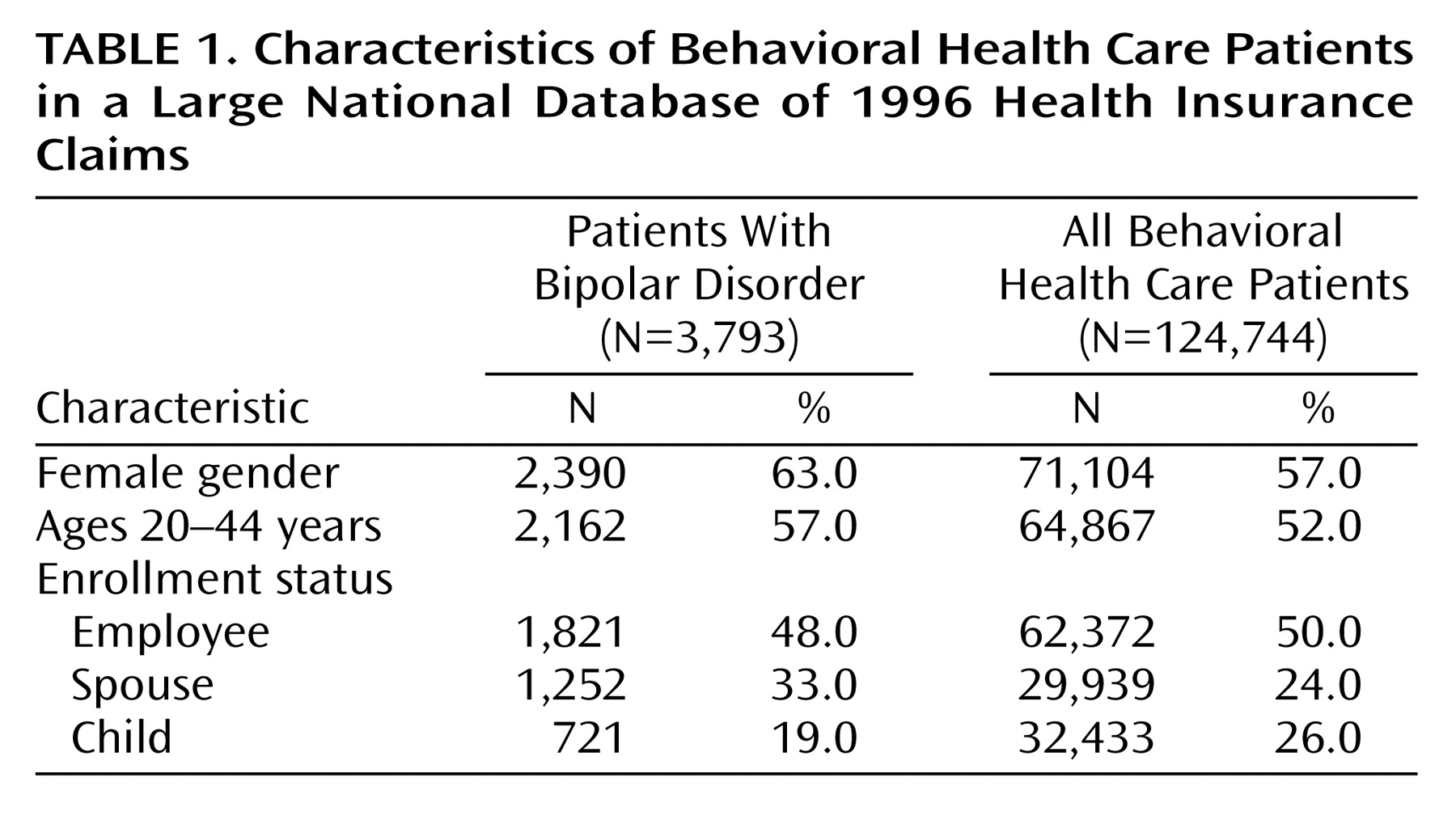
There were approximately 1.66 million covered individuals; of these, 7.5% (N=124,744) filed at least one insurance claim for a behavioral health care service received in 1996. Only 0.2% (N=3,793) of all covered individuals filed a behavioral health care claim for bipolar disorder.
Inpatient Hospital Admissions
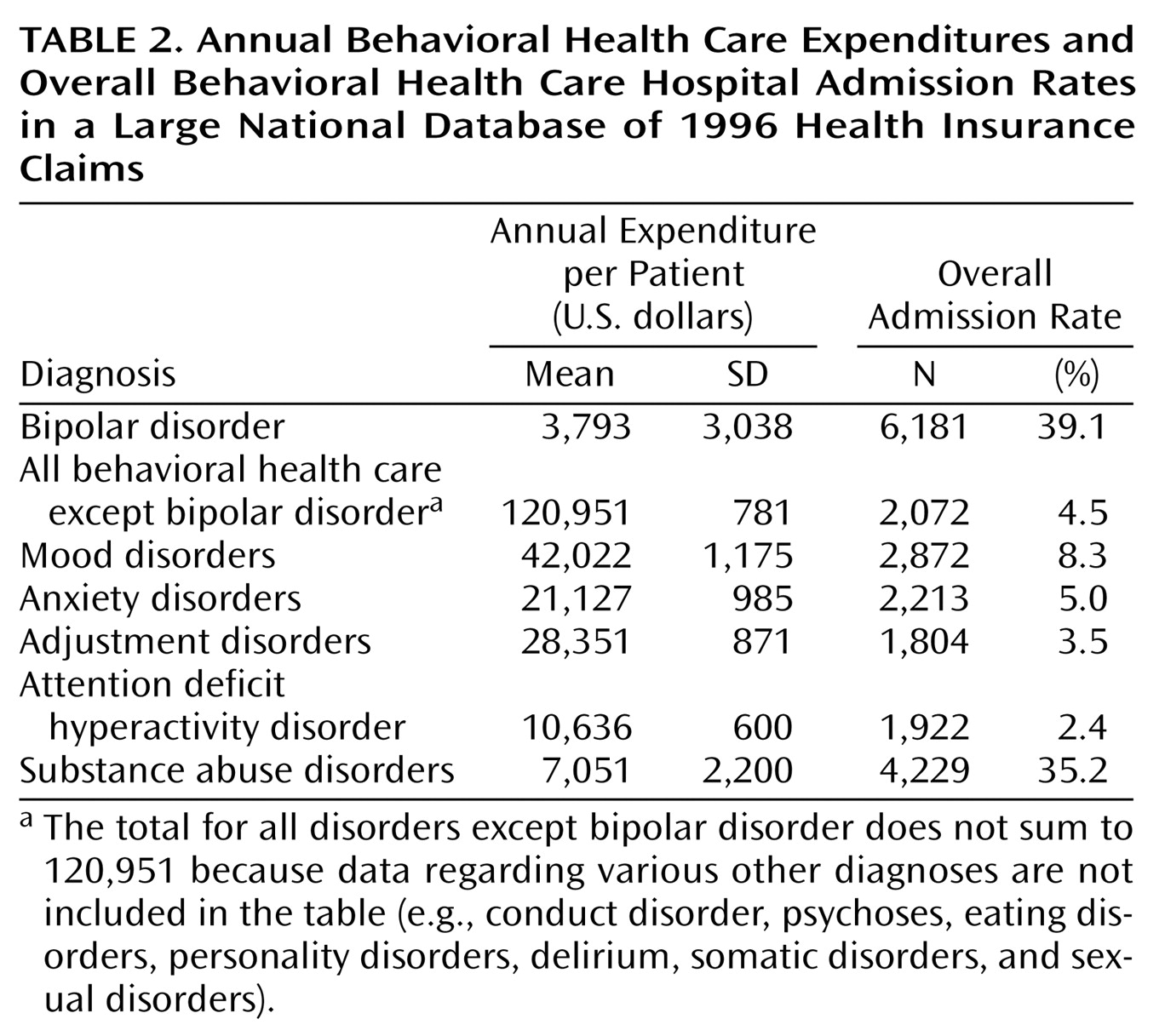
A total of 21.0% (N=797) of all of the bipolar patients identified had at least one behavioral health care hospital admission during 1996, which resulted in an annual inpatient behavioral health care hospital admission rate of 39.1%, surpassing even the 35.2% behavioral health care hospital admission rate for patients with substance abuse diagnoses. Furthermore, they had a high specific bipolar disorder hospital admission rate of 13.3% (N=504). Among patients with bipolar disorder who had a behavioral health care hospital admission during 1996, 6.9% (55 of 797) had more than 30 behavioral health care inpatient days.
Table 2 presents a comparison of behavioral health care expenditures and behavioral health care inpatient hospital admission rates between patients with bipolar disorder and patients with other behavioral health care diagnoses.
Behavioral health care hospital admission rates were particularly high among adolescents with bipolar disorder (12–19-year-olds). A total of 39.6% (188 of 475) of the adolescents with bipolar disorder had at least one behavioral health care inpatient hospital admission during the year, and approximately one-half of those had more than one behavioral health care hospital admission during the year, resulting in a high (84.6%, N=402) behavioral health care hospital admission rate for the adolescents with bipolar disorder. Congruent with the fact that multiple hospital admissions are common among adolescents with bipolar disorder who were ever hospitalized, adolescents had more behavioral health care hospital admissions per year than the adult patients with bipolar disorder who were ever hospitalized (rate: 2.14 versus 1.76, respectively).
Among the adults with bipolar disorder, employees experienced significantly fewer (χ2=15.15, df=1, p<0.001) behavioral health care hospital admissions during 1996 than the spouses with bipolar disorder (15.8%, 287 of 1,821, versus 21.2%, 269 of 1,267, respectively).
Behavioral health care hospital admissions were high among the patients with bipolar disorder in our data, but so were medical admissions, indicating high rates of medical comorbidity. Medical insurance claims records were available for 2,910 of the bipolar patients in this study. Among those patients, we observed that 22.0% (N=641) had at least one medical admission during the year compared to 8.6% (N=8,356) of the individuals with all other behavioral health care diagnoses in the same data subset (N=97,167). Furthermore, among the 620 patients with bipolar disorder in this data subset who experienced a behavioral health care hospital admission during the year, 85.0% (527 of 620) also experienced a medical admission during the same calendar year. By comparison, among patients with bipolar disorder with no behavioral health care hospital admissions (N=2,290), only 5% incurred a medical admission during the year. Given the high medical admission rates among patients with bipolar disorder with behavioral health care hospital admissions, it is not surprising that their average medical insurance expenditures were significantly higher (t=17.97, df=769.63, p<0.001) than those for patients with bipolar disorder without behavioral health care hospital admissions ($12,433 versus $3,044 per patient).
Expenditures for Care
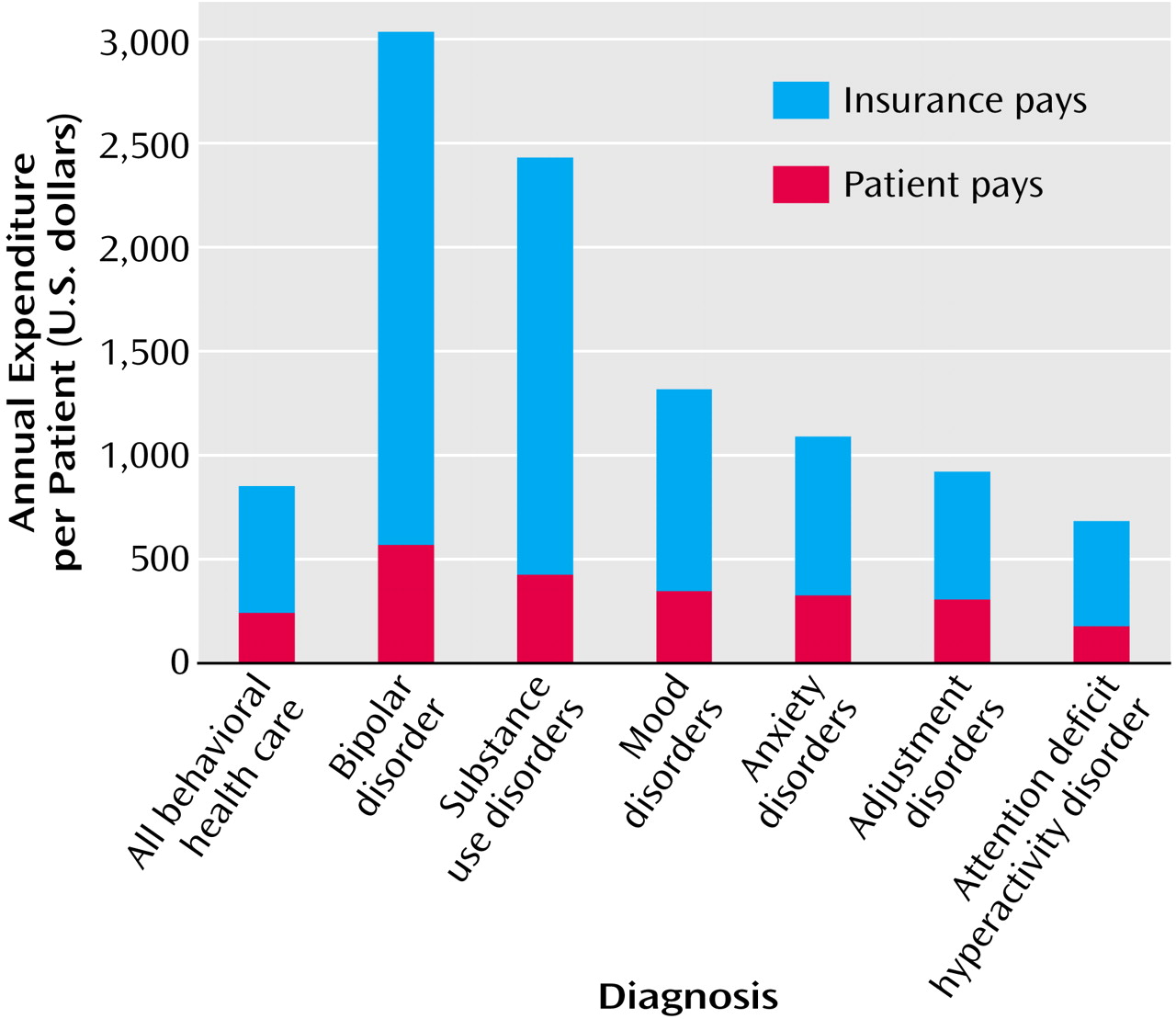
Consistent with the high behavioral health care hospital admission rate we reported, behavioral health care expenditures for patients with bipolar disorder were significantly higher than those for patients with all other behavioral health care diagnoses (t=22.45, df=3,818.78, p<0.001) (
Figure 1). A total of 59.9% (N=602) of those with bipolar disorder in the study were high service users of outpatient care as defined by having 20 or more behavioral health care outpatient visits per year.
Insurance plans pay significantly more (t=21.62, df=3,817.50, p<0.001) for behavioral health care for patients with bipolar disorder than for patients with other behavioral health care diagnoses, including substance abuse disorders, mood disorders, anxiety disorders, adjustment disorders, or ADHDs. Insurance plans pay an average of $2,470 per patient per year for behavioral health care for patients with bipolar disorder, a full 400% more per patient per year on average for behavioral health care than for all other claimants. Patients with bipolar disorder themselves pay an estimated $568 out of pocket annually for their care, which significantly surpasses the $232 annual out-of-pocket payments made by patients with all other behavioral health care diagnoses (t=17.57, df=3,830.08, p<0.001). Nonetheless, patients with bipolar disorder bear a lower proportion of their total behavioral health care expenditures, paying 18.7% ($568 of $3,038) of the cost out of pocket compared to 29.7% ($232 of $781) paid by all other behavioral health care patients.
Overall, 3.0% of all behavioral health care patients in our study were treated for bipolar disorder during 1996, but those 3.0% accounted for 12.4% ($9.4 million of $75.8 million) of total behavioral health care expenditures. High expenditures for behavioral health care for patients with bipolar disorder were driven by the disproportionately high use of inpatient care by these patients. For every $1.00 the insurance plans spent for outpatient care for patients with bipolar disorder, $1.80 was spent for inpatient care. Insurers also incurred higher mean annual expenditures for covered medical services for patients with bipolar disorder than for patients with other behavioral health care diagnoses.