Gender Differences
In initial analyses for midfrontal sites F3 and F4, we found main effects for gender (F=12.70, df=1, 106, p<0.001, η
2=0.11) and hemisphere (F=4.90, df=1, 106, p<0.03, η
2=0.04). In addition, we observed a group-by-gender-by-hemisphere interaction (F=5.47, df=1, 106, p<0.02, η
2=0.05).
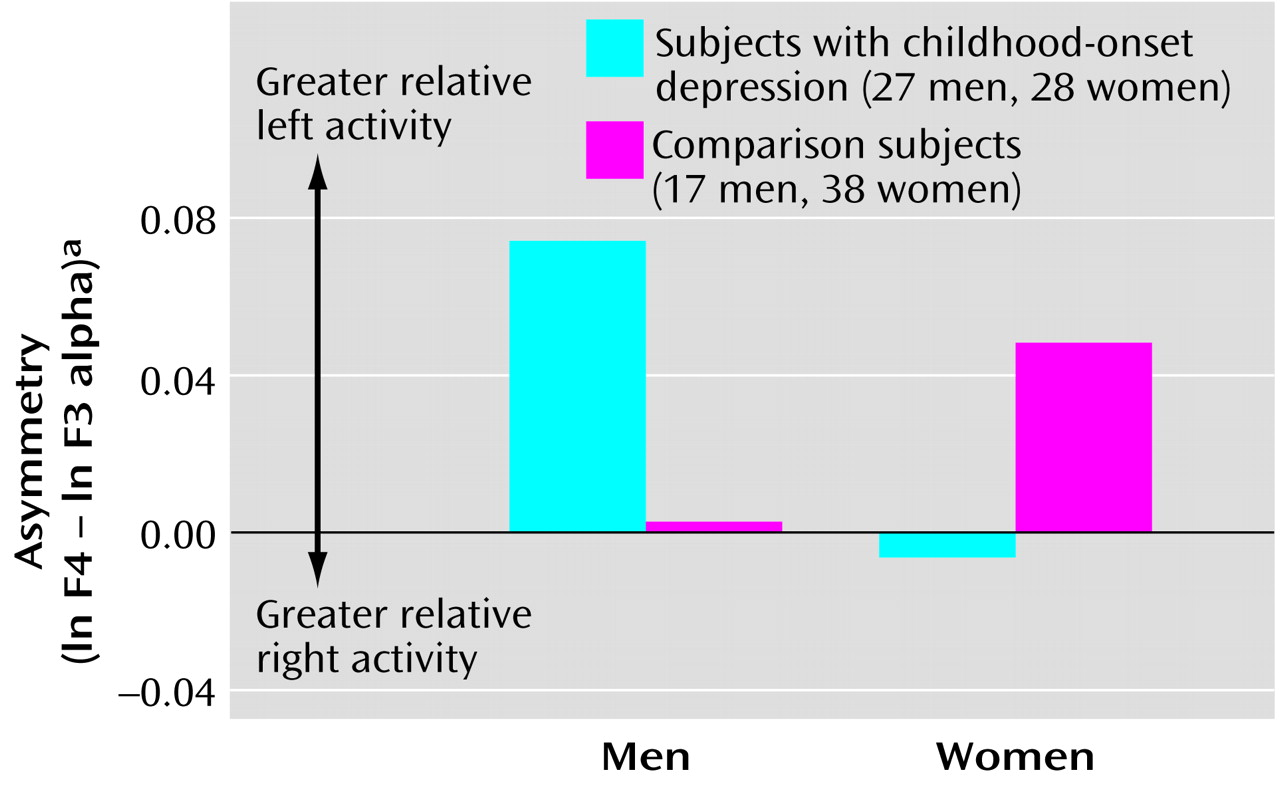
Figure 1 illustrates the mean values for midfrontal asymmetry for men and women in each group. Higher scores reflect greater relative left midfrontal alpha suppression. The figure shows that women with childhood depression had greater relative right midfrontal alpha suppression, whereas men with childhood depression had greater relative left midfrontal alpha suppression. The magnitude of asymmetry was greater for men than for women. Contrast analyses of data for subjects with childhood depression revealed that midfrontal asymmetry differed between men and women (t=2.00, df=53, p<0.05, η
2=0.07). Gender differences depended on both left midfrontal (F3) alpha power (t=–2.50, df=108, p<0.01, η
2=0.06) and right midfrontal (F4) alpha power (t=–2.64, df=108, p<0.009, η
2=0.06). Men had lower power than women at all sites.
Clinical History
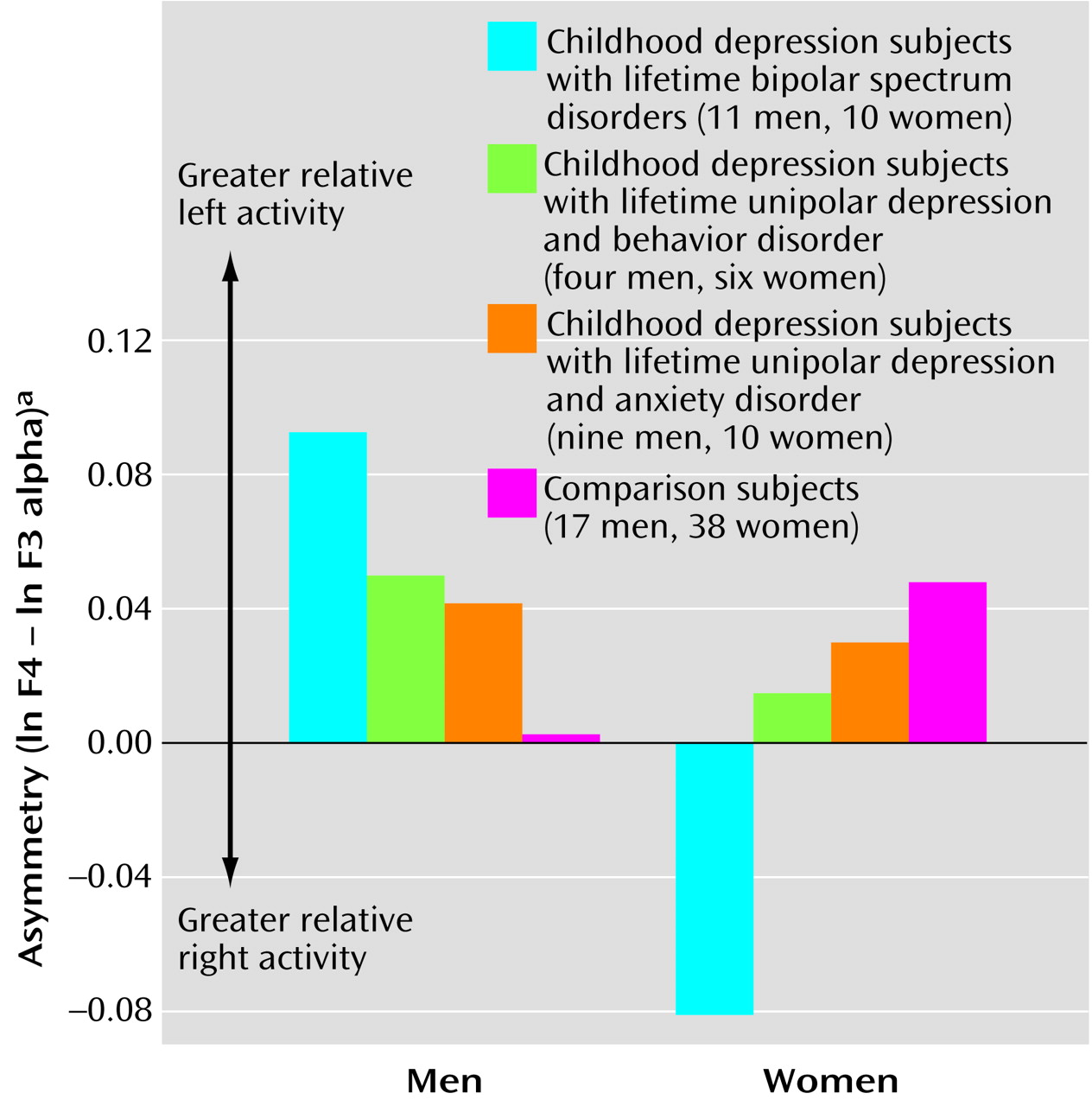
Participants were hierarchically sorted on the basis of whether they had a history of 1) lifetime bipolar spectrum disorder (N=21), 2) unipolar depression with early-onset behavior disorders (N=10), or 3) unipolar depression with early-onset anxiety disorders (N=19). The five participants who did not meet criteria for these categories were not included in these analyses.
Specifically at midfrontal sites, we observed a diagnostic group-by-gender-by-hemisphere interaction (F=3.38, df=3, 97, p<0.02, η
2=0.10) (
Figure 2). Among probands with bipolar spectrum disorder, men and women had particularly extreme relative left and relative right midfrontal asymmetry, respectively. Contrast effects showed that midfrontal asymmetry for the bipolar disorder group differed from that for other groups (t=–2.76, df=103, p<0.007, η
2=0.07). In addition, there was an interaction with gender (t=3.17, df=103, p<0.002, η
2=0.09). When men and women were considered separately, differences between the bipolar disorder and comparison groups remained for both men (t=2.13, df=26, p<0.04, η
2=0.15) and women (t=–2.95, df=46, p<0.005, η
2=0.16).
Current Depressive Symptoms
The childhood depression proband group, relative to the comparison group, had a higher mean current Beck Depression Inventory score (childhood depression group: mean=9.1, SD=7.6; comparison group: mean=2.5, SD=2.3) (F=35.05, df=1, 106, p<0.0001, η2=0.25). When the data were viewed categorically, 19 of the 55 childhood depression probands had a high level of depressive symptoms (i.e., Beck Depression Inventory score ≥10). This group included both probands with a history of unipolar depression and those with a history of bipolar disorder and probands who were and were not taking psychotropic medication (nonsignificant chi-square for group membership). Probands who were taking psychotropic medication (N=9) and those who were not (N=46) did not differ in self-reported level of depressive symptoms (F=0.47, df=1, 53, p=0.49, η2=0.009) or in midfrontal EEG asymmetry (F=0.33, df=1, 53, p=0.56, η2=0.006).
Men and women with childhood depression did not differ significantly in self-reported severity of depression, as measured with the Beck Depression Inventory (men: mean=8.6, SD=6.6; women: mean=9.5, SD=8.5) (F=0.18, df=1, 53, p=0.67, η2=0.003) or in the proportion of symptomatic subjects (eight men and 11 women) (F=0.55, df=1, 53, p=0.46, η2=0.01). Among the comparison subjects, there also were no gender differences in severity of depressive symptoms (F=0.58, df=1, 53, p=0.45, η2=0.01). Yet, despite comparable self-reported depressive symptoms in men and women, gender differences in midfrontal asymmetry were more extreme in the symptomatic than in the nonsymptomatic probands.
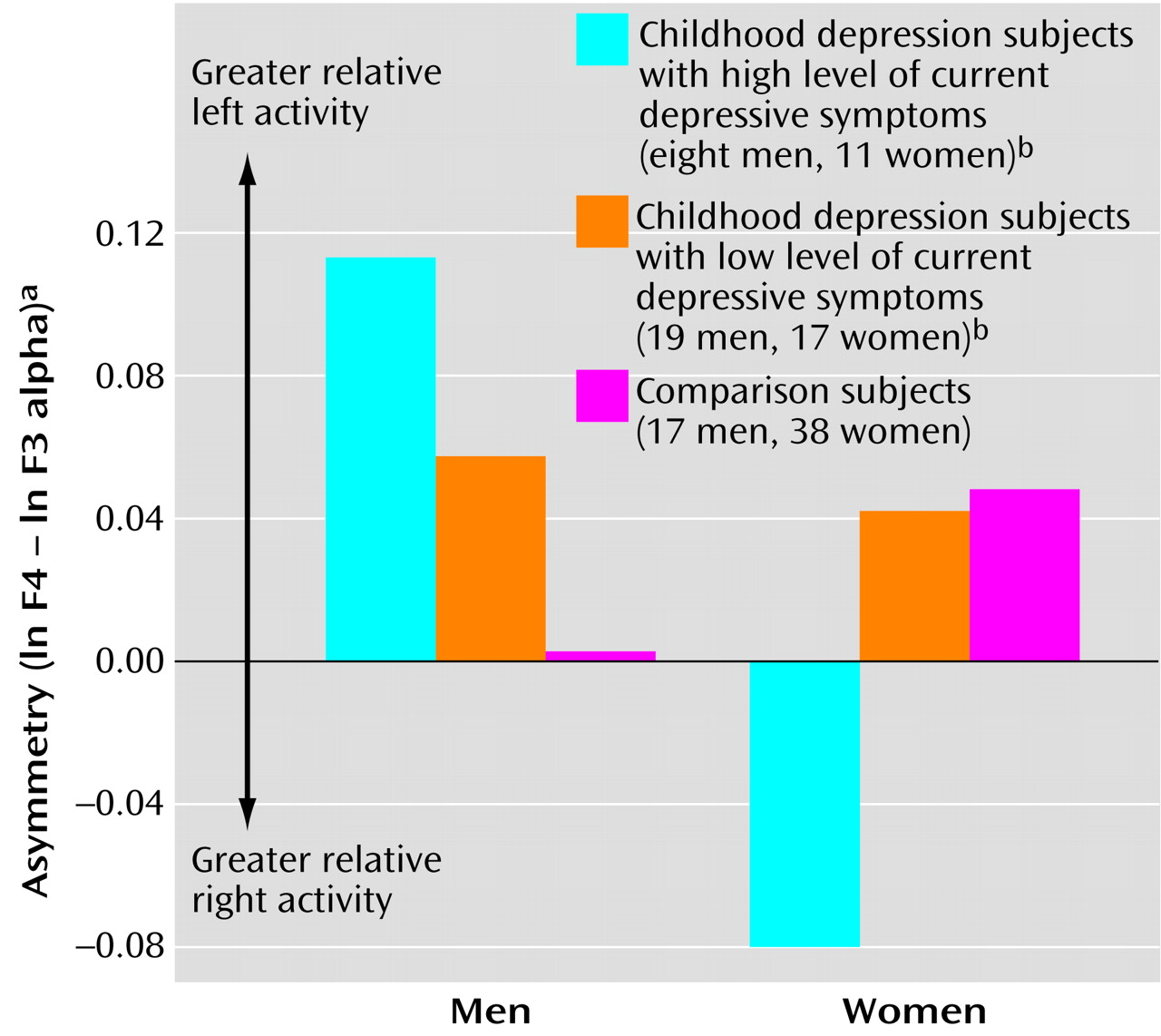
In particular, we found a depressive symptom group-by-gender-by-hemisphere interaction at midfrontal sites (F=5.46, df=2, 104, p<0.006, η
2=0.10). As illustrated in
Figure 3, symptomatic men with a history of childhood depression had greater relative left midfrontal asymmetry (t=1.99, df=42, p<0.05, η
2=0.09), and symptomatic women with childhood depression had greater relative right midfrontal asymmetry (t=–2.81, df=64, p<0.007, η
2=0.11). Within the childhood depression group, midfrontal asymmetry in symptomatic women tended to differ from that in nonsymptomatic women (t=2.17, df=26, p<0.04, η
2=0.15), but symptomatic and nonsymptomatic men did not differ from each other in this feature (t=–0.91, df=25, p=0.4, η
2=0.03).
We also examined the effects of current levels of anxiety as measured by the Beck Anxiety Inventory. The childhood depression proband group, relative to the comparison group, reported higher levels of anxiety (childhood depression group: mean=7.8, SD=7.3; comparison group: mean=3.3, SD=3.0) (F=16.85, df=1, 106, p<0.0001, η2=0.14). When viewed categorically, 21 of the clinical probands had elevated anxiety symptoms (i.e., Beck Anxiety Inventory score ≥8). No gender differences were present in the childhood depression group (t=–1.20, df=53, p=0.23, η2=0.03) or the comparison group (t=0.005, df=53, p=0.99, η2=0.0001).
Midfrontal and parietal asymmetries were comparable for participants with and without anxiety symptoms. However, currently anxious childhood depression probands, but not the probands without current anxiety symptoms, differed from comparison subjects in their midfrontal-central (FC1, FC2) asymmetry (F=4.96, df=2, 104, p<0.009, η2=0.09). Among the childhood depression probands with elevated anxiety, both men (N=8) and women (N=13) had relative right midfrontal-central asymmetry (ln FC2 – ln FC1=–0.0554 for men and –0.0814 for women). In addition, for occipital (O1, O2) asymmetry, we observed an interaction of current anxiety symptom group and gender (F=4.68, df=2, 104, p<0.01, η2=0.08). In contrast to the findings for frontal asymmetry, particularly extreme relative left occipital asymmetry was found in anxious women (ln O2 – ln O1=0.3057) and relative right occipital asymmetry was found in anxious men (ln O2 – ln O1=–0.0333).