Debates about the categorical validity of schizophrenia, schizoaffective disorder, and affective disorder are a consequence of the clinical similarities between these illnesses
(1–
4). For instance, 65% of bipolar disorder patients have hallucinations or delusions
(5), and symptoms of psychosis and thought disorder can be persistent
(6,
7). First-rank symptoms, considered pathognomonic for schizophrenia, occur in 23% of patients with psychotic bipolar illness
(8). Some studies
(5,
9,
10), but not all
(11), have found that patients with psychotic bipolar illness have poorer outcomes than their nonpsychotic peers and better outcomes than patients with schizophrenia
(12,
13).
A subgroup of bipolar disorder patients who also suffer from psychosis may have shared genetic susceptibility with schizophrenia patients. Although the New York High-Risk Project demonstrated that schizophrenia occurred only in the high-risk offspring of parents with schizophrenia and not of those with affective disorder
(14), other studies have found that subjects with schizophrenia have affectively ill family members
(15) and that patients with bipolar illness have family members with psychosis
(16). Chromosomes 3, 6, 10, 13, 15, 18, and 22
(17–
21) have loci that are associated with risk for both schizophrenia and affective illness. However, chromosome 8 is associated only with risk for schizophrenia, while loci associated only with risk for bipolar illness have been identified at 12q24, 21q21, and 4p16 (reviewed in reference
18).
Studies of information processing demonstrate both similarities and differences between these two illnesses. Impaired performance has been demonstrated in both illnesses for span of apprehension
(22), P300 evoked response latency
(23) and amplitude
(24), P50 auditory evoked response suppression
(25–
27), and prepulse inhibition
(28). Differences have been demonstrated with the P300 evoked response topography
(24) and amplitude
(23), facial scanpath patterns
(29), a mismatch negativity paradigm
(30), and the relationship between a left temporal P300 abnormality and left posterior superior temporal gyrus volume
(31). It is unclear to what extent the similarities are due to a common underlying pathophysiology or to the nonspecific effect of acute symptoms in psychosis.
Physiological phenotypes may help to identify any common pathophysiology. An abnormality in the suppression of the P50 auditory evoked potential response has been used as a phenotype in genetic studies of schizophrenia
(32). The suppression of the response to the second of two auditory stimuli is a measure of the ability of the brain to “gate,” or tune out, irrelevant stimuli by utilizing inhibitory pathways
(33). Patients with schizophrenia
(33,
34) and many of their unaffected relatives
(35) have abnormally low levels of P50 suppression. This abnormality has been linked to the chromosome 15q14 locus of the alpha 7-nicotinic acetylcholine receptor gene in families with schizophrenia
(32).
In bipolar disorder subjects, diminished P50 suppression has been associated with severity of clinical symptoms
(25) and elevated catecholamine levels
(26,
27) in a state-dependent manner. Previous studies have not addressed whether diminished P50 suppression in bipolar disorder patients who are or have been psychotic might also be a sign of a psychophysiologic mechanism common with schizophrenia. Therefore, this study compared P50 suppression in an outpatient population with diagnoses of schizophrenia, schizoaffective disorder–bipolar type, and bipolar illness as well as healthy comparison subjects. We hypothesized that subjects with a lifetime history of psychosis, regardless of current symptom severity, would have diminished P50 auditory evoked potential suppression. Additionally, we hypothesized that in the absence of severe symptoms, the subjects without a history of psychosis would demonstrate adequate P50 suppression.
Method
Subjects
Sixty-four patients with a history of at least one episode of mania were recruited from the Colorado Psychiatric Hospital outpatient program and depressive/manic depressive support groups in the Denver metropolitan area. Subjects received a complete description of the study and then gave their written informed consent. The Structured Clinical Interview for DSM-IV
(36) and a detailed life chart determined diagnosis. Medical records were reviewed when it was unclear whether the subject had suffered from psychotic or affective symptoms in the absence of alcohol abuse, drug abuse, or medical illness. Twenty-two subjects received a diagnosis of schizoaffective disorder, and 42 subjects received a diagnosis of bipolar disorder. A lifetime history of at least one psychotic episode determined whether the bipolar subjects had a history of psychosis. The Beck Depression Inventory
(37), the Young Mania Rating Scale
(38), and the Positive and Negative Syndrome Scale
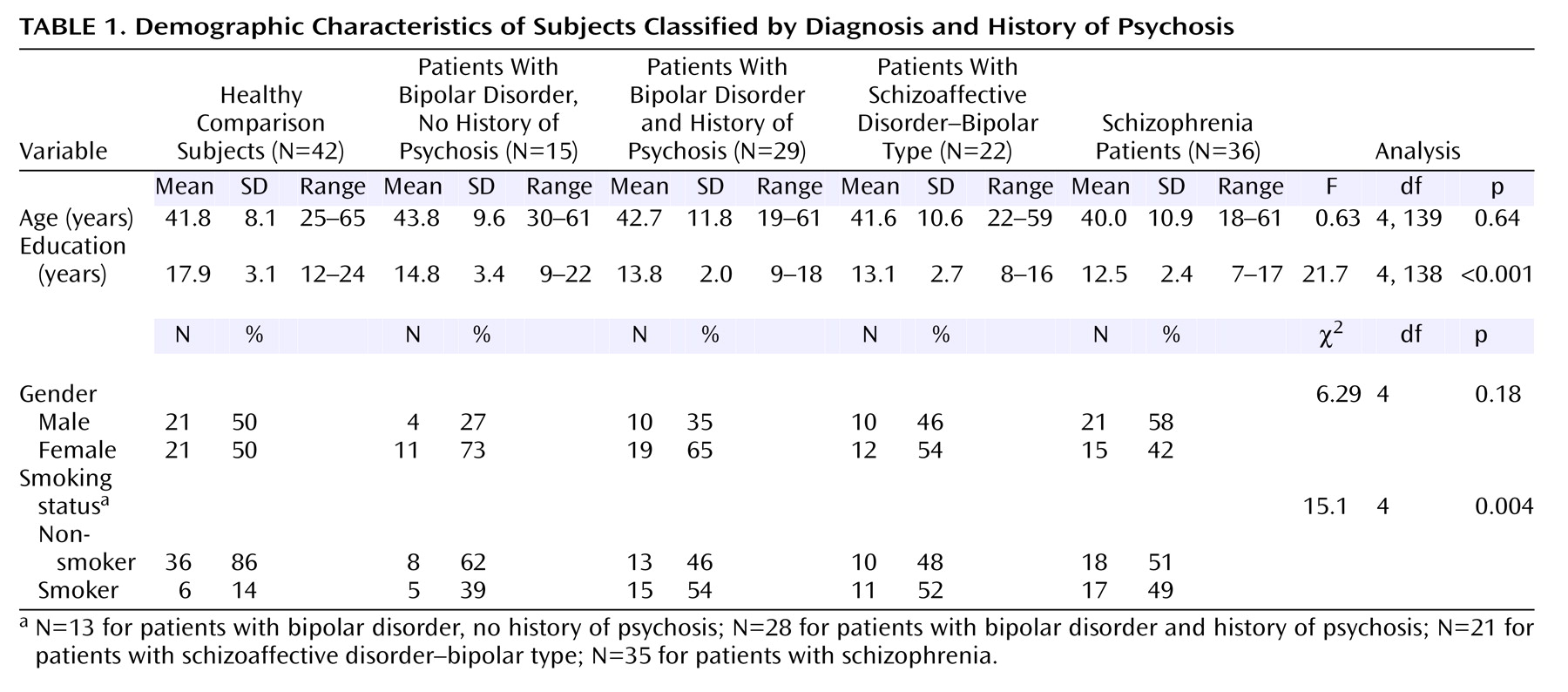
(39) assessed the level of severity of current illness. Subject groups did not differ in age or gender. Level of education differed between groups (
Table 1). Post hoc pairwise comparisons showed that the healthy comparison subjects had more years of education than subjects with bipolar disorder and no history of psychosis (p=0.004), bipolar disorder subjects with a history of psychosis (p<0.001), subjects with schizoaffective disorder–bipolar type (p<0.001), and subjects with schizophrenia (p<0.001). Rates of smoking also differed between groups (
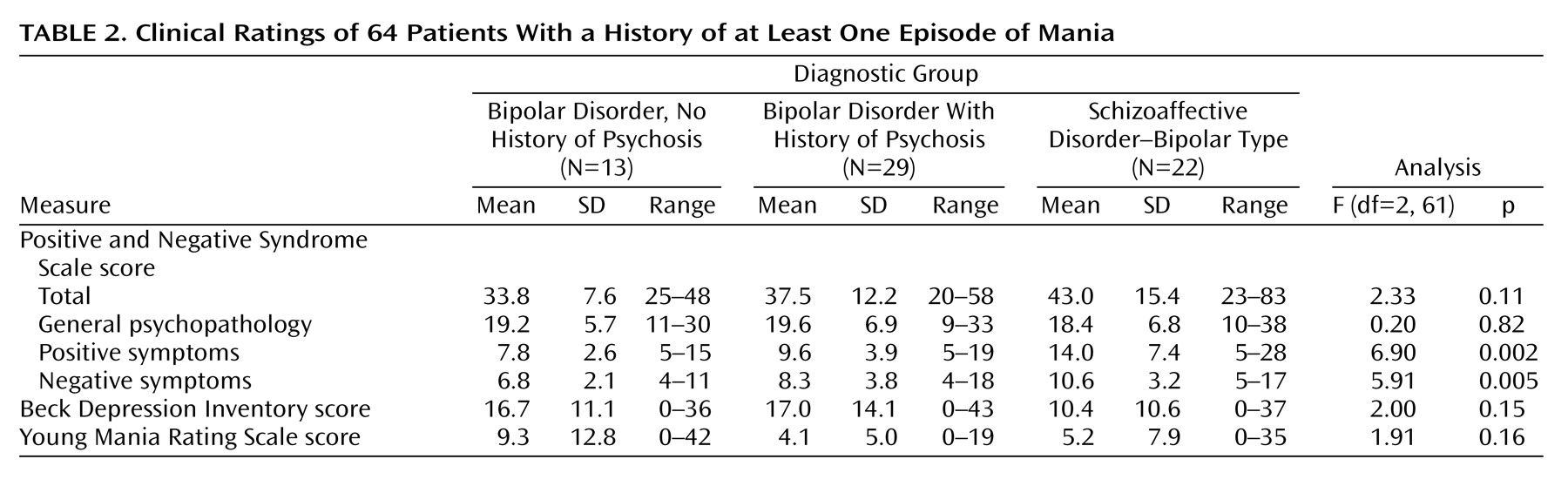
Table 1), with affected subjects smoking more than healthy subjects. Level of negative and positive symptoms differed between groups (
Table 2). In post hoc analyses, subjects with schizoaffective disorder had more negative symptoms (p=0.005) and positive symptoms (p=0.002) than the subjects with bipolar disorder. Groups did not differ on any other clinical measures (
Table 2). Subject groups did not differ in terms of age at illness onset or illness duration. Two additional patients with bipolar illness had only demographic and P50 recording information available. Groups were compared with previously collected data on 36 subjects with schizophrenia and 42 healthy comparison subjects, for whom only demographic and P50 recording data were available.
Electrophysiological Recordings
Recordings were obtained between 10:00 a.m. and 12:00 p.m. while subjects were in a supine position and staring at a fixed target to maintain alertness. Recordings were obtained from subjects at least 30 minutes after their last cigarette, since nicotine has been shown to enhance P50 suppression in subjects with schizophrenia
(40). A gold disk electrode affixed to the vertex (Cz) and referenced to the ears recorded electroencephalographic activity. Electroencephalogram (EEG) activity was amplified 20,000 times with bandpass filters (–50%) between 1 and 300 Hz. Electrodes at the right superior orbit and lateral canthus recorded electro-oculogram (EOG) activity. An operator blind to the subject’s diagnosis collected EEG and EOG data for 1000 msec for each paired stimulus presented. The operator rejected trials during online recording if they contained large muscle artifact or eye blinks, as indicated by an EEG or EOG voltage of ±50 μV over the area of the P50 wave. A conditioning-testing paradigm presented auditory stimuli with an intrapair interval of 0.5 seconds and interstimulus interval of 10 seconds. A 0.04-msec duration square wave pulse was amplified in the 20–12,000 Hz bandwidth and delivered through earphones that produced a 2.5-msec sound with a mean intensity of a 70-db sound pressure level, as measured at the subject’s ear by a sound meter
(41). If the subjects showed a startle response, the operator reduced the intensity by 2 dB. The operator increased the intensity by 2 dB if the subjects had a P50 test wave amplitude of less than 1.0 μV. At least five average evoked potential recordings were collected for each subject, each containing at least 16 trials. A high-pass filter (10 Hz) and a seven point, low-pass filter (300 Hz; A=0.95)
(42) digitally filtered each recording. The grand average used for analysis excluded averaged recordings with no discernible conditioning P50 waves or with prominent EOG activity at the same latency as the P50. Six subjects (three bipolar disorder subjects with no history of psychosis, two bipolar subjects with a history of psychosis, and one schizoaffective disorder subject) had only one usable trial due to artifact. There were no differences in the number of trials used for each grand average between the groups (F=1.0, df=2, 60, p<0.37). A previously described computer algorithm
(42,
43) was used to identify and quantify the P50 wave. The computer selected the most positive peak between 40 and 75 msec after the conditioning stimulus. The test P50 wave was the most positive waveform, ±10 msec of the latency of the conditioning P50 wave. This criterion represents the 95% confidence limit of the difference between conditioning and test latencies
(43). A rater blind to subject diagnoses also reviewed tracings. Thus, any possible P50 occurring in the test response was not overlooked. The amplitude of each wave was measured relative to the previous negativity. P50 suppression was calculated by the equation 100 × (1–[test wave amplitude/conditioning wave amplitude]).
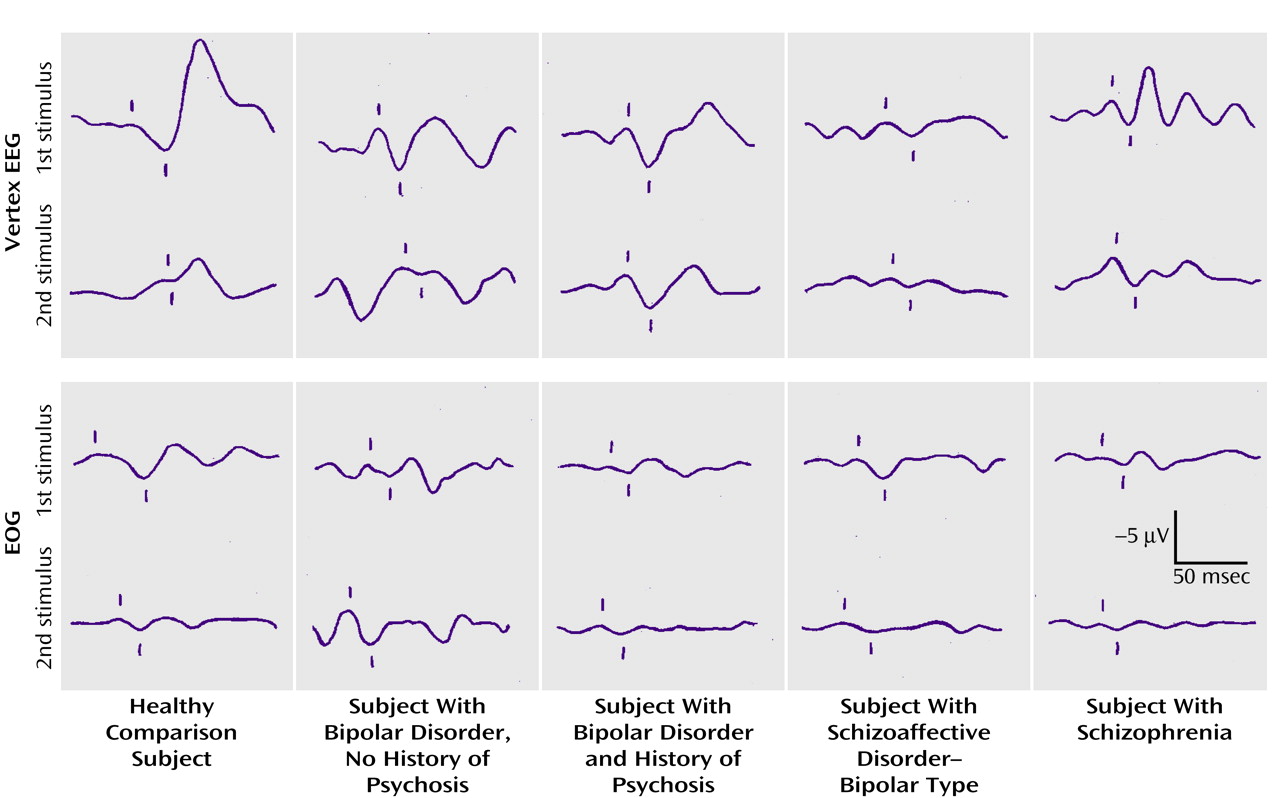
Figure 1 demonstrates representative examples of the recordings for the diagnostic groups.
Statistical Analysis
To determine if a lifetime history of psychosis affected the auditory event-related wave, a nonparametric Kruskal-Wallis one-way analysis of variance (ANOVA) with post hoc analysis to correct for multiple comparisons
(44) assessed overall effects among the five groups. Conditioning amplitude, test amplitude, P50 suppression, and conditioning latency were examined as dependent variables, with diagnostic group as the independent variable. A Pearson correlation between P50 suppression and scores on the Young Mania Rating Scale, Beck Depression Inventory, and Positive and Negative Syndrome Scale assessed whether there was a relationship between the level of current psychopathology and P50 suppression. An ANOVA for the continuous variables and chi-square test of association for categorical variables were used to test for potential differences between groups with respect to demographic variables. Two-tailed Student’s t tests were used for individual comparisons between groups for continuous variables. Finally, demographic variables for which the groups differed were tested for their effect on the P50 suppression percentage with Pearson correlation or an ANOVA.
Results
A lifetime history of psychosis was associated with decreased suppression of the P50 test stimulus response, regardless of diagnosis (
Figure 2). One-way ANOVA revealed significant group differences in mean P50 suppression (F=15.7, df=4, 139, p<0.001). Post hoc analysis showed the P50 suppression of subjects with schizophrenia (mean=22.3, SD=49.9) was significantly lower than the P50 suppression of healthy subjects (mean=87.1, SD=12.9) (p<0.001). The subjects with schizophrenia also had significantly lower P50 suppression than the subjects with bipolar illness and no history of psychosis (mean=71.2, SD=41.1) (p<0.001) and the bipolar disorder subjects with a history of psychosis (mean=57.8, SD=38.2) (p<0.02). Relative to healthy comparison subjects, bipolar disorder subjects with a lifetime history of psychosis also had decreased P50 suppression (p=0.002), as did those with schizoaffective disorder–bipolar type (mean=52.5, SD=38.5) (p<0.001). The subjects with bipolar illness and no history of psychosis exhibited P50 suppression that was not different from normal subjects (p<0.88).
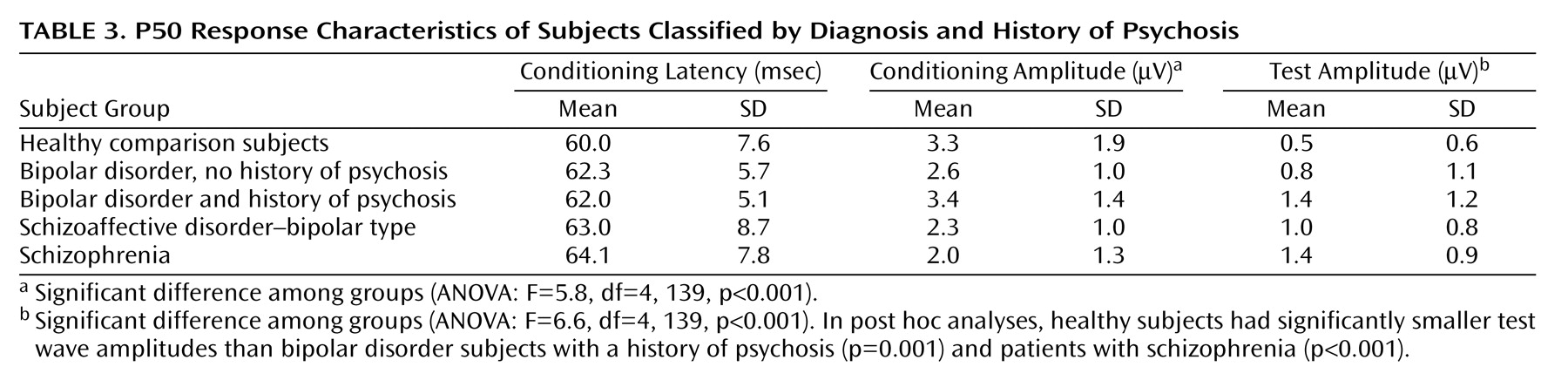
The conditioning wave latency did not differ among groups (F=1.4, df=4, 142, p<0.23) (
Table 3). The subjects with schizophrenia and schizoaffective disorder had the smallest mean conditioning wave amplitudes, and an ANOVA revealed significant group differences. In the post hoc analyses, subjects with schizophrenia had significantly smaller conditioning wave amplitudes than the healthy comparison subjects (p<0.001) and the bipolar subjects with a history of psychosis (p<0.001).
Several clinical variables were measured on the day of testing to ascertain their possible contribution to diminished P50 suppression. No correlations were seen between P50 suppression and scores on the Positive and Negative Syndrome Scale (total: r=–0.01, p=0.94; positive symptoms: r=–0.07, p=0.61; negative symptoms: r=0.10, p=0.43; general psychopathology: r=–0.02, p=0.90) or on the Young Mania Rating Scale score (r=0.11, p=0.39) or Beck Depression Inventory (r=–0.04, p=0.75).
Subjects who reported smoking on a daily basis did not have significantly different P50 suppression (mean=51.6, SD=42.2) than did subjects who described either never having smoked or having been a former smoker (mean=61.1, SD=45.3) (t=–1.23, df=138, p=0.22). For subjects with a lifetime history of psychosis, the difference in P50 suppression between those taking an atypical antipsychotic medication (48.9%) and those not taking an atypical antipsychotic medication (38.5%) was not significant (t=–1.53, df=85, p<0.14). No significant effects on P50 suppression were present for bipolar disorder subjects if they were being treated with an antidepressant (t=–0.86, df=62, p<0.40) or a mood stabilizer (t=0.16, df=62, p<0.88).
Discussion
Patients with bipolar illness and a history of psychosis, as well as those with schizoaffective disorder–bipolar type and schizophrenia, had impaired levels of P50 suppression, whereas patients with nonpsychotic bipolar illness exhibited P50 suppression similar to people without psychiatric illness. The severity of the diminished P50 suppression in the bipolar disorder subjects with a history of psychosis was intermediate between the subjects with schizophrenia and the healthy comparison subjects. Two of the 13 subjects in the nonpsychotic bipolar illness group exhibited P50 suppression less than two standard deviations from their group mean. These subjects may have a vulnerability to psychosis that had not yet manifested itself. For instance, over a period of 10 years, 17.6% of nonpsychotic bipolar disorder subjects eventually develop psychosis
(5). Another explanation is that the interview did not reveal psychotic symptoms. Twenty-two percent of subjects who deny any history of psychosis during two separate interviews are later found to have evidence of psychotic illness
(10). Finally, the limited number of subjects in the nonpsychotic group may have contributed to a type II error. It may be noteworthy that nonpsychotic subjects were relatively infrequent in our bipolar clinical population.
Smoking normalizes P50 suppression in people with schizophrenia
(40), and the number of cigarettes smoked per day has been correlated with levels of alpha-7 nicotinic receptors in postmortem hippocampus and cortex
(45). Acute effects of smoking were controlled for in this study by having all subjects abstain from smoking for at least 30 minutes prior to testing. Smoking rates were elevated in this study population, similar to previous findings
(46,
47). Smokers exhibited nonsignificantly lower levels of P50 suppression. This finding is not unexpected, since no clear relationship between smoking history and P50 suppression in schizophrenia subjects has been established.
Previous work has not shown severity of psychosis in subjects with schizophrenia to be correlated with P50 suppression
(27). The present study did not find any correlation between the current level of manic, depressed, or psychotic symptoms and P50 suppression in the bipolar and schizoaffective subjects. Thus, these results differ from previous studies that had established a positive correlation between acute symptoms and P50 suppression
(25,
26,
48). However, the present study is in agreement with one study that did not find an association between clinical symptoms in mania and P50 suppression
(27). These discrepancies may be due to the variability in acute pathology in these outpatient groups when compared with the extremely ill inpatient groups in which the correlation was first demonstrated
(25). Furthermore, although P50 suppression was previously reported to have normalized with clinical improvement in acute mania (from –41% to 59%), the improved levels of suppression were still less than the levels of healthy subjects (81%)
(26). These acutely ill subjects may have had both trait and state effects on P50 suppression.
This finding is similar to findings that inpatients with schizophrenia have stable Continuous Performance Test impairment from admission to discharge, whereas inpatients with bipolar illness have normalizing Continuous Performance Test performance from admission to discharge. At discharge, however, their performance is still impaired relative to healthy comparison subjects
(49). These results are also consistent with a model proposed by Nuechterlein et al.
(50) defining measures of impairment as stable vulnerability indicators, mediating vulnerability indicators, or episode indicators. The diminished P50 suppression within the bipolar disorder subjects with a history of psychosis appears to represent a mediating vulnerability indicator, since it has both trait- and state-like components. Thus, diminished P50 auditory evoked potential suppression in this study may be related to a common physiological feature in bipolar illness with a history of psychosis and schizophrenia, although the severity of this P50 suppression abnormality is greater in schizophrenia.