The severity of multiple idiopathic physical symptoms occurs along a continuum
(5), and only 0.1%–0.2% of adults in the United States have enough symptoms to satisfy diagnostic criteria for the most severe form of multiple idiopathic physical symptoms, somatization disorder
(6). A much larger proportion of individuals in the general population report multiple idiopathic physical symptoms, however, and Escobar and colleagues
(7) developed criteria for a less severe (“abridged”) syndrome characterized by four or more idiopathic symptoms for men and six or more for women, also known as the somatic symptom index 4/6 (SSI-4/6). Escobar et al.
(4,
6) found that the SSI-4/6 criteria were met by 4.4% of U.S. adults studied. Since then, a myriad of low-threshold syndromes involving multiple idiopathic physical symptoms have been studied, and some have been used clinically. These include undifferentiated somatoform disorder (DSM-III-R), multisomatoform disorder
(8), an index using three symptoms for men and five for women (SSI-3/5)
(9), and chronic multisymptom illness
(10). In a large multiethnic general population sample
(4,
6,
7), the SSI-4/6 was associated with a higher prevalence of psychiatric disorders, especially mood and anxiety disorders, greater use of medical services, and higher levels of unemployment and days in bed, effects that persisted even after the influences of demographic factors and health status were controlled for. Rief and colleagues
(9) compared several sets of criteria for multisymptom syndromes, including the DSM-III-R and DSM-IV somatization disorder criteria, the SSI-3/5, and the SSI-4/6, in patients referred for behavioral treatment. Rief et al. found a high degree of concordance across subthreshold definitions based on multiple symptoms. Escobar and colleagues
(11) briefly reviewed the research findings from various studies using the SSI-4/6. They noted that the SSI-4/6 has shown robust associations, suggesting construct validity, in diverse study groups, such as primary care patients, Puerto Ricans, disaster victims, U.S. women in the community, and patients seen in medical specialty clinics for one of a wide range of “single-symptom syndromes,” such as tinnitus, chronic pelvic pain, and persistent dizziness.
We wanted to learn more about the natural history of multiple idiopathic physical symptoms, particularly their relationship to mortality, using data from the National Institute of Mental Health (NIMH) Epidemiological Catchment Area (ECA) study. An important methodological issue when determining the relationship between a health condition and a longitudinal outcome is the need to consider how the baseline condition changes over time. An outcome such as mortality reflects only one potential consequence of multiple idiopathic physical symptoms, and it is important to correct mortality figures for the occurrence of “competing” consequences
(12,
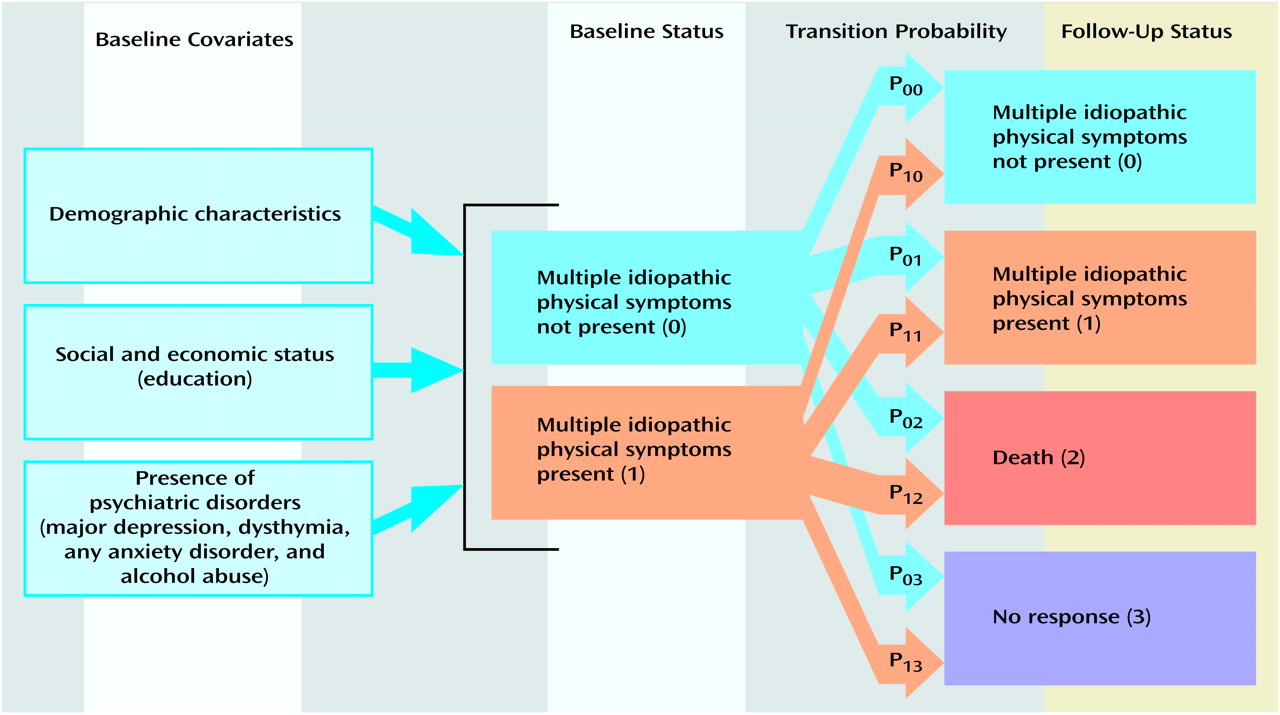
13). For example, by considering survey nonresponse, the incidence of multiple idiopathic physical symptoms, and the resolution of multiple idiopathic physical symptoms as competing outcomes, one can better understand the potential impact of these factors on estimates of mortality related to multiple idiopathic physical symptoms. Therefore, in the present research we used a multivariate competing-risks model to investigate the natural history of multiple idiopathic physical symptoms and the possible linkage between such symptoms and mortality among U.S. adults.
Results
The bivariate association between baseline status regarding multiple idiopathic physical symptoms and mortality was statistically significant (full sample: χ
2=6.32, df=1, p=0.02; sample excluding nonrespondents: χ
2=5.60, df=1, p=0.02).
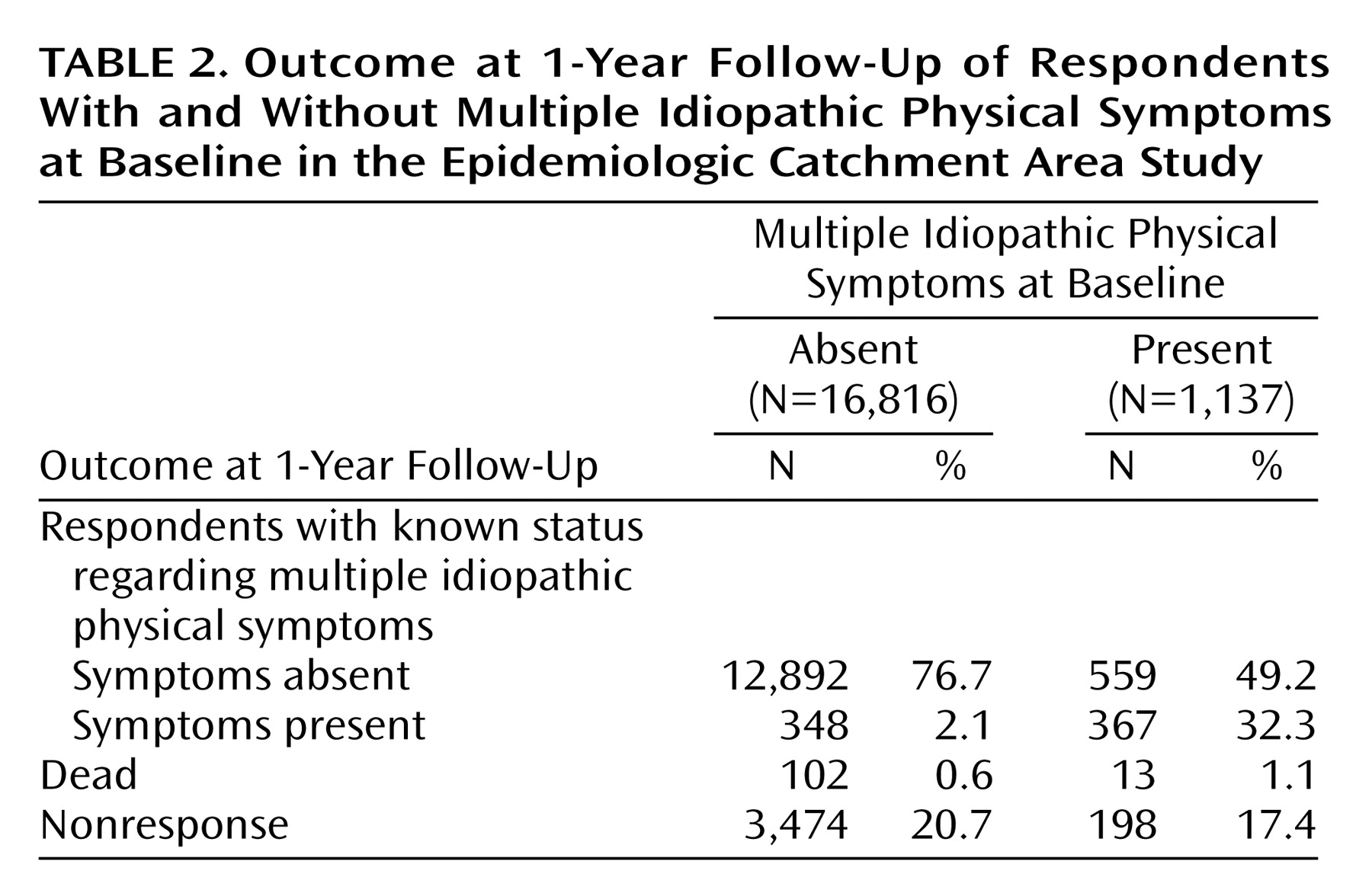
Table 2 presents the distribution of the respondents by baseline and 1-year status in regard to multiple idiopathic physical symptoms. Of those who did not meet our criteria for multiple idiopathic physical symptoms at baseline (16,816 persons), about 0.6% died within the period of follow-up; 96.6% of the respondents completing the 1-year follow-up (including the deceased subjects) did not have multiple idiopathic physical symptoms 1 year later. Of the respondents completing the 1-year follow-up, 2.6% developed multiple idiopathic physical symptoms within the 1-year period. About two in 10 individuals without baseline multiple idiopathic physical symptoms failed to respond to the survey at 1-year follow-up. Compared with those without baseline multiple idiopathic physical symptoms, individuals with multiple idiopathic physical symptoms were about twice as likely to die and were slightly less likely to be nonrespondents at the 1-year follow-up. The probability of recovering from multiple idiopathic physical symptoms within the 1-year period was sizable. More than one-half (59.5%) of those completing the 1-year follow-up who had multiple idiopathic physical symptoms at baseline had recovered from the syndrome 1 year later. These actual values describe the sample, while subsequent figures use multinomial logit modeling to generate population estimates. Sample values may differ considerably from population values predicted from statistical modeling.
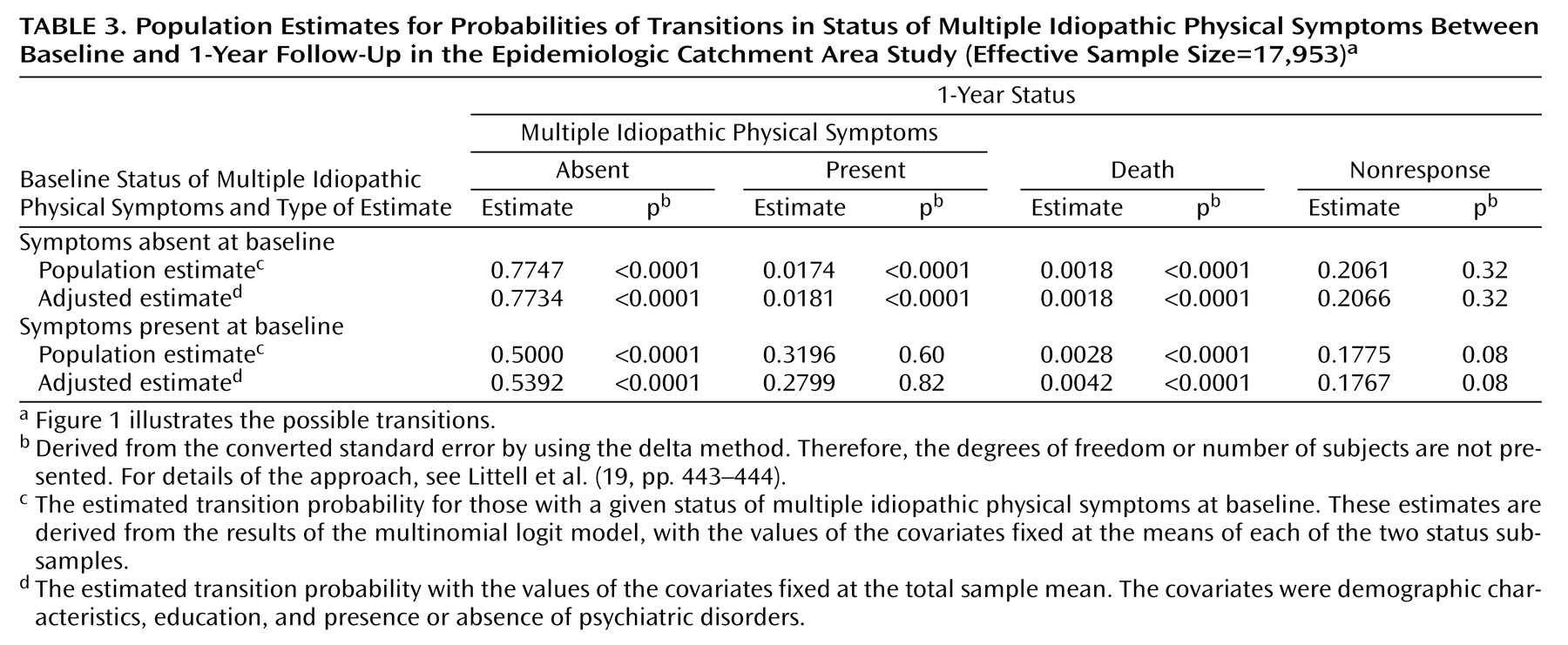
Table 3 shows the two sets of population estimates of the eight transition probabilities, derived from the multinomial logit model. Since the dependent variable of a multinomial logit analysis consists of a series of log odds (12), interpretation of the regression coefficients and odds ratios is less than intuitive
(13). Accordingly, these coefficients and odds ratios, available on request, are not presented here. Instead, we present the previously described population and adjusted population estimates of transition probabilities (
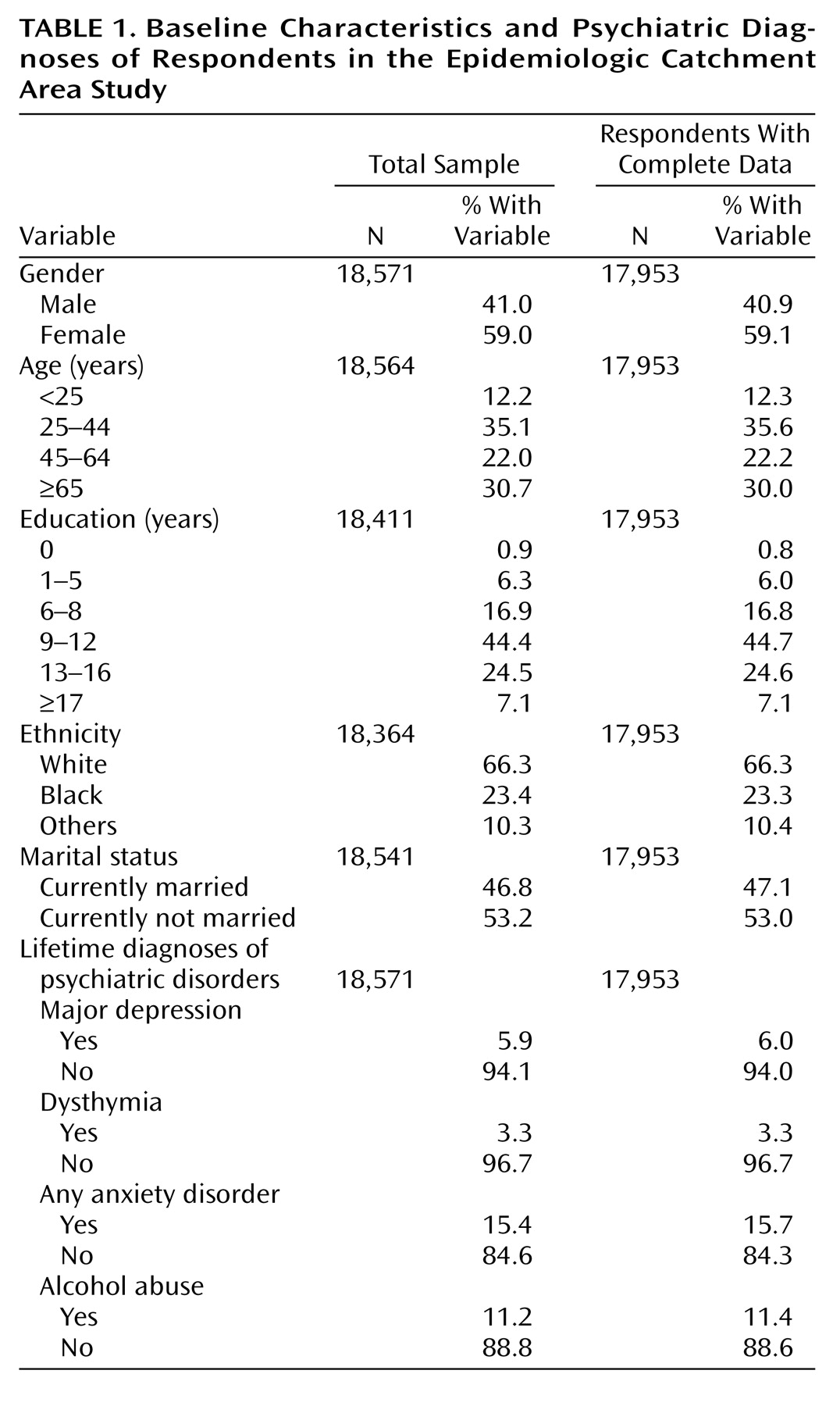
Table 3). Estimated mortality was higher among those with multiple idiopathic physical symptoms at baseline than among those without such symptoms (0.28% versus 0.18%) (z=2.42, N=17,953, p=0.02). This elevation in estimated mortality persisted after adjustment for differences between groups in major depression, dysthymia, anxiety disorders, alcohol abuse, and demographic characteristics, as shown by the second set of population estimates (0.42% versus 0.18%) (z=5.09, N=17,953, p<0.0001).
Table 3 shows the estimated probability that a U.S. adult would undergo no transition in status regarding multiple idiopathic physical symptoms from the baseline survey to the 1-year follow-up (0.7747 for subjects without multiple idiopathic physical symptoms at baseline and 0.3196 for the smaller group with such symptoms at baseline). The estimated probability of developing multiple idiopathic physical symptoms over the period in a respondent who did not have such symptoms at baseline was approximately 0.0174 (equivalent to an estimated 1-year incidence of 1.74 per 100 person-years; z=6.68, N=17,953, p<0.0001), while the estimated probability of recovery among the respondents at 1 year who had had multiple idiopathic physical symptoms at baseline was 0.5000 (equivalent to an estimated 1-year resolution rate of 50 per 100 person-years; z=66.99, N=17,953, p<0.0001). Among respondents with multiple idiopathic physical symptoms at baseline, the estimated probability of being lost to follow-up a year later was 0.1775 (z=1.77, N=17,953, p=0.08) compared to an estimated probability of 0.2061 among those without multiple idiopathic physical symptoms at baseline (z=1.01, N=17,953, p=0.32). Because at least one transition probability in each probability set was statistically significant, all these probabilities were considered statistically meaningful. These estimated probabilities were essentially unchanged after adjustment for major depression, dysthymia, any anxiety disorder, alcohol abuse, and group demographic differences, as shown by the adjusted probability estimates (demonstrated by the second set of population estimates in
Table 3).
Discussion
Several limitations of our analysis should be noted. First, differences in mortality between respondents with and without multiple idiopathic physical symptoms were small, and therefore, misclassification of death, particularly in the group of follow-up nonrespondents, could confound the relationship of multiple idiopathic physical symptoms to mortality. Second, although multinomial logit regression accounts for nonresponse in the estimation of the association between multiple idiopathic physical symptoms and competing outcomes, we cannot eliminate the possibility of nonresponse bias. Third, given the panel data available for this analysis, we used logistic regression to model determinants of outcome. This procedure does not account for the amount of time that elapsed before the outcomes occurred. If the exact timing of an outcome (e.g., death) is available, then a hazard-rate approach would be more appropriate. Fourth, the sample was followed only for 1 year. A longer period of follow-up would allow greater elucidation of mortality patterns over time. Finally, some might question the relevance of data collected almost two decades ago. While this is a limitation, we know of no direct evidence suggesting changes in the occurrence of multiple idiopathic physical symptoms over the past two decades. The ECA survey continues to be among the most frequently cited epidemiological surveys of psychiatric illness and perhaps the only one to involve a comprehensive etiological assessment of such a wide range of physical symptoms in a population-based sample.
In spite of these limitations, we found a modest but meaningful and statistically significant relationship between multiple idiopathic physical symptoms and subsequent mortality. The relationship persisted and was perhaps even strengthened after adjustment for potential confounding due to major depression, dysthymia, any anxiety disorder, alcohol abuse, and various demographic characteristics, therefore suggesting a substantial and independent impact of multiple idiopathic physical symptoms on mortality. Although the 1-year risk of death rates was low (0.28% versus 0.18%), over an extended period these mortality differences might lead to important population differences (e.g., at a constant rate, over a decade mortality would reach 2.8% among individuals with multiple idiopathic physical symptoms versus 1.8% among those without such symptoms). We cannot assume, however, that rates or differences remain stable over time, and therefore, population-based studies allowing more extended follow-up are necessary.
Future research should explore the possible mechanisms by which multiple idiopathic physical symptoms could lead to increased mortality. A number of explanatory pathways seem plausible, and many or all may be operative. First, multiple idiopathic physical symptoms may sometimes be unrecognized manifestations of a progressive disease
(20). Although symptoms were classified as medically explained or unexplained in the ECA survey, information regarding comorbid medical illness at baseline was not obtained. This explanation, if operative, would appear to occur only rarely among those suffering with multiple idiopathic physical symptoms, because we found that over one-half of those with multiple idiopathic physical symptoms were recovered 1 year later. This is consistent with findings from existing studies suggesting that individuals with idiopathic symptoms seldom manifest serious and previously occult disease on subsequent follow-up
(1).
A second potential explanation for greater mortality among those with multiple idiopathic physical symptoms involves comorbidity with many mental disorders
(5,
21,
22). Mortality may be mediated by some combination of disabling symptoms, impaired coping, and one or more coexisting mental disorders that leads to increases in death by accidental and nonaccidental means. However, even after we controlled for a number of these disorders, the relationship between multiple idiopathic physical symptoms and mortality only strengthened, suggesting that multiple idiopathic physical symptoms represent an independent mortality risk factor.
Third, the observed difference in mortality may be a function of altered health behaviors consequent to the onset of multiple idiopathic physical symptoms. The presence of physical symptoms may usher in the development of such adverse health behaviors as smoking, drinking, and lack of exercise. For example, Walker and colleagues
(23) found that childhood adversity was associated with multiple idiopathic physical symptoms and with behaviors associated with increased health risk. The influence of such behaviors on health is increasingly well known and may help explain the observed association between multiple idiopathic physical symptoms and a higher mortality rate
(24,
25).
Fourth, a higher mortality rate among individuals with multiple idiopathic physical symptoms may occasionally occur from the iatrogenic impact of aggressive biomedical management, such as unnecessary and invasive surgery and diagnostic testing, as well as the adverse effects of medications used to treat symptoms
(26,
27).
Significant cultural, racial, and ethnic differences in the relationship between multiple idiopathic physical symptoms and mortality may exist
(28). These factors may affect such issues as symptom reporting, health-related behaviors, and the seeking of help for physical symptoms. We adjusted our estimates for differences in available demographic characteristics, such as ethnicity, marital status, and education. However, because of the relatively small number of deaths occurring over the follow-up period, we were unable to reliably ascertain the specific impact of ethnic differences on the relationship between multiple idiopathic physical symptoms and mortality. This should be the specific focus of future national and cross-national epidemiological research.
Finally, we used a competing-risks model as a way of broadening research on the relationship between multiple idiopathic physical symptoms and mortality. The use of similar statistical modeling techniques can broaden the awareness of dynamic processes involved in health outcomes associated with multiple idiopathic physical symptoms. For instance, a competing-risks model can be used to examine the possible influence of nonresponse bias on the relationship between multiple idiopathic physical symptoms and mortality.
In sum, our results confirm the important health impact of multiple idiopathic physical symptoms on those who suffer from them. The fact that multiple idiopathic physical symptoms have an important effect on functioning
(29), distress
(30), and mortality suggests that more efforts are needed to study the ways such symptoms alter health and health behaviors. Determinants of poor prognosis and effective clinical management strategies should be investigated. Perhaps most important, the lens through which many clinicians view multiple idiopathic physical symptoms and their patients who suffer from them requires careful assessment. Elevated morbidity and mortality rates among these individuals challenge our heretofore largely biomedical sense of such patients as simply “worried well” who suffer from “nondisease.”
 where β represents the matrix of regression coefficients to be estimated. This equation defines a given log odds as a linear function of model covariates (12).
where β represents the matrix of regression coefficients to be estimated. This equation defines a given log odds as a linear function of model covariates (12).