Structural brain abnormalities, including ventricular enlargement and decrements in gray matter volume
(1,
2), play an important role in the pathology of schizophrenia. Smaller volumes of gray matter occur in the neocortex as well as in subcortical structures, such as the thalamus
(3), amygdala, and hippocampus
(1,
2).
If the structural brain abnormalities of schizophrenia were related to the illness process, one would expect schizophrenic patients with a poor outcome to display more extensive brain abnormalities than schizophrenic patients with a relatively good outcome. To test this hypothesis, intracranial volume and volumes of the cerebrum, gray and white matter, thalamus, frontal lobes, lateral and third ventricles, and cerebellum were compared in patients with schizophrenia at the extremes of the outcome spectrum and healthy comparison subjects.
Method
Twenty patients with a poor outcome, 25 patients with a good outcome, and 23 healthy comparison subjects participated after written informed consent was obtained. A diagnosis of DSM-IV schizophrenia was established by means of the Comprehensive Assessment of Symptoms and History
(4). Subjects with a major medical or neurological illness, an IQ below 80, a history of having received ECT, or a history of substance dependence were excluded.
Poor-outcome patients had been hospitalized for more than 50% of their total duration of illness and had been continuously hospitalized over the past 3 years. Good-outcome patients had been hospitalized for less than 10% of their total duration of illness and were not hospitalized during the past year. All patients needed to have a minimum duration of illness of 15 years to ensure a reliable outcome measure
(5).
The three groups did not differ significantly in age, gender, or handedness. The two patient groups did not differ significantly in doses of antipsychotic medication. Symptom profile, level of functioning, and cognitive functioning were evaluated by means of the Positive and Negative Syndrome Scale
(6), the Disability Assessment Schedule
(7), the Global Assessment Scale
(8), and the Mini-Mental State Examination
(9).
With a Philips (Eindhoven, the Netherlands) 1.5 T scanner, T
1-weighted scans with 1.2-mm contiguous coronal slices and dual contrast turbo spin echo scans with 1.6-mm-thick contiguous coronal slices of the whole head were acquired. Intracranial matter, cerebral gray and white matter (whole brain, excluding the cerebellum and brainstem), frontal lobes
(10), lateral and third ventricles, cortical CSF, and cerebellum volumes were measured automatically
(11), whereas the thalamus was measured manually
(12).
The interrater reliability determined by the intraclass correlation coefficient (ICC) of the intracranial volume was 0.99; for the cerebrum, ICC=0.99; for the cerebellum, ICC=0.95; for the lateral ventricles, ICC=0.99; for the third ventricle, ICC=0.95; for the left thalamus, ICC=0.78; and for the right thalamus, ICC=0.74.
Volumetric differences between the three groups were analyzed for each structure with repeated measures analysis of covariance (ANCOVA) by using a group-by-side (left and right) and, if applicable, side-by-matter (gray and white) design with intracranial volume as the covariant. Post hoc two-tailed t tests were used to evaluate which group contributed most to the significant effects of the ANCOVAs.
Results
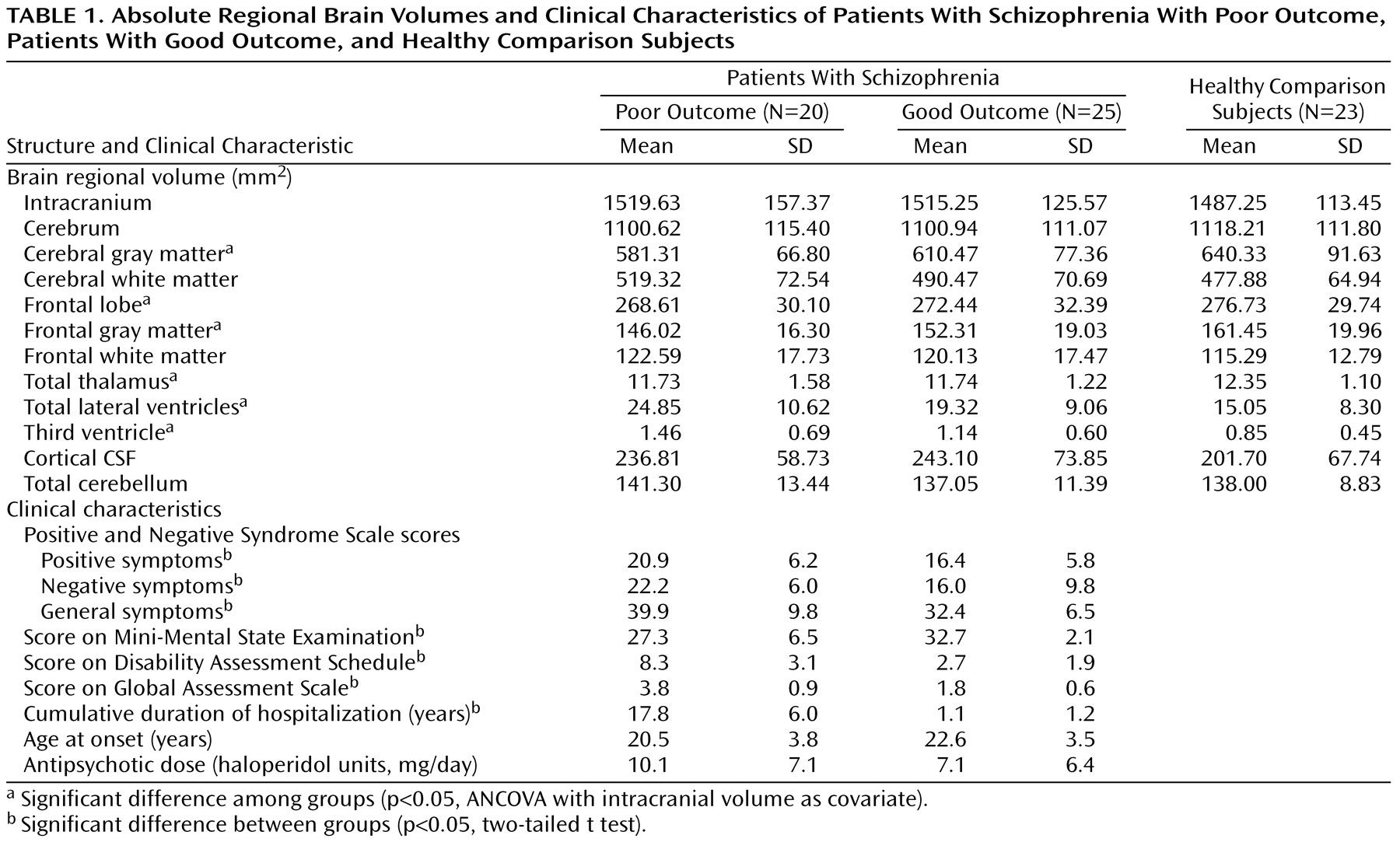
Clinical characteristics are listed in
Table 1. Poor-outcome patients displayed significantly more positive, negative, and general symptoms and were more severely impaired in cognitive and social functioning than good-outcome patients. Eleven of the poor-outcome patients were taking typical antipsychotics, and nine were taking atypicals. Nineteen of the good-outcome patients were receiving typical antipsychotics, and six were receiving atypicals. Regional brain volumes are also listed in
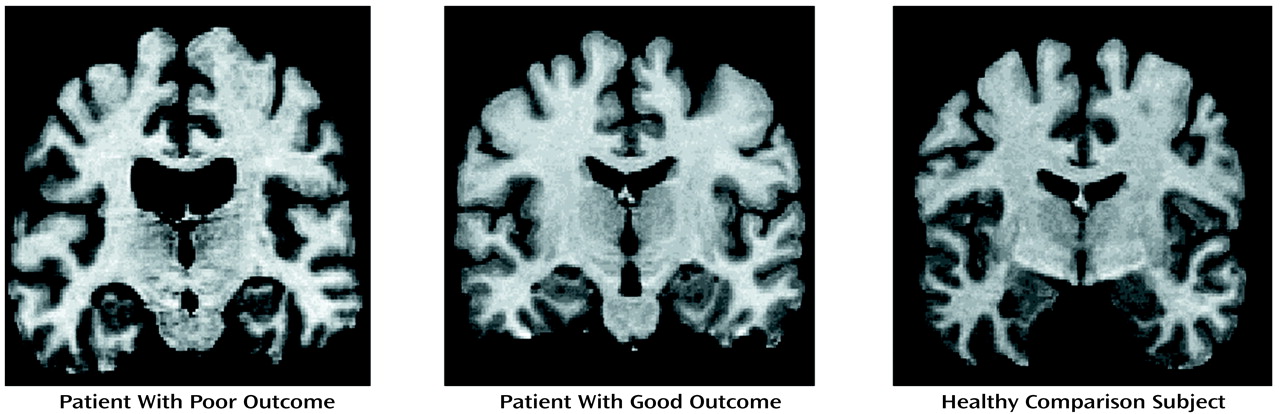
Table 1 and
Figure 1. No significant main effects or interactions were found among intracranial, cortical CSF, or cerebellar volumes. No significant interactions between group and side were found for any of the volume measures.
A significant interaction of group and matter (F=6.3, df=2, 64, p<0.01) was found, which could mainly be attributed to a significantly smaller gray matter volume in poor-outcome patients than in healthy comparison subjects (t=2.4, df=41, p<0.02), whereas the gray matter volume of the good-outcome patients did not significantly differ from those of the other two groups.
A significant main effect of group (F=3.3, df=2, 64, p<0.05) was found for frontal lobe volume (
Figure 1), which could mainly be attributed to a significantly smaller frontal lobe volume in the poor-outcome patients than in the healthy comparison subjects (t=2.5, df=41, p<0.02), whereas the frontal lobe volume of the good-outcome patients did not significantly differ from those of the other two groups.
A significant interaction of group and frontal lobe matter was found (F=10.9, df=2, 64, p<0.01), which was mainly caused by a difference between poor-outcome patients and healthy comparison subjects in the volumes of frontal lobe gray matter (t=2.8, df=41, p<0.01), whereas the volumes of frontal lobe gray matter did not differ from that of good-outcome patients and those of the other two groups.
A significant main effect of group was found for lateral ventricle volume (F=5.5, df=2, 64, p<0.01), which could mainly be attributed to a larger lateral ventricle volume in poor-outcome patients than in healthy comparison subjects (t=3.4, df=41, p<0.01), whereas the lateral ventricle volume of good-outcome patients did not significantly differ from those of the other two groups.
A significant main effect of group was found for third ventricle volume (F=5.4, df=2, 64, p<0.01), which could mainly be attributed to a significantly larger third ventricle volume in poor-outcome patients than in healthy comparison subjects (t=3.5, df=41, p<0.01), whereas third ventricle volume in good-outcome patients did not significantly differ from those of the other two groups.
A significant main effect for group was found for thalamic volume (F=3.5, df=2, 64, p<0.05), which could be attributed to smaller thalamic volumes both in poor-outcome patients as well as in good-outcome patients than in healthy comparison subjects (t=2.3, df=41, p<0.03, and t=2.3, df=46, p<0.03, respectively), whereas thalamic volumes did not significantly differ between poor- and good-outcome patients.
Discussion
In this study the relationship between outcome and structural brain abnormalities in schizophrenia was investigated by comparing patients with schizophrenia at the extremes of the outcome spectrum with healthy comparison subjects.
Thalamic volumes were smaller in the patients with schizophrenia, irrespective of their outcome. In contrast, the poor-outcome patients displayed much smaller gray matter volumes of the cerebrum (particularly in the frontal lobes) and larger lateral and third ventricles than patients who had a favorable course of illness.
These results suggest that the smaller thalamic volumes found in the patients with schizophrenia than in the healthy comparison subjects may reflect a greater susceptibility for the disorder that is unrelated to outcome, whereas the smaller gray matter volumes in the cerebrum, particularly in the frontal lobes, and the larger lateral and third ventricles appear related to poor outcome in schizophrenia.
Recently, we reported that patients with schizophrenia, but not their healthy siblings, displayed smaller volumes of the frontal lobe gray matter
(11), which suggests that in contrast to smaller thalamic volumes, the smaller volumes of the prefrontal gray matter may require additional risk factors that occur exclusively in patients with schizophrenia. Poor-outcome patients may possibly have a greater number of such risk factors than good-outcome patients. These factors may include environmental risk factors, such as malnutrition during pregnancy
(13), obstetric complications at the time of birth
(14), or genetic risk factors, such as a larger number of genes carrying risk or genes with a stronger effect on the disease
(15).