Two trends of the past decade have had a major influence on clinical trials of new drugs to treat schizophrenia: 1) increasing concerns about whether the use of drug washout periods is ethical
(1–
3) and 2) the transition to use of “atypical” antipsychotic drugs in clinical practice
(4). It has become widely assumed, although far from proven
(5), that atypical antipsychotics as a group, in addition to having more favorable extrapyramidal side effect profiles, show superior efficacy, compared with traditional antipsychotic drugs. Much of this belief is based on the demonstrated superiority of clozapine in comparison with traditional antipsychotic drugs and the comparability of other atypical antipsychotics to clozapine in subsequent clinical studies
(5,
6). The superiority of atypical antipsychotics, other than clozapine, in direct comparison to traditional agents in treating the core symptoms of schizophrenia is only modestly supported by clinical trials
(5).
It has been hypothesized that antipsychotic discontinuation may negatively influence pathophysiological mechanisms and clinical outcome in schizophrenia
(7), although this thesis remains controversial
(8–
12). Whereas it is untenable to argue that psychotic exacerbation brought about by the discontinuation of antipsychotic drug treatment is experientially benign, the effects of drug withdrawal on outcome or on subsequent response to drug treatment remain to be more clearly elucidated. Moreover, as drug development proceeds to include potential antipsychotic drugs with unproven underlying mechanisms, the utilization of drug-free periods will be needed for critical proof-of-concept experiments
(13). Drug washout periods also remain important for establishing levels of symptoms and biological parameters characteristic of an individual’s illness without the “contamination” of existing drug treatment
(9–
11). Indeed, the definition of drug response as a change from a drug-free condition has become increasingly important with the development of pharmacogenetic studies in which data on candidate genes associated with specific brain processes are used to predict the outcome of drug treatment
(14).
Clinical trials whose goal is to lead to approval of a drug by the U.S. Food and Drug Administration
(15) employ a parallel design in which one arm may include a placebo treatment. These studies also characteristically rely on truncated placebo arms (i.e., not all patients complete the treatment period) and often use the last-observation-carried-forward method, in which the last ratings before dropout are carried forward to the endpoint
(16,
17). Patient dropout, however, may precede psychotic symptom exacerbation
(18). For this reason, it is not surprising that placebo arms in these studies often show modest or no symptom exacerbation
(16), despite the prevailing understanding that patients removed from antipsychotic treatment worsen substantially.
In this paper we report data from studies involving patients with treatment-resistant schizophrenia treated on an intramural NIMH research ward. The studies examined the behavioral effects of drug washout and subsequent treatment with clozapine and were carried out under double-blind treatment conditions. Behavioral change after discontinuation of antipsychotic treatment was quantified, and the hypothesis that symptom exacerbation during washout negatively affects future drug response was tested.
Discussion
This study demonstrates that patients with schizophrenia who meet the criteria for treatment resistance
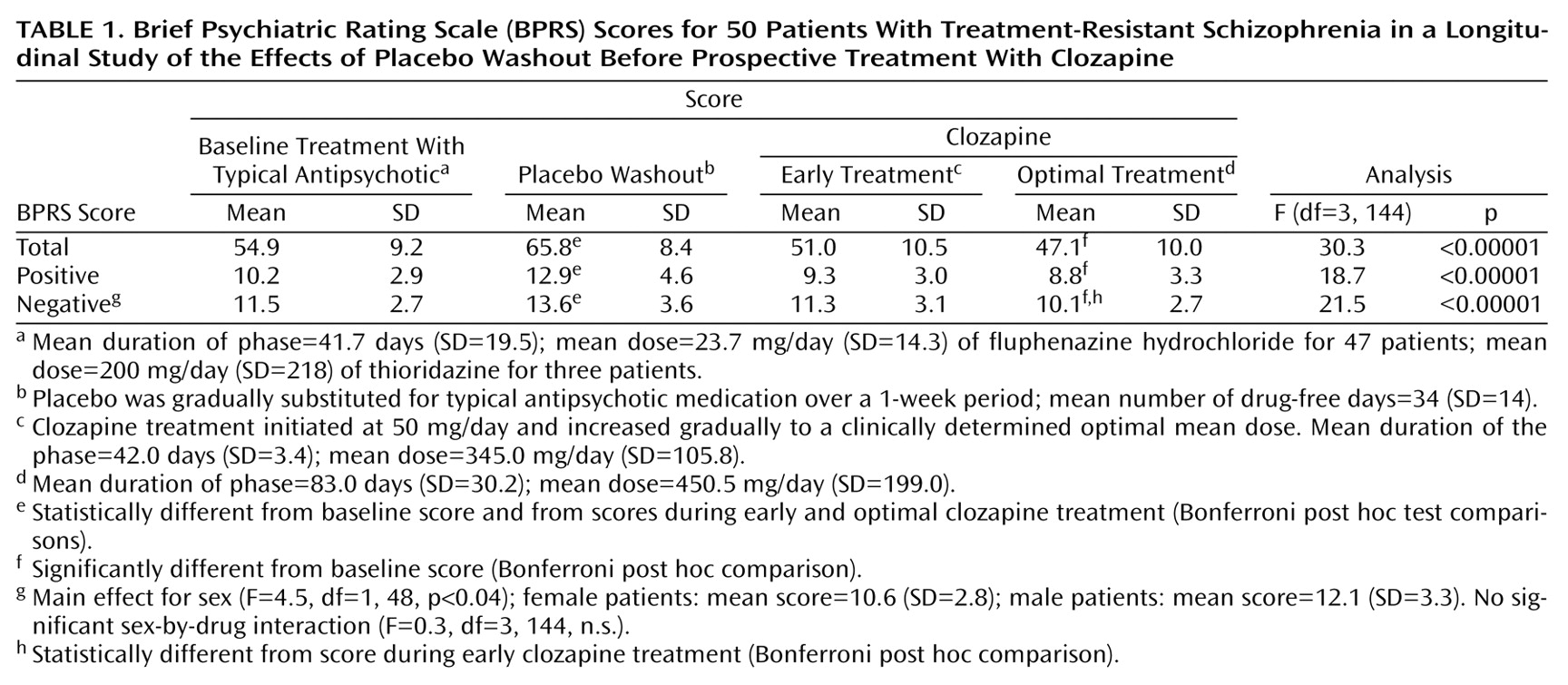
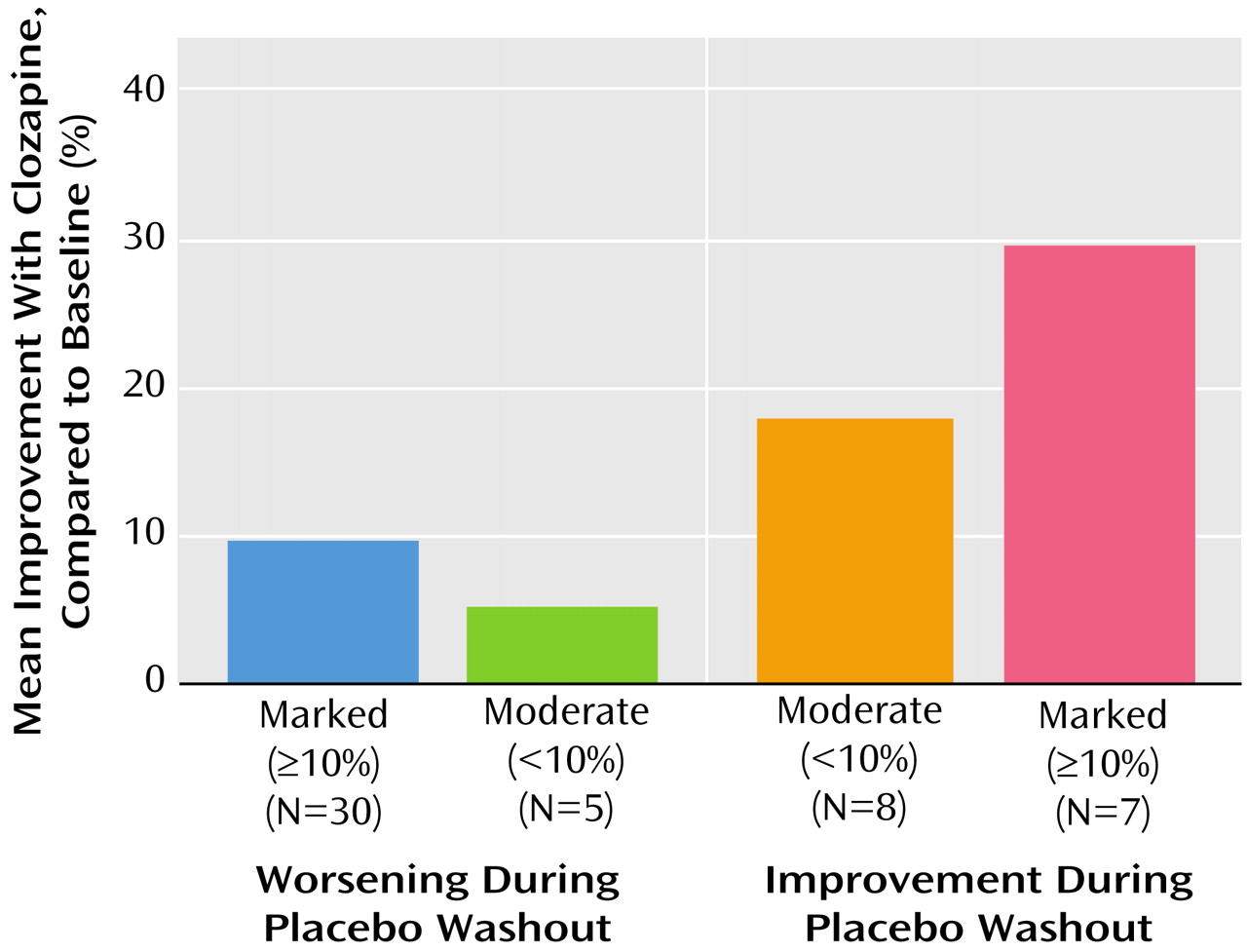
(20) show symptom exacerbation after the discontinuation of chronic treatment with a typical antipsychotic. However, the clinical deterioration induced by drug withdrawal does not appear to negatively affect subsequent response to treatment with clozapine. Group mean BPRS scores showed that clozapine treatment resulted in a significant improvement in symptoms, compared with both placebo and baseline treatment with a typical antipsychotic. Individual patient data revealed that although a majority (60%) of patients showed marked deterioration (≥10% worsening) after discontinuation of baseline drug treatment, some patients actually had a decrease in symptoms after drug discontinuation. It is interesting to note that patients whose symptoms decreased the most during drug washout showed marked further improvement during clozapine treatment, suggesting that, at least for some patients, responsiveness to typical antipsychotic treatment should not necessarily be equated to responsiveness to clozapine. It should be considered, however, that the study had no control condition for clozapine response in patients without a prior drug withdrawal period, raising the possibility that drug withdrawal compromised the degree of clozapine-induced improvement that might otherwise have been seen. Moreover, drug withdrawal could have different effects when carried out at different stages of the illness, for example, after a first break or during recovery from an acute psychotic exacerbation of chronic illness.
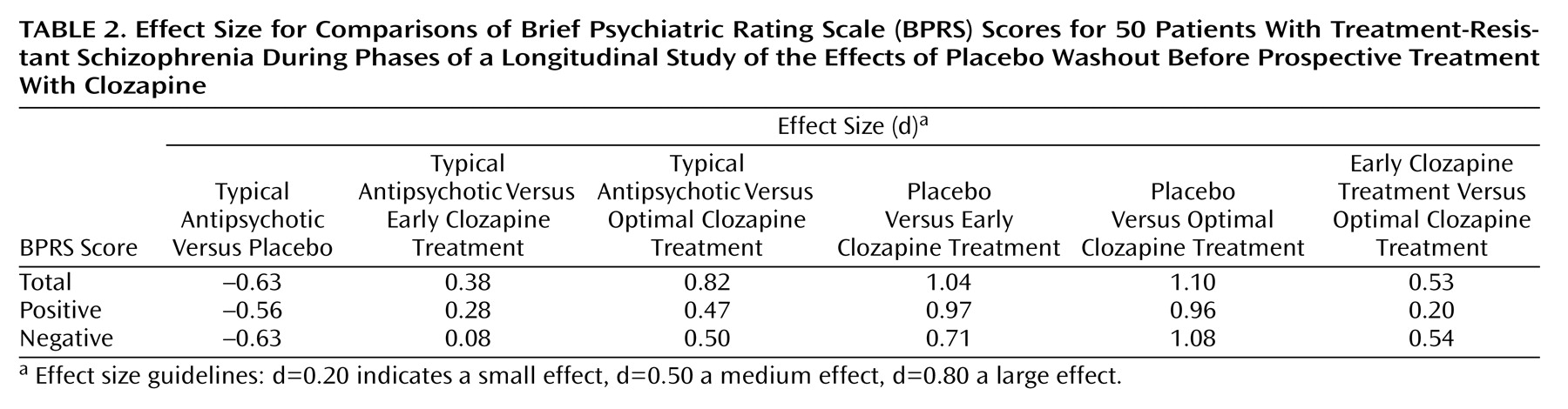
The sensitivity of patients with treatment-resistant schizophrenia to drug discontinuation suggests that the concept of “treatment resistance” is far from absolute. The clinical characteristics of the patients in our study were typical of seriously ill patients with schizophrenia
(19), although the selection criteria for NIMH research studies minimize the inclusion of patients at high risk for violence or severe noncompliance. The effect size of 0.63 for drug discontinuation for the overall group for the BPRS total score was between the accepted levels of medium (d=0.50) and large (d=0.80), although the exclusion of more uncooperative patients, as well as the ready availability of intervention if clinical deterioration was detected, may have led to underestimation of the actual effect size of drug withdrawal. Although the design of this study addressed response to traditional antipsychotic treatment through the “window” of drug discontinuation, it did emphasize that the identification of an “inadequate” response to prior trials of typical antipsychotics is relative. Clinical studies whose patient selection criteria may exclude patients with “treatment-resistant” disorders in order to reduce the number of nonresponsive patients in the clinical trial population in which a new drug is tested may be unwisely excluding a patient group that could provide valuable data. Measurement of behavioral change after discontinuation might be the best way to identify patients with inherent responsiveness to traditional antipsychotic treatment.
The enhanced therapeutic effectiveness of clozapine in seriously ill patients with schizophrenia was again demonstrated in this study. Statistically significant improvement during optimal clozapine treatment, compared to baseline treatment with a typical antipsychotic, for BPRS total and positive and negative symptom scores was clearly demonstrated. Early clozapine treatment, however, while associated with statistically significant improvement compared with placebo, was not significantly different in effectiveness from baseline treatment with a typical antipsychotic. The greater effectiveness of optimal clozapine treatment than early clozapine treatment, in relation to baseline treatment with a typical antipsychotic, would appear to be related to the interaction of time (longer treatment) and dose (higher dose). It is interesting to note that the negative symptom score was the only treatment variable that showed statistically significant superiority of optimal clozapine treatment, compared with early clozapine treatment, supporting the need for prolonged treatment with clozapine to elicit its full effects on some treatment complexes
(28).
Effect size provides a measure by which variable difference is “standardized,” i.e., it is expressed in relation to the variation (standard deviation). For this reason, effect size is well suited for comparison of results across studies
(29). In this study, very large effect sizes for BPRS total scores were found for both early and optimal clozapine treatment, compared with placebo (d=1.04 and d=1.10, respectively). Most studies comparing clozapine (or other atypical antipsychotics) with typical antipsychotics have been carried out by using a randomized, multiarm parallel design in which one group of patients is treated with a typical antipsychotic and another group is treated with clozapine
(5). The longitudinal design used here enabled the assessment of drug-free symptom levels, a critical component for biological research and rater consistency; this design enhances power while including a smaller number of subjects
(30,
31). It is interesting to note that the effect size of 0.82 for the BPRS total score for optimal clozapine treatment, compared with baseline treatment with a typical antipsychotic, is nearly identical to the effect size of 0.81 calculated by Chakos et al.
(5) for the study by Kane et al. (20) comparing clozapine and chlorpromazine in a parallel design. In contrast to the large effect size for the BPRS total score, medium effect sizes were found for positive (d=0.47) and negative (d=0.50) symptom scores for optimal clozapine treatment, compared to baseline treatment with a typical antipsychotic, lending some support for the idea that these symptom complexes may not be the most sensitive to the therapeutic effects of clozapine
(32).
Our study findings also suggest that a placebo-controlled, multiarm, parallel-design clinical trial with truncated treatment arms (e.g., last observation carried forward) may substantially underestimate behavior indicating clinical deterioration during placebo treatment. For example, examination of results for BPRS total scores from the placebo arm of studies by Marder and Meilbach
(33) and Beasely et al.
(34)—clinical trials that examined the effects of risperidone and olanzapine, respectively, compared to placebo—showed a mean change of 3% and an effect size of 0.15 in the former and a mean change of 8% and an effect size of 0.18 in the latter. In both studies, the mean change in scores and the effect size are substantially smaller than the mean change of 20% and the effect size of 0.63 found in our study. However, for the 58% of the patients in our study who showed a marked symptom exacerbation during drug washout (≥10% increase in symptom ratings), symptom ratings worsened by a mean of 43% during placebo washout, compared with baseline treatment with a typical antipsychotic, and a very large effect size of 1.5 was found. Thus, underestimation of placebo response may be particularly pronounced in studies that include patients with schizophrenia that is not treatment resistant. Relapse rate—a variable that is difficult to connect to symptom ratings—after neuroleptic withdrawal has been shown to increase over time, with a 50% relapse rate occurring at approximately 6 months after neuroleptic withdrawal and with time to relapse influenced by the rate of drug discontinuation
(35,
36).
Our findings provide some support for the idea of “treatment resistance” to conventional antipsychotic medication insofar as 30% of the patients improved during the drug washout. It is interesting to note that the patients who improved during the drug washout showed further improvement during clozapine treatment. Although these findings are difficult to interpret, they give some credence to the possibility that some patients have differential responsiveness to traditional antipsychotic treatment and to clozapine.
In summary, our study provides data regarding the effect size of drug discontinuation in seriously ill patients with schizophrenia in a research ward setting. The concept of treatment resistance is a relative one, and patients who meet the criteria for treatment-resistant disorders are not necessarily insensitive to drug treatment. Our study also demonstrates that symptom exacerbation induced by drug withdrawal does not appear to negatively affect the effectiveness of subsequent treatment with clozapine. The study findings highlight the need for designers of multiarm, parallel-design clinical trials to use caution when including a truncated placebo arm as a comparator to antipsychotic treatment, particularly if the study involves proof-of-concept of a new mechanism. Finally, in this study, clozapine again displayed an enhanced therapeutic profile, compared to traditional antipsychotic treatment, with the greatest effectiveness for clozapine seen over time (>6 weeks) at a dose of approximately 450 mg/day.