Antipsychotic medications represent the cornerstone of pharmacological treatment for patients with schizophrenia. Although these agents have been shown to improve psychopathology, reduce relapse, and improve functioning (DSM-IV-TR), nonadherence to treatment with antipsychotics is common. Nonadherence rates ranging from 20% to 89%, with an average rate of approximately 50%, have been reported
(1–
3). Among patients with schizophrenia, nonadherence to maintenance treatment with antipsychotic medication is associated with a greater number of clinic and emergency room visits and more psychiatric hospitalizations
(4–
6). Improving adherence to treatment with antipsychotic medication in patients with psychotic disorders is a complex task
(7,
8). Identifying risk factors associated with nonadherence is an important initial step because modifiable risk factors might become targets for future interventions. Estimating the medical costs of nonadherence—including those associated with psychiatric care, physical health care, and pharmaceuticals—would provide information on the overall economic impact of adherence and might create an incentive for insurers to allocate resources to improve adherence in this population.
We examined nonadherence to treatment with antipsychotic medication among Medicaid beneficiaries with schizophrenia in San Diego County, Calif., using a unique data set that linked Medi-Cal eligibility and claims files to individual-level information on ethnicity and living situation. San Diego County provides a suitable sample to investigate nonadherence because of its size (it is the sixth largest county in the United States), its diverse ethnic composition (19% Latinos, 18% African Americans, and 6% Asians
[9]), and the predominance of fee-for-service payment for disabled beneficiaries, which allows accurate capture of health services and pharmacy use in a claims database. This analysis builds on previous research
(5,
10) by examining a full range of health care services and costs in an ethnically diverse population in a large metropolitan area.
We analyzed risk factors associated with adherence, including age, gender, ethnicity, comorbid substance abuse disorder, living situation, and antipsychotic regimen (atypical, typical, and polypharmacy). We also examined the relationship of nonadherence to psychiatric and medical hospitalizations and the health care costs related to nonadherence. We had the following hypotheses: 1) Individuals prescribed atypical antipsychotic medication would have greater adherence to treatment than those receiving conventional antipsychotics. 2) Individuals residing in supervised living situations (i.e., assisted living, living with family) would have greater adherence to treatment than those in less supervised environments (i.e., living alone, homeless). 3) Individuals who were nonadherent would have a higher likelihood of acute psychiatric hospitalization and thus greater hospital costs and lower pharmacy costs than those who were adherent. We did not expect differences in medical hospitalization or outpatient costs, and we had no expectations regarding overall costs of health care.
Method
We used data from San Diego County Adult Mental Health Services to identify individuals diagnosed with schizophrenia by a specialty mental health provider and living in the community during fiscal years 1999 and 2000. Variables extracted from these data included ethnicity, the most commonly recorded (modal) living situation (which had been assessed at each use of service), and whether a substance use disorder was diagnosed. Living situation assignment included 1) living independently, 2) living with family members, 3) living in an assisted living facility, or 4) being homeless. We excluded subjects who were primarily institutionalized or residing in jails because of their inherent differences in service use and our interest in populations that might benefit from community-based interventions to improve adherence. We have previously used the county database to examine the differential use of services by age, gender, and ethnicity
(11–
13).
We merged the individual-level data from Adult Mental Health Services with 3 years of data on Medi-Cal eligibility and claims (1998–2000) and identified fee-for-service beneficiaries continuously enrolled over the course of a year who filled at least one prescription for an antipsychotic medication. We limited the analyses to individuals not dually eligible for Medicaid and Medicare because we would be missing the majority of the outpatient and inpatient services of those who were dually eligible. Eligibility for Medicare involves having contributed to the Social Security system through employment. Thus, our study population of Medicaid recipients is likely to be less functioning than the population with schizophrenia as a whole. Data were analyzed at the person-year level, with individuals contributing up to 3 years of data.
Our analysis was based on prescription fills for oral antipsychotic medications. Individuals prescribed depot antipsychotics were excluded for several reasons. The pharmacokinetic profiles of depot antipsychotic medications are considerably different from those of oral medications. Further, users of depot medications are more likely to have been nonadherent in the past and are often heavy recidivist users of inpatient services.
Patients were assigned to one of the following oral medication groups: 1) typical antipsychotic, 2) clozapine, 3) another atypical antipsychotic, or 4) antipsychotic polypharmacy. We examined individually the atypical antipsychotics risperidone, olanzapine, and quetiapine but did not find significant differences in adherence among these agents and therefore determined that they would be most appropriately combined. For each year studied, a treatment designation of typical antipsychotic, clozapine, or other atypical antipsychotic was restricted to the medications of those who received typical antipsychotics or the above-mentioned atypical antipsychotics for the entire year. The antipsychotic polypharmacy designation was assigned to patients receiving concurrent prescriptions of two or more antipsychotics for more than 50% of the period in which they were eligible for Medi-Cal in that year. We excluded individuals in years when they were changing medications.
Adherence to prescribed regimens was determined by examining Medi-Cal claims by means of medication refill records
(14,
15). Adherence was measured by the annual cumulative possession ratio, which was computed for each person in each calendar year. The cumulative possession ratio was calculated by dividing the number of days medications were available for consumption by the number of days subjects were eligible for Medi-Cal
(14,
15). For example, a person eligible for the entire year but who received a total of 240 days’ supply of prescribed antipsychotic medication would have a cumulative possession ratio of 0.66.
As has been done in previous studies
(5,
10), we categorized a person-year’s adherence on an ordinal scale derived from the cumulative possession ratio using the following designations: nonadherent (ratio=0.00–0.49), partially adherent (ratio=0.50–0.79), adherent (ratio=0.80–1.10), and excess medication fillers (ratio >1.10). Excess filling of medications may occur for several reasons, including actual overuse and loss or theft of medications. We discuss potential causes and their consequences in more detail later in this article.
We used Medi-Cal claims to determine whether someone was hospitalized in a given year (indicated by a hospital claim), either in an acute psychiatric facility, a psychiatric ward of a community hospital, or a medical/surgical ward of an acute care hospital. Psychiatric claims are billed separately from medical/surgical claims, and each type is identifiable by provider classification codes and category of service codes. For hospitalized individuals, we calculated the total amount paid by Medi-Cal for inpatient care. For all subjects, we computed the amount paid for outpatient mental health and medical care, including physician services and other clinic care, laboratory and radiological services, and other noninpatient acute care; the amount paid for all pharmaceuticals; and the total amount paid by Medi-Cal for acute care. We have previously used this combined database to analyze costs by living situation
(16), but this is our first study using these data to examine adherence to antipsychotic medication.
Statistical Analysis
Logistic regression was used to estimate the probability of being adherent (as opposed to nonadherent, partially adherent, or an excess filler) as a function of age, gender, ethnicity, comorbid substance abuse, living situation, or type of antipsychotic medication. The resulting parameter estimates were used to provide estimates of adherence standardized to the underlying population characteristics. Logistic regression was similarly used to estimate the probability of acute psychiatric hospitalization and the probability of acute medical hospitalization and to provide estimates of hospitalization standardized to the underlying population characteristics.
Standard errors were estimated by using the nonparametric bootstrap method with 1,000 replications
(17). Data for the bootstrap analysis were sampled by the individual, rather than by observation, to account for potential individual-correlated errors.
A two-part model was used to estimate hospital costs associated with nonadherence
(18,
19). A logistic model estimated the probability of hospitalization (for either psychiatric or medical care), and a gamma model estimated hospital costs conditional on positive cost
(20). Pharmacy costs, outpatient costs, and total costs were estimated by using a gamma regression only, since all subjects had some positive costs in these areas. Standardized effects were calculated over both parts of the model; standard errors were estimated by using the nonparametric bootstrap
(17).
Results
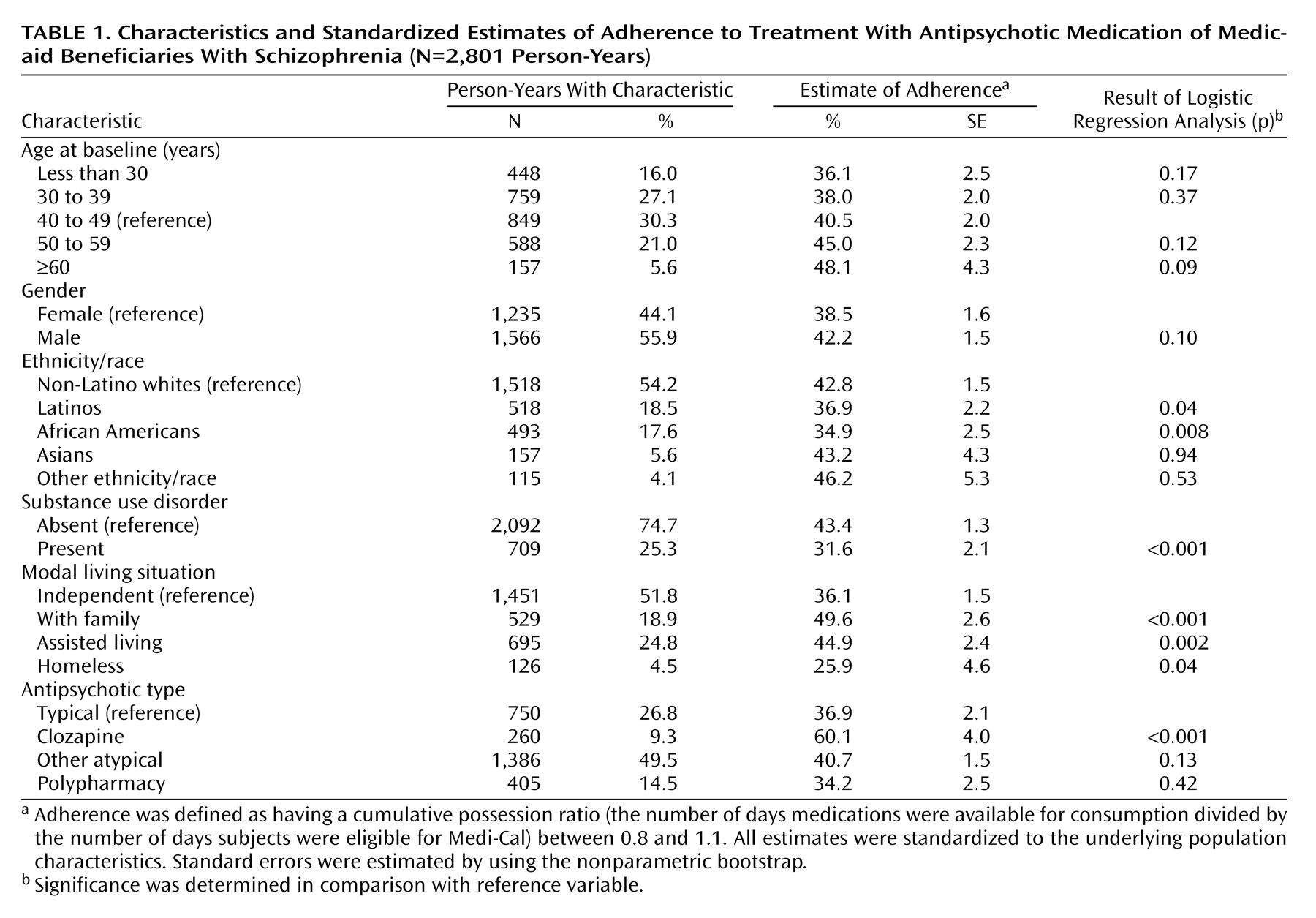
Table 1 provides descriptive statistics for our Medi-Cal beneficiaries with schizophrenia in San Diego County. We identified 1,619 individuals diagnosed with schizophrenia who were living in the community in 1998–2000. Merging this person-level information with 3 years of Medi-Cal antipsychotic pharmacy claims provided data for 5,084 person-years, of which 1,895 indicated changing of medications and 388 included prescriptions for depot medications. Our analysis sample of 2,801 person-years included 750 person-year records for typical antipsychotics, 260 for clozapine, 1,386 for other atypical antipsychotics, and 405 for antipsychotic polypharmacy. Based on our adherence designations, 24% of patients were considered nonadherent, 16% partially adherent, 19% were excess fillers, and 41% were adherent.
The mean age of the patients was 42 years (SD=11); the majority were between the ages of 30 and 59. Fifty-six percent were men, and the ethnic diversity of the sample approximated that of San Diego County’s general population
(9) (
Table 1). About one-quarter of the individuals were diagnosed with a comorbid substance use disorder. About one-half of the subjects lived independently, 25% resided in assisted living facilities, 19% lived with family members, and 5% were homeless.
Table 1 also shows the standardized probability of antipsychotic adherence for each potential risk factor. We found that the likelihood of adhering to an antipsychotic medication generally increased with age. African Americans and Latinos had a lower probability of being adherent than Caucasians. Substance abusers were less likely to be adherent than non-substance-abusers. Nonadherence had a high association to living situation: those living with family members or in assisted living facilities were more likely to be adherent than those living independently, whereas those who were homeless were less likely to be adherent. Individuals prescribed clozapine were more likely to be adherent than those prescribed typical antipsychotics. We did not find statistically significant differences in adherence between patients receiving typical antipsychotics and those receiving atypical antipsychotics other than clozapine and those receiving multiple drugs.
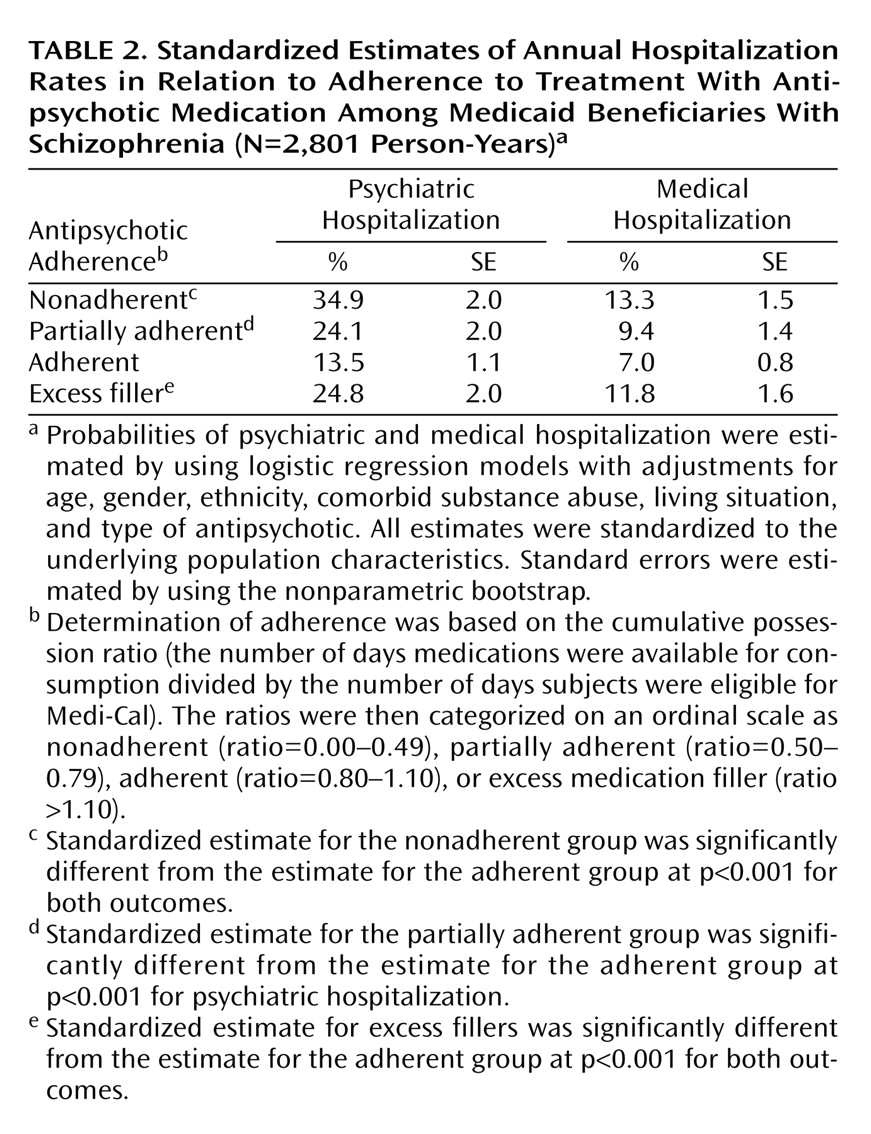
Table 2 shows the probability of psychiatric hospitalization and the probability of medical hospitalization by level of antipsychotic adherence with adjustments for age, gender, ethnicity, comorbid substance abuse, living situation, and type of antipsychotic. Psychiatric hospitalization was strongly related to the degree of adherence: individuals who were considered nonadherent were two and one-half times more likely to be hospitalized than those who were adherent. Those who were partially adherent or excess fillers were 80% more likely to be hospitalized than those who were adherent.
Hospitalization for medical conditions was related to antipsychotic adherence as well. Individuals who were nonadherent or excess fillers were about 70% more likely to be hospitalized for medical care, and those who were partially adherent were more than 30% more likely to be hospitalized than those who were adherent. The three most common nonpsychiatric inpatient diagnoses were pneumonia, heart disease, and chronic obstructive pulmonary disease.
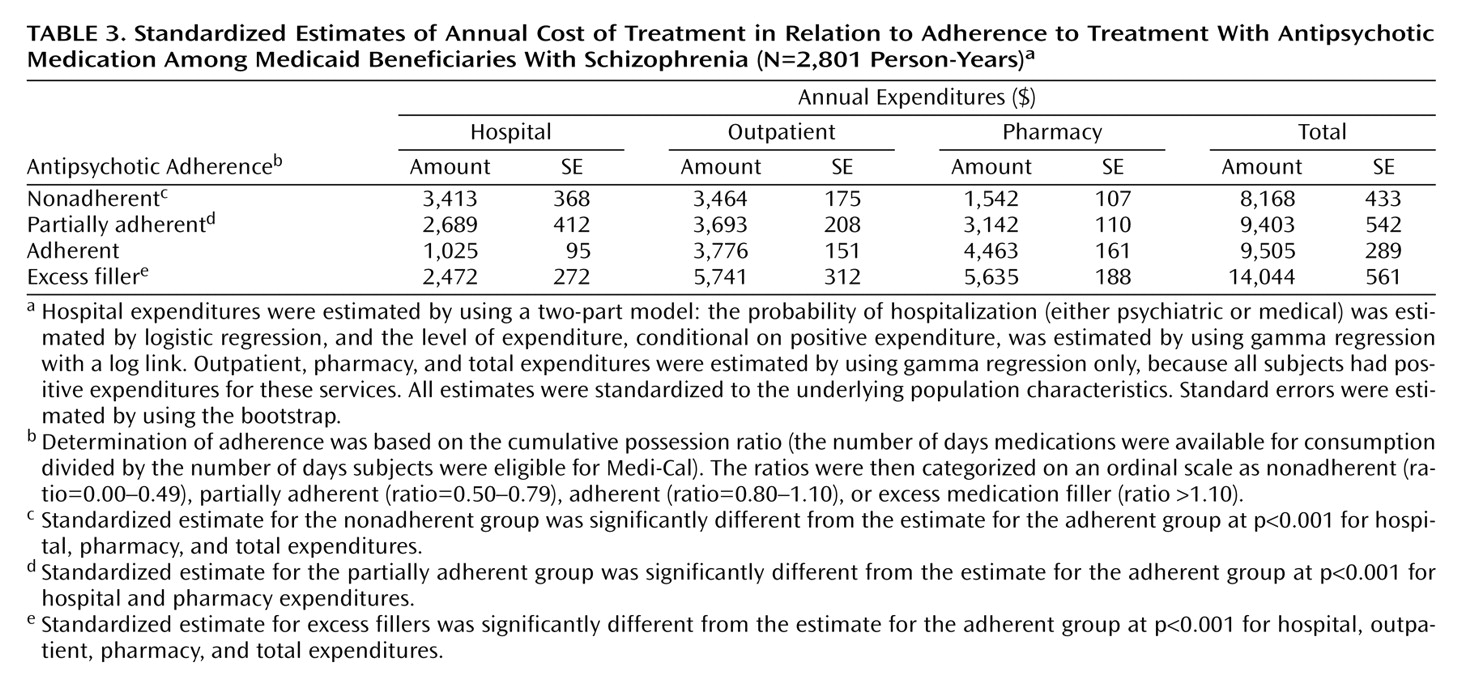
Table 3 shows standardized estimates of annual costs associated with adherence. Medi-Cal expenditures for hospitalizations were proportional to the probability of hospitalization: the hospital expenditures of those who were nonadherent were more than three times higher than the hospital expenditures of those who were adherent. The costs of those who were partially adherent or who had excess medication fills were about two and one-half times higher than the costs of those who were adherent. Outpatient expenditures were similar among those who were adherent, partially adherent, or nonadherent but were higher for those who had excess fills.
Pharmacy expenditures were greater for those more adherent to their medications and highest for those with excess fills. Overall, cost savings for avoided hospitalizations among those who were adherent partially offset the higher pharmacy costs associated with adherence: total costs for those who were adherent were about $1,300 higher over a year than the costs for those who were nonadherent and were about equal to the costs of those who were partially adherent. Total expenditures for subjects who were adherent were more than $4,000 less than for those with excess fills.
We conducted a post hoc analysis of predictors of excess filling of antipsychotic medication using logistic regression and the methods described above. We found that African Americans were less likely than non-Latino whites to be excess fillers of medications (15.2% versus 20.6%) (p=0.004) and that individuals in assisted living facilities were more likely than those living independently to be excess fillers (29.0% versus 15.6%) (p<0.001). Receiving multiple antipsychotic medications was strongly related to the probability of being an excess filler of medication: 54.4% of those receiving multiple medications versus 12.5% of those receiving a single typical medication were excess fillers (p<0.001).
Discussion
Despite the widespread use of atypical antipsychotics, we found a low rate of adherence to treatment with antipsychotic medication in a sample of young and middle-aged adult Medi-Cal beneficiaries with schizophrenia in San Diego County. Overall, we found 40% of patients with schizophrenia to be nonadherent or partially adherent to their antipsychotic treatment (i.e., a cumulative possession ratio <0.80). An additional 19% of the patients were excess medication fillers (i.e., cumulative possession ratio >1.10). Although rates of nonadherence vary depending on the definition used, our estimates of nonadherence are similar to the nonadherence rate of 50% reported in several reviews and research papers
(1–
3,
21). Our strict definition of adherence (cumulative possession ratio of 0.8–1.1) might have led to underestimated adherence rates, and the selection criteria we used (continuous enrollment, individuals not changing medications) would tend to lead to overestimates of adherence rates.
We found that the adherence rates of individuals treated with the atypical antipsychotics risperidone, olanzapine, and quetiapine were similar to those of patients treated with conventional antipsychotic medication. Results from previous research have been mixed regarding differences in adherence between typical and atypical antipsychotics
(5,
21–26). Rosenheck et al.
(23) found that patients taking clozapine had greater medication adherence than those taking haloperidol because of greater symptom improvement and fewer side effects. Dolder et al.
(21) reported that patients treated at the San Diego Veterans Affairs Medical Center who were taking atypical antipsychotics were more likely to be adherent than those taking typical antipsychotics, but this finding was sensitive to the exact definition of adherence. Three meta-analyses
(27–
29) reached different conclusions regarding the comparative efficacy and side effect profile of atypical and conventional antipsychotics. Geddes et al.
(27) found no clear evidence that atypical antipsychotics were more efficacious or better tolerated than conventional antipsychotics. Davis et al.
(28) reported that some, but not all, atypical antipsychotics were more efficacious than conventional antipsychotics. Leucht et al.
(29) found that atypical antipsychotics were moderately more efficacious than low-dose conventional antipsychotic medications but that only clozapine had significantly fewer extrapyramidal symptoms. Our finding of a lack of a significant difference in the adherence rates between conventional neuroleptics and atypical antipsychotics (other than clozapine) points to a need for continued research on improving adherence in patients with schizophrenia.
We found that individuals living with family members or in an assisted living facility were more likely to be adherent than those who lived independently. This might result from greater medication supervision and support of medication-taking behavior by family members or staff at assisted living facilities or from greater access to outpatient services. Alternatively, it may be that characteristics of the patients themselves, rather than their living situations, determine rates of adherence. Patients who live with family members or in assisted living facilities are different in ways we have not measured from those who live independently and those who are homeless, and it may be that these personal characteristics related to selection of living situation are driving our results. For example, individuals living with a family member may have higher functioning than those in other living situations, and functioning may be a determinant (rather than an outcome) of adherence. However, to the extent that residents of assisted living facilities are sicker than individuals living independently, one would expect their rate of adherence to be lower.
Individuals who were homeless had the lowest probability of being adherent. They were also the least likely to receive medication supervision, to have the support of family members, and to have access to outpatient care. Studies of interventions aimed at reducing homelessness
(22,
23,
30–33) have found that homeless individuals assigned to community housing, group homes, and residences providing a higher level of services were more likely to remain stably housed than homeless individuals attempting to live independently. To the extent that assisted living facilities provide a residence with improved medication oversight, they could be viewed as a preferred alternative to homelessness. Policy makers interested in reducing homelessness might consider subsidizing these facilities for certain subgroups of homeless individuals and evaluating whether these subsidies improve long-term residential and treatment outcomes.
Individuals noted to have a substance abuse disorder were significantly less likely to be adherent to their antipsychotic medication than those without a documented substance abuse disorder. This finding is consistent with previous research examining substance abuse and antipsychotic adherence
(22,
23,
33–35).
Unlike a number of previous investigations
(1,
2,
7), we found significant associations between adherence to treatment with antipsychotic medication and age and ethnicity. Investigators examining the course of schizophrenia
(23,
36–38) have observed that positive symptoms show a modest improvement over time, and it may be that adherence improves along with a decline in severe psychotic symptoms. It is also possible that younger people with schizophrenia, presumably with a shorter duration of illness than older individuals, may not have had sufficient time to appreciate the consequences of nonadherence.
We found that Latinos and African Americans were significantly less likely to be adherent than Caucasians. Valenstein et al.
(5) reported that African Americans were significantly less likely to be adherent to their antipsychotic medication, but the low rate of adherence among Latinos is a new finding. Adherence of any particular ethnic group is likely to be affected by a unique combination of factors. Psychosocial and other nonbiological factors such as cultural beliefs and expectations, as well as access to care, may play an important role in determining adherence. In addition, there are likely to be biologically determined ethnic differences in therapeutic response to and adverse effects with antipsychotic medications. For example, tardive dyskinesia has been reported to be more common in African American patients than in Caucasians
(39,
40). Pharmacogenetic differences in the rate of metabolism of antipsychotic medications and in the response to antipsychotic medications have also been reported
(41,
42). To what extent such ethnic differences result in variations in adherence remains to be studied.
With respect to psychiatric hospitalization, we found that patients who were partially adherent to their antipsychotic medication were two and one-half times more likely to be hospitalized and that patients who were nonadherent were three times more likely to be hospitalized than patients who were adherent. Excess fillers of antipsychotic medication (i.e., cumulative possession ratio >1.10) were two times more likely to be hospitalized. A few previous investigations have reported similar findings
(4,
5,
10,
22,
43,
44), including the association between excess amounts of antipsychotic medication and a greater likelihood of being hospitalized. Excess medication fills might have resulted from overuse of antipsychotics, increasing the risk of medication side effects and associated medical care. Alternatively, excess filling of medication may be indicative of other problems, such as having an unsatisfactory response to antipsychotics requiring numerous medication changes, or being in a situation in which medications are often lost, stolen, or sold. The strongest predictor of excess filling of antipsychotic medication was filling prescriptions for multiple antipsychotics. This suggests that therapeutic complexity is an important factor related to excess fills. Although the current study does not prove a causal relationship between nonadherence or excess fills and hospitalization, it adds more evidence to the notion that antipsychotic nonadherence is an important factor leading some individuals to be hospitalized and that excess fills are deserving of additional study and perhaps intervention.
With respect to medical hospitalization, we found that individuals who were nonadherent, partially adherent, or excess fillers were more likely to be hospitalized. There is a growing body of literature suggesting that individuals with schizophrenia receive worse physical health care and experience poorer outcomes than individuals with depression or those without mental illness
(45,
46). Patients who are nonadherent to their antipsychotic treatment are likely to be more symptomatic and, presumably, less able to comply with outpatient treatment for other medical illnesses. As a result, they may be more likely to experience exacerbations of illness requiring hospitalization. The nature of some of the most common nonpsychiatric inpatient diagnoses in the current study (e.g., pneumonia, heart failure, chronic obstructive pulmonary disease), suggests that the association between adherence and medical hospitalization might result from behaviors influencing both adherence and physical health.
As expected, hospital costs were lower and pharmacy costs were higher for those who were adherent to their antipsychotic medications than for those who were nonadherent. Overall, improving medication adherence has the potential to improve health for individuals with schizophrenia without seriously increasing costs. Thus, interventions that efficiently improve medication adherence are likely to be cost-effective. In contrast, excess fillers had higher pharmacy, hospital, outpatient, and total costs. Targeting excess medication fills has the potential to save more than $1,000 per person per year in medication costs alone. These findings suggest additional research into the causes and clinical consequences of excessive provision of antipsychotic medication.
Our study has a number of strengths and limitations. We were able to examine antipsychotic adherence and hospitalization in a large, diverse sample of individuals. Although our data had limited clinical measures, Adult Mental Health Services data provided additional demographic information, including ethnicity and living situation. We used medication refill records from claims data to assess adherence. Although refill records are limited by their inability to directly monitor medication administration, they represent an objective and unobtrusive measure of adherence
(14,
15). The threshold for adherence (i.e., cumulative possession ratio of at least 0.80) was high, but this threshold is supported by findings of substantial differences in hospitalization among patients classified as nonadherent, partially adherent, and adherent.
Poor adherence, poor family support, poor social integration, and homelessness can be and likely are linked as one direct effect of schizophrenic pathology. Provision of a better medical and psychiatric safety net is highly desirable for nonadherent patients, but such supervision is already part of the case management system for chronically mentally ill patients, and subsidized housing is already a part of publicly available care for the mentally ill. Our findings argue for new approaches to improve the effectiveness of health services delivered to the mentally ill through the existing network of agencies and providers. They also suggest targeting subgroups for specific improvement strategies to protect high-risk patients with schizophrenia.