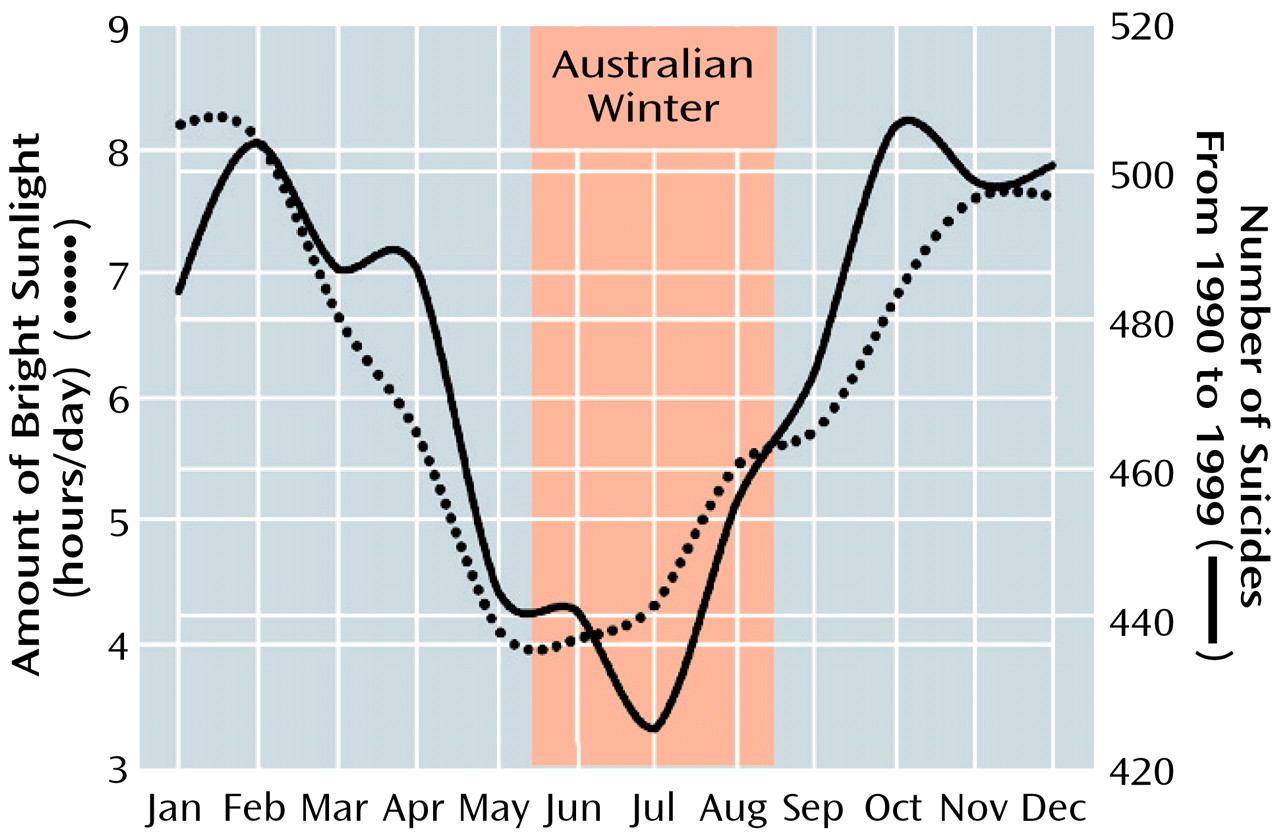
In this study, we found that the incidence of suicide in the state of Victoria in southeastern Australia was at its lowest in winter and highest during the spring and summer and that it paralleled the daily hours of bright sunlight. Over the study period encompassing the past decade, there was a significant increase in the suicide rate among men 21–60 years of age and among women 41–60 years of age.
The observation that the incidence of suicide displayed an annual variation with, in the majority of instances, the peak occurring in spring, is in agreement with a number of studies undertaken in the Northern and Southern Hemispheres
(3–
7). We found a significant increase in the rate of suicide to be evident only in those subjects 21–40 and 41–60 years of age. This observation is not in accordance with data derived from England and Wales, where the suicide rate in men and women has recently been reported to have declined during the period 1990–1997
(8).
There exists a large body of evidence indicating that subjects with mental illness contribute disproportionately to the overall incidence of suicide
(1) and that the occurrence and severity of some affective disorders, such as depression and mania, are more pronounced in the spring and summer period
(2,
9,
10). Maes et al.
(5) demonstrated a clear springtime peak in violent suicide and observed a positive correlation between the seasonality of depression severity and the frequency of suicide
(2). In line with this observation, Morken and Linaker
(11) found the frequency of violence in Norway to be correlated with changes in day length and noted that the incidence of violent episodes increased with latitude. In their comprehensive examination of suicide across 28 countries, Chew and McCleary
(6) concluded that the degree of seasonal variation in suicide is high in the temperate zones (between 30° and 60° north and south of the equator) and low in populations in the tropics. Whether latitude per se provides a reliable indicator of climatic variation is problematic—many places of similar latitude have markedly different climates. This is especially so for large countries such as Australia or the United States. Our observation of a strong association between suicide and sunlight hours and other reports documenting higher rates of suicide in springtime raise concerns about a possible link between suicide and bright light exposure. While there exists a small number of case reports documenting suicide attempt following bright light therapy
(12), Lam and colleagues
(13), in their retrospective examination of almost 200 case records, found that only 3% of seasonal affective disorder patients experienced a slight worsening of suicide scores following light therapy. Moreover, no patient attempted suicide or discontinued light therapy because of perceived elevated suicide risk
(13).
We have demonstrated that the incidence of suicide in southeastern Australia displays a clear seasonal pattern, being positively linked with prevailing levels of sunlight. Moreover, the rate of suicide increased in the latter half of the last decade. While it is tempting to speculate on the importance of an environmental cue in predisposed individuals that results in depressed affect or suicidal ideation, it is clear that social issues such as possible reductions in the availability of mental health care and disintegration and loss of community
(14) should be considered in parallel.