While signs and symptoms remain the defining characteristics of psychiatric nosology, there is increasing consensus that the scope of assessment should include broader dimensions, such as functioning and quality of life. This has led to the increasingly frequent axiom that successful treatment must go beyond ameliorating signs and symptoms to address the broader issue of restoration of health. The 1948 World Health Organization definition of health as “a state of complete physical, mental, and social well-being and not merely the absence of disease” has resurfaced as an important touchstone for the evaluation of both mental and physical health treatment outcomes
(1). Thus, the thoughtful assessment of quality of life for psychiatric patients and the impact of our treatment interventions on quality of life are emerging as important issues for the field of psychiatry
(2,
3).
Quality of life has been defined in a number of ways, and many measures exist for assessing the construct
(4). Most definitions explicitly state that the assessment of quality of life should take into account patients’ subjective views of their life circumstances
(5). This includes perceptions of social relationships; physical health; functioning in daily activities and work; economic status; and an overall sense of well-being
(6). While measures of functioning focus on objective, quantifiable impairments that exist, measures of quality of life assess enjoyment and life satisfaction associated with various activities.
Evidence is accumulating that anxiety and affective disorders are associated with substantial impairments in quality of life and functioning. Individuals with major depressive disorder
(7), obsessive-compulsive disorder (OCD)
(8,
9), panic disorder
(10–
13), and social anxiety disorder
(14,
15) have substantially poorer quality of life than community comparison cohorts. In many cases, the quality-of-life impairments associated with these anxiety disorders are equal to or greater than those seen with other chronic medical disorders
(9,
16,
17).
What factors are associated with relatively better or worse quality of life for people suffering from mood and anxiety disorders? For patients with panic attacks, significant clinical correlates of quality of life include psychiatric comorbidity
(21), worry
(21), chest pain severity
(21), lack of social support
(10,
21), education
(12), and disability
(22). For patients with posttraumatic stress disorder (PTSD), the presence of comorbid medical disorders has been shown to significantly predict quality-of-life impairment
(23–
25). Understanding the relationship between quality-of-life dysfunction and specific clinical features of different anxiety and affective disorders may suggest new directions to improve treatment interventions and may facilitate more appropriate allocation of scarce health care resources. Thus, there is a need to examine the relative contribution of illness-specific factors (severity of symptoms, psychiatric comorbidity, and duration of illness) and demographic factors on quality of life across anxiety and affective disorders.
This study examines quality-of-life impairment in research subjects with one of eight anxiety or affective disorders with a common instrument relative to community normative data. The degree of quality-of-life impairment across these disorders will be examined as well as the relative contribution of illness-specific symptom severity, the presence of psychiatric comorbidity, the duration of illness, and demographic features to the prediction of quality-of-life dysfunction.
Method
Data for this analysis were drawn from 11 multicenter trials investigating the efficacy of sertraline treatment for anxiety or affective disorders. The sample included subjects with major depressive disorder
(26), chronic/double depression
(27), panic disorder
(28), PTSD
(29), premenstrual dysphoric disorder
(30,
31), OCD
(32), dysthymia
(33), and social phobia
(34). For premenstrual dysphoric disorder, panic disorder, and chronic/double depression, the data from the two available studies for each disorder were combined since the designs were identical.
In addition to the samples of patients entering clinical trials, data from a nonpsychiatric community sample (N=67) were used for establishing norms for the Quality of Life Enjoyment and Satisfaction Questionnaire
(35). These subjects had responded to notices seeking volunteers to serve as comparison subjects at the New York State Psychiatric Institute and Columbia University.
The ethics committees of the participating sites in these studies approved the protocols, and the studies were all conducted according to the guidelines of the Declaration of Helsinki and its amendments. All subjects read about the study, had the opportunity to ask questions, and gave written informed consent to participate in the research studies.
Subjects
Subjects from the clinical trial samples were men and women ages 18 or older (
Table 1). For the studies of chronic/double depression and dysthymia, the subjects were men and women 21–65 years and older
(27,
33). The studies of premenstrual dysphoric disorder included women ages 24–45
(30,
31). Women of child-bearing potential employed medically accepted birth control methods. Subjects with bipolar disorder, schizophrenia or other psychosis, alcohol or substance abuse or dependence, severe personality disorders, or the presence of significant suicide risk were excluded from participation. Subjects were further excluded if they demonstrated any clinically significant or unstable medical condition or had any condition that could significantly alter the pharmacokinetics of sertraline. (Refer to previously published studies [
26–
34] for additional details.)
The community sample was composed of people who had responded to advertisements seeking volunteers to serve as comparison subjects for studies conducted at the School of Medicine at Columbia University. They were screened to rule out clinically significant current mental or medical illnesses. A potentially available pool of subjects was maintained and contacted when a new study was funded and community comparison subjects were needed. We mailed them the Quality of Life Enjoyment and Satisfaction Questionnaire with a cover letter that included the informed consent form, and they completed it and returned it to one of us (J.E.). The subjects were then mailed a second form with another cover letter. The sample size was determined by the money available for the initial developmental study. The subjects were paid for completing the forms. We had 100% participation.
Quality-of-Life Assessment
The short form of the Quality of Life Enjoyment and Satisfaction Questionnaire
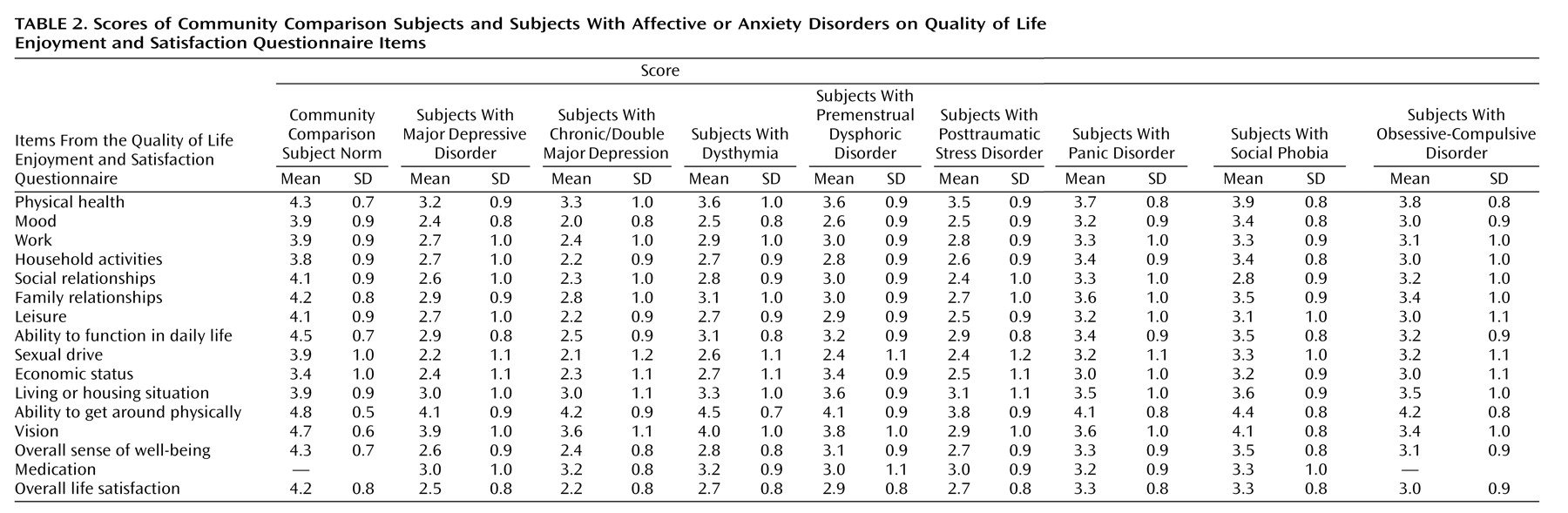
(35) was completed by the subjects before treatment in every study. The Quality of Life Enjoyment and Satisfaction Questionnaire is a self-report form composed of 16 items each rated on a 5-point scale that indicates the degree of enjoyment or satisfaction experienced during the past week. A total score of items 1 to 14 is computed and expressed as a percentage of the maximum possible score of 70. The 14 items evaluated each subjects’ satisfaction with his or her physical health; social relations; ability to function in daily life; ability to get around physically; mood; family relations; sexual drive and interest; ability to work on hobbies, work, leisure time activities; economic status; household activities; living/housing situation; and overall sense of well-being. There are two global items, numbers 15 and 16, that are not included in the Quality of Life Enjoyment and Satisfaction Questionnaire’s total score: medication and life satisfaction and contentment over the last week. In the community sample, the short-term (1 to 2 weeks) test-retest reliability (intraclass correlation coefficient) of the Quality of Life Enjoyment and Satisfaction Questionnaire’s 14-item total score was 0.86, and the internal consistency (Cronbach’s alpha) was 0.90. The test-retest consistency for the overall rating of life satisfaction and contentment was 0.71. Any subject scoring within 10% of the mean of the community sample was considered in the normal range. Severe impairment was operationally defined as Quality of Life Enjoyment and Satisfaction Questionnaire scores two or more standard deviations below the community norm.
Predictors of Quality of Life
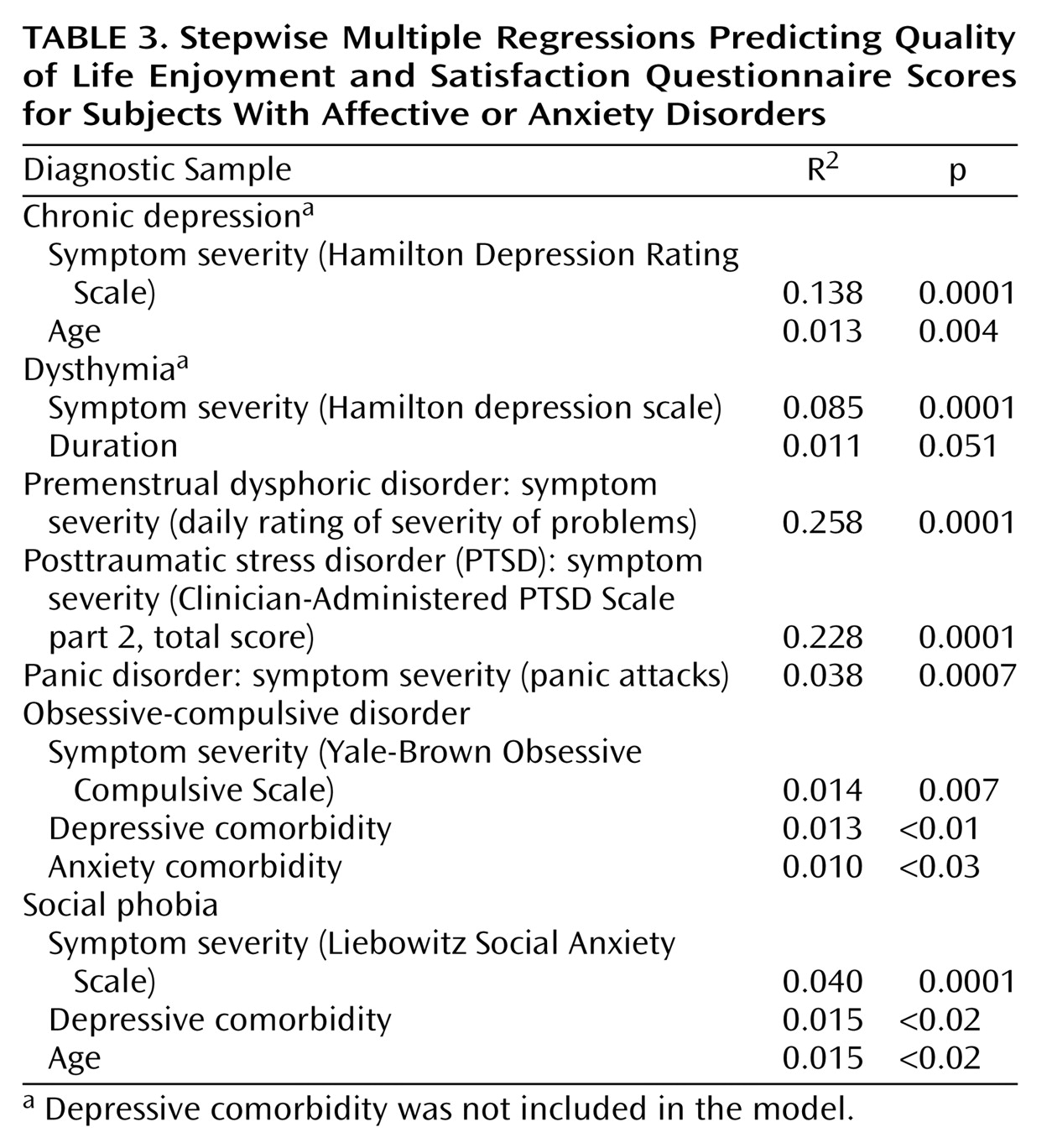
In addition to demographic variables (age, sex), duration of illness, and comorbidity, severity of illness-specific symptoms were examined as predictors of quality of life for each disorder. For the studies of major depressive disorder, chronic/double major depressive disorder, and dysthymia, the 17-item Hamilton Depression Rating Scale
(36) served as the measure of symptom severity. For OCD, the Yale-Brown Obsessive Compulsive Scale
(37) was used; for PTSD, the Clinician-Administered PTSD Scale part 2
(38) was the symptom severity measure; for premenstrual dysphoric disorder, the severity measure was the Daily Rating of Severity of Problems Form
(39); for social phobia, the Liebowitz Social Anxiety Scale
(40) was used.
Data Analytic Plan
Pearson’s correlations were used to compare the cumulative Quality of Life Enjoyment and Satisfaction Questionnaire total scores for the specific disorders with the single global item score for each disorder (item 16). Regression analyses were conducted for the eight different clinical samples to evaluate the diagnostic-specific and nonspecific clinical characteristics that contribute to quality-of-life impairment. For each disorder, a stepwise regression was conducted to enter duration of illness, age, anxiety comorbidity, depressive comorbidity, sex, and illness-specific symptom severity. Standardized coefficients were not compared since such contrasts require a priori hypotheses.
Discussion
Consistent with previous studies that employed a variety of instruments to measure quality of life and social dysfunction
(8–
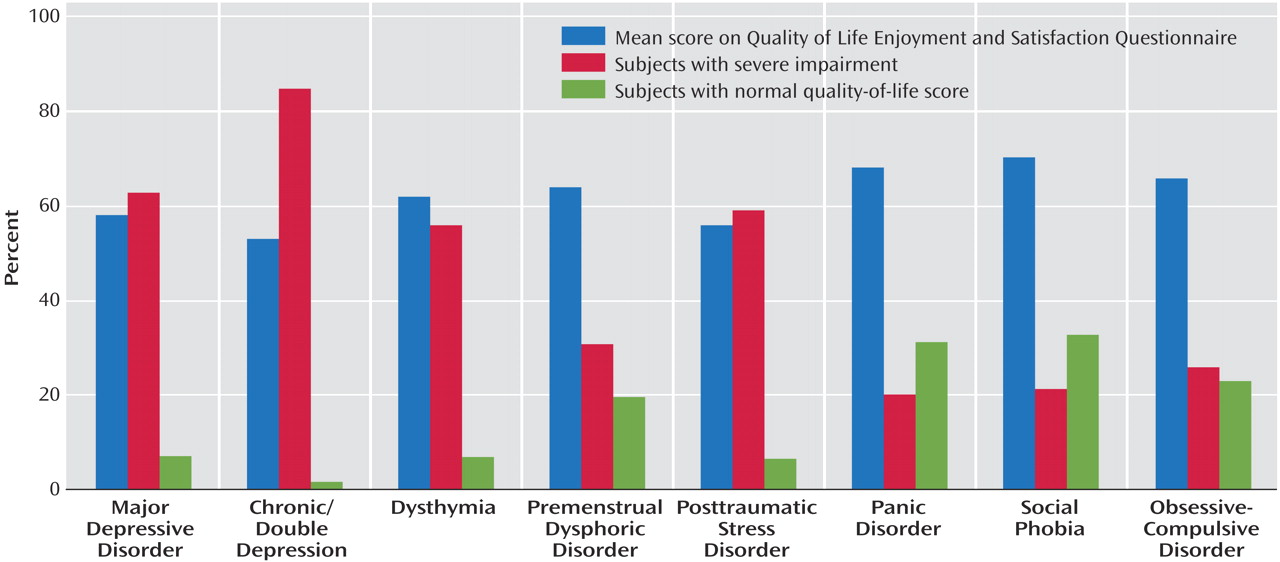
15), our examination of quality-of-life impairment with the Quality of Life Enjoyment and Satisfaction Questionnaire demonstrated substantial impairment in quality of life across anxiety and affective disorder subjects entering clinical trials. The typical subject with major depressive disorder, chronic/double depression, dysthymia, premenstrual dysphoric disorder, panic disorder, social phobia, or OCD has a Quality of Life Enjoyment and Satisfaction Questionnaire score that is considerably below the community norm, and many subjects with these disorders have severe impairment in quality of life. Even for the syndromes with the more benign levels of impairment in quality of life, less than one-third of subjects had Quality of Life Enjoyment and Satisfaction Questionnaire scores within 10% of the mean community normative value.
The chronic major depressive disorder sample had a high proportion of subjects with severe quality-of-life impairment and a low proportion of subjects with quality-of-life scores within 10% of the community norm. Eighty-five percent of the subjects with chronic/double depression had Quality of Life Enjoyment and Satisfaction Questionnaire scores in the severely impaired range, whereas 63% of the subjects with major depressive disorder and 56% of the subjects with dysthymia had Quality of Life Enjoyment and Satisfaction Questionnaire scores in the severely impaired range. These data are consistent with previous work demonstrating a monotonic gradient between the severity of depression and quality-of-life dysfunction
(41–
43).
Subjects with PTSD displayed an exceptionally high rate of severe quality-of-life impairment (59%). Examination of individual items of the Quality of Life Enjoyment and Satisfaction Questionnaire revealed that the impact of PTSD was broad, with substantial impairment occurring across all of the domains of quality of life. A greater severity of functional impairment in PTSD, compared with other anxiety disorders, has recently been reported in a large study of primary care patients
(44). In our analysis of subjects with PTSD, depressive comorbidity was not a significant predictor of the baseline Quality of Life Enjoyment and Satisfaction Questionnaire, although 37% of the PTSD patients in the sample had a current or lifetime history of a depressive disorder.
In general, our data suggest that anxiety disorders are associated with mild to moderate levels of impairment on the Quality of Life Enjoyment and Satisfaction Questionnaire. In contradistinction, studies that limit their comparisons to specific facets of quality of life or functional disability have reported greater impairment as well as specific differences in quality of life or dysfunction between anxiety disorders
(45–
47). This may reflect the unique impact of specific anxiety disorders on individual domains of quality of life (e.g., panic disorder limits mobility outside the home; OCD restricts employment success; social phobia affects social relationships). When more domains of quality of life are taken into account, the impact of severe dysfunction in a few domains may become diluted. Differences in sample ascertainment may be another important reason for these findings. Our sample is a carefully characterized but highly selected sample of research subjects, whereas the other studies investigated either epidemiological or clinical samples of convenience.
We hypothesize that the construct of quality of life may partially account for the apparent discrepancy between a clinician’s perception of more severe quality-of-life impairment for a patient with social phobia, panic disorder, or OCD and the patient’s usually less severe self-report of quality-of-life impairment. Definitions of quality of life have emphasized the importance of an individual’s perceptions of his or her life circumstances
(5). Therefore, one must consider how factors like an early age at onset or disease chronicity might alter perceptions. Social phobia and OCD are syndromes with a relatively early onset that are known to be associated with significant disability and impairment in work and social functioning
(37,
48,
49). The early onset of these disorders may alter the subjects’ perceptions of what constitutes a “normal” quality of life. Thus, subjects with OCD and social phobia may not perceive their quality of life as being as limited as subjects with disorders that have a more precipitous onset during adulthood. With these disorders, specific measures of functioning in various domains may yield a different picture compared to measures of quality of life.
The analyses examining the impact of demographic and clinical factors on quality-of-life dysfunction for each disorder revealed that illness-specific symptoms explained only a small (1.4% for OCD) to modest (25.8% for premenstrual dysphoric disorder) percentage of the variance. This suggests that quality of life is a related but semi-independent component of DSM-IV syndromes. Once a mood or anxiety disorder is present, it appears as though other factors besides severity of symptoms affect quality of life. Such factors may include personality dimensions (e.g., hardiness), financial resources that allow for access to more enjoyable activities and lifestyle, availability of social supports, and degree of life success or attainment of life goals.
The finding that symptom severity does not account for a large proportion of the variance in quality of life also suggests that a complete picture of a patient’s presenting illness should include some type of assessment of quality of life. Treatment studies may want to incorporate quality of life not only as an outcome measure but also as part of the inclusion criteria for the selection of subjects. For example, one research strategy might target subjects with both moderate-to-severe symptoms and substantial impairment in quality of life to a more intensive treatment option (i.e., combined psychosocial and psychopharmacological treatments).
A limitation to the current investigation is that the samples were drawn from clinical trial studies. Subjects in these studies were recruited based on their willingness to participate in an experimental medication trial and therefore are not representative of all patients experiencing these syndromes in the community. The inclusion and exclusion criteria of these trials, particularly the limitations on medical and psychiatric comorbidity, also limit the generalizability of these findings to nonselected individuals with these syndromes. However, one advantage of the selected samples is that they facilitate the characterization of quality-of-life dysfunction in a relatively homogeneous cohort of subjects with moderate-to-severe symptom profiles. The high level of comorbidity found in community samples would hinder our ability to parse out the influence of the individual syndromes on quality of life. A second criticism of our work might be the lack of inferential statistical analyses reported in this article; however, we did not have a priori hypotheses that would justify employing such techniques. We felt that it was premature to generate hypotheses based on the limited published data available at the time that these analyses were initiated. Our concern is that post hoc statistical comparisons of quality-of-life differences among these samples might lead to spurious conclusions that could be perpetuated in the literature. An additional limitation is the arbitrary definition of “normative” quality of life that we implemented (i.e., within 10% of the community norm). As yet, there are no standards for setting the degree of discrepancy from a normative sample mean to evaluate whether a psychopathological sample has moved sufficiently toward normalcy
(50). Further research is necessary to determine whether different standards for defining normative influence findings in regard to quality-of-life differences. A fourth limitation is that we examined only a single measure of subjective quality of life. Assessments of the range of mood and anxiety disorders on multiple measures of quality of life, as well as measures of functional impairment, are needed. We also acknowledge that we assessed a relatively restricted set of demographic and symptom measures in these preliminary regression analyses. However, our review of the literature suggests that the variables we analyzed were the ones most likely to account for the variance in quality of life.
We believe that this article can serve as the impetus for future research comparing and contrasting quality of life across psychiatric syndromes. Studies investigating the relationship between quality of life and functional impairment in nonselected clinical populations clearly are needed. Experiments employing our data as the rationale for hypotheses assessing the impact of mood and anxiety disorders on quality of life should be initiated. In general, more thoughtful research investigating the relationship between quality of life, measures of disability, symptom profiles, and demographic variables is warranted.
In summary, our cross-sectional cross-disorder analyses of subjects entering medication trials revealed a substantial degree of quality-of-life impairment for all anxiety and affective disorders examined (major depressive disorder, chronic major depressive disorder, dysthymic disorder, premenstrual dysphoric disorder, PTSD, panic disorder, social phobia, and OCD). Illness-specific symptom measures were consistently associated with levels of quality of life in all disorders, but the amount of variance exhibited was not large. This suggests that quality of life is a semi-independent measure of patients’ perceptions of their illnesses and should be part of the diagnostic evaluation and treatment plan for patients with mood and anxiety disorders.