groups in the number of parents with OCD (χ2=5.22, df=1, p=0.02). However, the siblings of probands with bulimia were significantly more likely to have a diagnosis of OCD than were the siblings of the comparison subjects (χ2=7.9, df=1, p=0.005).
The morbidity risk for OCD was analyzed separately in the families of eating disorder probands without and with a comorbid diagnosis of an obsessive-compulsive spectrum disorder (109 families and 27 families, respectively). The first-degree relatives in the families of the 109 probands without a comorbid obsessive-compulsive spectrum disorder were significantly more likely to have OCD than were the relatives of the comparison subjects (χ
2=9.84, df=1, p=0.002), but there was no significant difference in the number of relatives with OCD between the subgroup of 28 probands with anorexia, restricting type, and the comparison group (χ
2=4.70, df=1, p=0.03) (
Table 2). There were no significant differences between the families of the 109 probands and the comparison families in the number of parents with OCD (χ
2=5.35, df=1, p=0.02) or the number of siblings with OCD (χ
2=2.56, df=1, p=0.11).
The first-degree relatives in the families of the 27 eating disorder probands with a comorbid obsessive-compulsive spectrum disorder were significantly more likely to have OCD than were the relatives of the comparison subjects (χ
2=14.04, df=2, p<0.0001), but there was no significant difference in the number of relatives with OCD between the subgroup of 10 probands with anorexia, binge-eating/purging type, and the comparison group (χ
2=1.35, df=1, p=0.25) (
Table 2). The parents of the 27 eating disorder probands with a comorbid obsessive-compulsive spectrum disorder were more likely to have OCD than the parents of the comparison subjects (χ
2=10.45, df=1, p=0.001), even though the parents of the 10 probands with anorexia, binge-eating/purging type, were no more likely to have OCD than the parents of the comparison subjects (χ
2=1.35, df=1, p=0.25). The siblings in the 27 families of eating disorder probands with a comorbid obsessive-compulsive spectrum disorder were no more likely to have OCD than siblings in the comparison families (χ
2=0.26, df=1, p=0.61).
No intergroup differences were observed among the relatives of the various subgroups of eating disorder probands.
Tic Disorders
The first-degree relatives in the overall group of eating disorder probands were not significantly more likely to have a tic disorder than were the relatives of the comparison subjects (χ
2=9.18, df=2, p=0.01) (
Table 2). However, tic disorders were significantly more likely among the relatives of the probands with bulimia (χ
2=10.27, df=2, p=0.006) and among the relatives of the probands with anorexia, restricting type (χ
2=9.16, df=1, p=0.002), than among the relatives of the comparison subjects.
The first-degree relatives in the families of the 109 eating disorder probands without a comorbid obsessive-compulsive spectrum disorder were no more likely to have a tic disorder than were the relatives of the comparison subjects (χ2=6.80, df=1, p=0.009). However, tic disorders were significantly more likely in the families of the probands with anorexia, restricting type, without a comorbid obsessive-compulsive spectrum disorder than in the comparison families (χ2=10.04, df=1, p=0.002).
The siblings of the 27 eating disorder probands with a comorbid obsessive-compulsive spectrum disorder were more likely to have tic disorders than were the siblings of the comparison subjects (χ2=11.12, df=1, p<0.001). Tic disorders were more likely among the relatives of the probands with bulimia in these 27 families than among the relatives of the comparison subjects (χ2=7.62, df=1, p=0.006).
No intergroup differences were observed among the relatives of the various subgroups of eating disorder probands.
Obsessive-Compulsive Spectrum Disorders
The families of the eating disorder probands were significantly more likely to include first-degree relatives affected with obsessive-compulsive spectrum disorders than were the families of the comparison subjects (χ
2=20.77, df=2, p<0.001) (
Table 2). The parents of the eating disorder probands were significantly more likely have obsessive-compulsive spectrum disorders than the parents of the comparison subjects (χ
2=10.72, df=1, p=0.001). The families of the eating disorder probands were more likely to include affected siblings than were the comparison families (χ
2=8.21, df=1, p=0.004); this difference was due to the significantly higher number of affected siblings in the families of the probands with bulimia than in the comparison families (χ
2=10.99, df=1, p
<0.001) and the higher number of affected siblings in the families of the probands with anorexia, restricting type, than in the comparison families (χ
2=7.12, df=1, p=0.008).
The families of the 109 eating disorder probands without a comorbid obsessive-compulsive spectrum disorder included significantly more first-degree relatives who were affected with these disorders than did the comparison families (χ2=19.16, df=2, p<0.001). The parents of the eating disorder probands were more likely to be affected than the parents of the comparison subjects (χ2=9.07, df=1, p=0.003); this difference was due to the higher number of affected parents in the families of the probands with bulimia and with anorexia, restricting type, than in the comparison families (χ2=9.31, df=1, p=0.002 and χ2=7.31, df=1, p=0.007, respectively). The siblings of the probands with bulimia and with anorexia, restricting type, were more likely to be affected than the siblings of the comparison subjects (χ2=7.56, df=1, p=0.006 and χ2=7.32, df=1, p=0.007, respectively).
The first-degree relatives in the subset of the 27 families of the eating disorder probands with a comorbid obsessive-compulsive spectrum disorder were more likely to have an obsessive-compulsive spectrum disorder than the relatives of the comparison subjects (χ2=23.21, df=2, p<0.001). Only the fathers of the probands with anorexia, binge-eating/purging type, were no more likely to be affected than the fathers of the comparison subjects (χ2=1.19, df=1, p=0.28). The siblings of the probands with bulimia were significantly more likely to be affected than the siblings of the comparison subjects (χ2=21.42, df=1, p<0.001).
No intergroup differences were observed among the relatives of the various subgroups of eating disorder probands.
Eating Disorders Plus Obsessive-Compulsive Spectrum Disorders
The rates of both eating disorders and obsessive-compulsive spectrum disorders were significantly higher in the first-degree relatives of the eating disorder probands than in the relatives of the comparison subjects (10.34% versus 0%) (χ2=23.83, df=2, p<0.001). The rates were higher in the relatives of the probands with anorexia, restricting type (11.3%) (χ2=25.52, df=2, p<0.001), the relatives of the probands with anorexia, binge-eating/purging type (8.1%) (χ2=15.25, df=2, p<0.001), and the relatives of the probands with bulimia (12.9%) (χ2=25.44, df=2, p<0.001), compared separately with the rate in the relatives of the comparison subjects.
No significant intergroup differences in the rate of eating disorders plus obsessive-compulsive spectrum disorders were found in the relatives of the eating disorders subgroups.
The parents and the siblings of the eating disorder probands had a significantly higher morbidity risk for these disorders than did the parents and siblings of the comparison subjects (χ2=13.03, df=2, p=0.001 and χ2=11.72, df=2, p=0.003, respectively). Only the siblings of the probands with anorexia, binge-eating/purging type, had a morbidity risk that did not differ significantly from that of the siblings of the comparison subjects (χ2=6.48, df=2, p<0.04).
The first-degree relatives of the 109 eating disorder probands without a comorbid obsessive-compulsive spectrum disorder had a significantly higher rate of both eating disorders and obsessive-compulsive spectrum disorders than the relatives of the comparison subjects (χ2=22.81, df=2, p<0.001), and the affected relatives in this subgroup accounted for most of the affected relatives in the overall group of families of the eating disorder probands. The parents of this subgroup of 109 probands were significantly more likely to have an eating disorder or an obsessive-compulsive spectrum disorder than the parents of the comparison subjects (χ2=12.39, df=2, p=0.002), and the siblings in this group were significantly more likely to be affected than the siblings of the comparison subjects (χ2=10.02, df=2, p=0.007), although the siblings of probands with anorexia, binge-eating/purging type, did not differ from the siblings of the comparison subjects in their rate of these disorders (χ2=4.08, df=3, p=0.13).
The rate of eating disorders or obsessive-compulsive spectrum disorders was higher in the families of the 27 eating disorder probands with a comorbid obsessive-compulsive spectrum disorder and in each of the eating disorder subgroups than in the comparison families (χ2=23.21, df=3, p<0.001). The parents of these 27 eating disorder probands were more likely to be affected with these disorders than the parents of the comparison subjects (χ2=14.04, df=2, p<0.001). Their siblings were more likely to be affected than the siblings of the comparison subjects (χ2=14.04, df=2, p<0.001); most of this difference was accounted for by the higher rate in the siblings of the probands with bulimia than in the siblings of the comparison subjects (χ2=21.42, df=1, p<0.001).
Discussion
This study examined the occurrence of obsessive-compulsive spectrum disorders among first-degree relatives in 136 nuclear families of eating disorder probands in Italy. The DSM-IV distinction between the restricting and the binge-eating types of anorexia nervosa was used, despite our awareness that many patients diagnosed with restricting-type anorexia may later develop binge-eating/purging type anorexia or bulimia
(42). The rate of crossover from anorexia to bulimia is reported to range from 10% to 50%.
The higher morbidity risk for obsessive-compulsive spectrum disorders in the first-degree relatives of the patients with eating disorders (10.34%) lends further support to the proposal that obsessive and compulsive symptoms in eating disorder patients should not be considered signs of an additional diagnosis, but rather part of the eating disorder, and that obsessive-compulsive disorder and eating disorders are phenotypic expressions of the same liability.
Eating disorder patients without a comorbid obsessive-compulsive spectrum disorder might develop such a disorder later; although we found no difference in age between the eating disorder probands with and without a comorbid obsessive-compulsive spectrum disorder, even though those with a comorbid diagnosis were slightly older (by 2 years).
The comorbidity of obsessive-compulsive spectrum disorders in eating disorder probands did not influence familial liability for obsessive-compulsive spectrum disorders, despite the significantly greater familial risk for these disorders among the parents of probands with bulimia and anorexia, restricting type, than in the parents of the 109 eating disorder probands without comorbid obsessive-compulsive spectrum disorders. No differences in morbidity risk were found for first-degree relatives of eating disorder probands with and without a comorbid obsessive-compulsive spectrum disorder (data not shown). Unlike our results, the findings of Lilenfeld et al.
(19) showed that stratification by proband comorbidity status influenced the adjusted risk ratios for OCD in first-degree relatives. However, even after Lilenfeld et al. adjusted the risk ratios for OCD for the sex, age, and interview status of the relatives in their study, relatives of patients with anorexia nervosa and bulimia had a significantly higher risk for OCD than did the relatives of the comparison subjects. Our finding of an absence of difference in familial risk for eating disorders between the eating disorders group and the comparison group is similar to the finding of Lilenfeld et al.
(19) of no increased risk for anorexia nervosa and bulimia in the relatives of patients with eating disorders. From this we can conclude that when eating disorders are considered independently of obsessive-compulsive spectrum disorders, no evidence of a familial risk for eating disorders is found.
Although prevalence studies performed to date have considered anorexia and bulimia as two distinct categories, we found no differences in the morbidity risk for obsessive-compulsive spectrum disorders in comparisons of the eating disorders subgroups, suggesting that relatives of patients with anorexia and those of patients with bulimia share the same liability for obsessive-compulsive spectrum disorders.
Nevertheless, we observed a tendency toward higher morbidity risk for OCD and related disorders in some relatives: sisters of patients with bulimia (morbidity risk=12.13%), sisters of patients with anorexia, binge-eating/purging type (morbidity risk=13.35%), brothers of patients with bulimia (morbidity risk=18.23%), and brothers of patients with anorexia, restricting type (morbidity risk=27.36%). In general, the sisters of the eating disorder probands had a higher morbidity risk for obsessive-compulsive spectrum disorders, whereas the morbidity risk observed in their mothers was comparable to that of their fathers. We observed a higher occurrence of tic disorders in male relatives (fathers and brothers), in accordance with earlier findings that female relatives of OCD probands are affected with OCD and male relatives with tic disorders
(43,
44). However, OCD was not associated with a particular subtype of eating disorder in our study, and the overlap in morbidity risk for OCD among eating disorder subgroups provided indirect proof of a link between these disorders.
The main limitation of this study derives from the methods used to collect some clinical information from first-degree relatives. The family history method we used could have influenced the estimated true prevalence of eating disorders and OCD in first-degree relatives. Another problem was the choice of the techniques used to analyze nonindependent data.
The increased familial risk for obsessive-compulsive spectrum disorders in the families of the eating disorder probands suggests the need to further test the hypothesis of a genetic component for this risk. To better define the features of this liability, we have planned a segregation analysis of these family data that will consider eating disorders and OCD as a common phenotype (manuscript in preparation). These findings could enable us to define more accurately the relationship between the psychopathological aspects of eating disorder and OCD diagnoses, to better describe the common structure shared by the two disorders, and to improve treatment for eating disorders and OCD.