Considerable controversy surrounds the proper role of short-term inpatient psychiatric treatment for the acute care of young people following an intentional self-injury
(1). Whereas some clinical researchers have questioned the necessity and usefulness of admitting acutely self-injurious youth for inpatient psychiatric treatment for other than medical reasons
(2), others have developed specific psychiatric indications for admitting suicidal youth to the hospital
(3). In practice, emergency room clinicians must grapple with determining whether acutely self-injurious children and adolescents can be safely managed from a medical and psychiatric perspective in treatment settings that are less restrictive and disruptive than hospital care. A wide range of clinical considerations—including medical severity of the attempt, child risk factors, availability of family support and community resources, cost and reimbursement issues, and concerns over adherence with follow-up treatment plans—influence the clinical decision of whether to admit a young person for inpatient care following a self-inflicted injury
(4,
5).
In the current study, we examine national trends from 1990 to 2000 in community hospital admissions of young people 5–20 years of age with intentional self-inflicted injuries. Using nationally representative data, we describe changes in the rates at which young people were admitted to community hospitals with such injuries and characterize changes in the method of injury, clinical diagnoses received, length of inpatient stay, discharge status, inpatient costs, and primary payer. As a result of changes in the managed care environment, we anticipated that there would be a decline in the rate of youths hospitalized with self-inflicted injuries, a decrease in their length of stay, and an increase in the proportion diagnosed with high-risk conditions, such as mood and substance use disorders, strongly associated with youth suicide.
Method
Data were drawn from the 1990 and 2000 nationwide inpatient samples of the Healthcare Costs and Utilization Project
(10). The project is sponsored by the Agency for Healthcare Research and Quality and includes over 100 clinical and nonclinical variables. The Healthcare Costs and Utilization Project consisted of 6,268,515 computerized discharge reports from a geographically diverse sample of 882 community hospitals in 1990 and 7,450,992 discharge reports from a diverse sample of 994 hospitals in 2000. Community hospitals include nonfederal short-term general hospitals and academic medical centers but not specialized psychiatric hospitals. Each year the Healthcare Costs and Utilization Project approximates a 20% stratified sample of U.S. community hospitals. Selection into the sample is based on a stratified probability selection of short-stay nonfederal general hospitals. Weights were constructed on the basis of the reciprocal probability of sampling to approximate national estimates. All percentages in this report are weighted to adjust for the sampling probability.
We limited the analysis to data from youths 5–20 years of age who were admitted to the hospital on an urgent or emergent basis and had a discharge diagnosis for intentional self-inflicted injury (ICD-9-CM: E950.0–E959.9). To estimate population rates of hospitalization for self-inflicted injury, population data were culled from the 1990 and 2000 United States Bureau of the Census
(11).
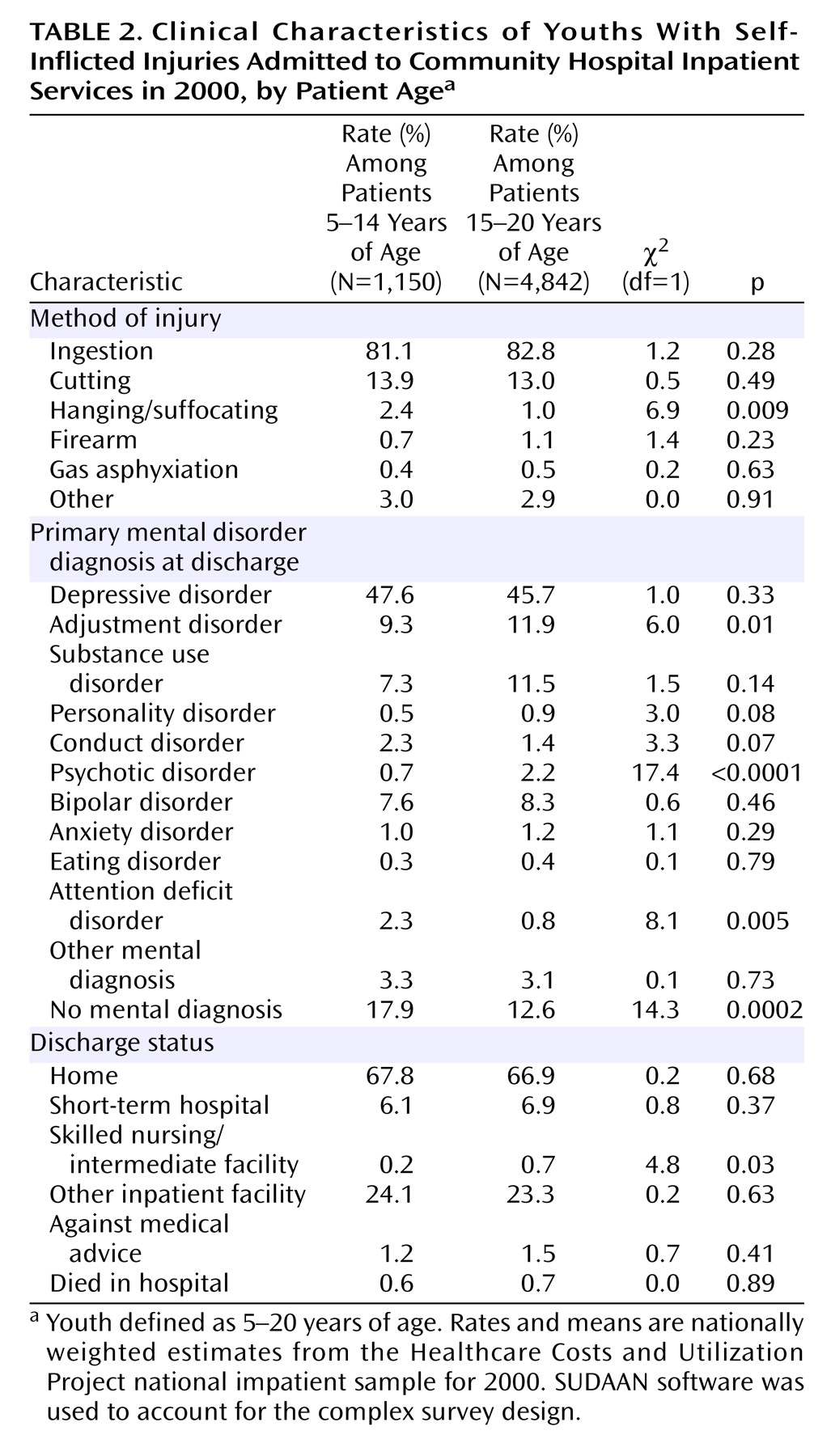
Our first goal was to describe the method of injury, primary mental disorder diagnosis, length of stay, and discharge status of youth by gender and age group in 2000. We then described trends in the hospitalization rate of youths with intentional self-injury between 1990 and 2000. We determined rates of intentional self-injury per 100,000 population, both overall and stratified by age and gender. Substantial missing race/ethnicity data and changes in the federal classification of race/ethnicity categories during the study period prevented a meaningful analysis of these variables.
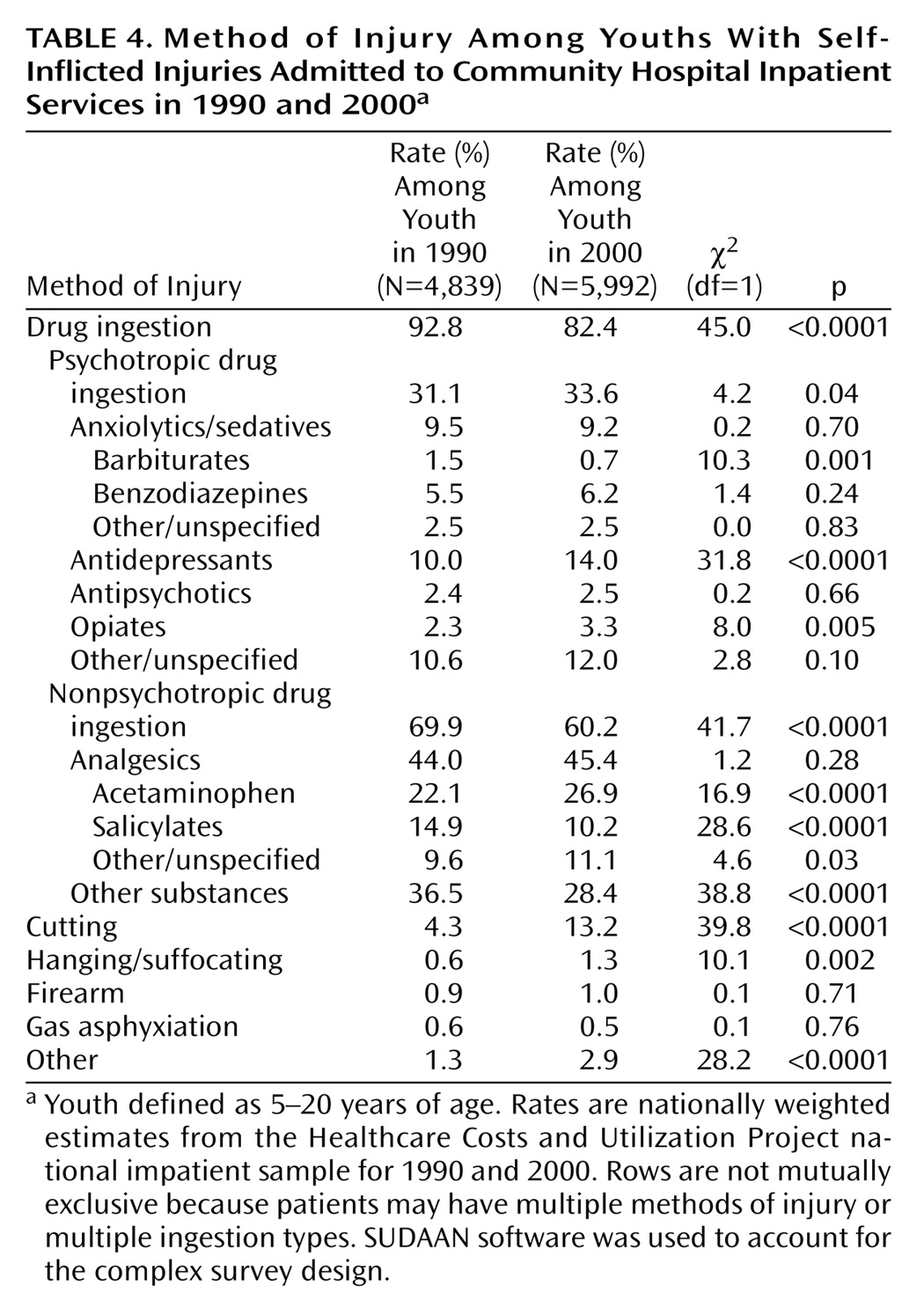
We then examined trends in the distribution of self-injury method. Injuries were first classified by major category: drug ingestion (E950), hanging/suffocating (E953), firearm (E955), gas asphyxiation (E951, E952), cutting (E956), and a residual group of other types of injury (E954, E957, E958, E959). Psychotropic drug ingestion was subsequently subclassified on the basis of discharge diagnosis codes: anxiolytics/sedatives (barbiturates, benzodiazepines, and others), antidepressants, antipsychotics, opiates, and other/unspecified psychotropic drugs. Nonpsychotropic ingestion was subclassified as analgesics (acetaminophen, salicylates, and other/unspecified) and other nonpsychotropic substances.
We then examined trends for mean length of stay, discharge status, primary payer, and primary mental disorder diagnoses among youth admissions with intentional self-injuries. Primary mental disorder was defined as the first-listed diagnosis that was a mental disorder (ICD-9-CM: 219–320). Mental disorders were classified into depressive disorders (ICD-9-CM: 296.2, 296.3, 298.0, 300.4, 311), adjustment disorders (309), substance use disorders (291, 292, 303, 304, 305), personality disorders (301), conduct disorder (312, 313.81), psychotic disorders (295, 297–299), bipolar disorder (296.0, 296.1, 296.4–296.9), anxiety disorders (300.0, 300.2, 300.3, 308.3, 309.21, 309.81, 313.0), eating disorders (307.1, 307.5), attention deficit hyperactivity disorder (314), and other mental disorders. A separate category was constructed for discharges with no mental disorder diagnosis.
Because cutting or self-mutilation is rarely associated with completed suicide in young people
(12) and tends to be less lethal than other forms of self-injury
(13), we also examined overall trends in hospitalization of youths with intentional self-injury excluding cutting (E956). Finally, total inpatient expenditures were calculated for all youths admitted with self-inflicted injuries in 1990 and 2000 and for all admissions excluding self-injury by cutting. The Consumer Price Index for medical care was used to inflate 1990 to 2000 dollars
(14).
We used the SUDAAN statistical software package
(15) to accommodate the complex sampling design and weights from the Healthcare Costs and Utilization Project when calculating means and corresponding standard errors and to calculate 95% confidence intervals (CIs) for the rate estimates.
Discussion
Between 1990 and 2000, there was a statistically nonsignificant decrease in the annual rate of community hospital inpatient service utilization among youths admitted following intentional self-injury (from approximately 49 per 100,000 in 1990 to 45 per 100,000). This trend roughly parallels the national decline in suicides among youths 15–19 years of age, from 11.1 per 100,000 in 1990 to 8.2 per 100,000 in 2000
(12).
The trend in hospital admissions may portray important changes in the care of young people who intentionally injure themselves. During the period from 1991 to 2001, the Youth Risk Behavior Survey reported a substantial increase in the rate of injurious suicide attempts by students in grades 9 through 12, from 1.7% to 2.6%
(16,
17). In the context of increasing base rates of self-injurious behavior, a slight decline in inpatient admissions of youths with intentional self-inflicted injuries suggests that the proportion of suicide attempts resulting in inpatient care has substantially declined.
In line with previous epidemiological
(18) and clinical research
(19), hospitalization as a result of self-inflicted injury was more common among female than male youths. Male youths were less likely than female youths to have a depressive disorder
(20) or an eating disorder
(21) but were more likely to have substance use disorder
(22). Male youths were also proportionately more likely than female youths to use more highly lethal methods of self-injury
(23) and to die in the hospital.
For young children ages 5 to 9 years, the rate of hospitalization with self-inflicted injuries, although still comparatively low, significantly increased during the study period. This trend should alert clinicians to the risks of suicidal behavior in young children. While the cause of this increase remains unknown, some evidence links child exposure to video games and movie violence to violent attitudes
(24) and behavior
(25). One small study has suggested that younger children who attempt suicide report many of the same depressive symptoms common to suicidal adolescents
(26). The recent increase of inpatient admissions of young children with intentional self-inflicted injuries highlights the importance of prevention and early intervention programs that target preschool
(27) or early grade school
(28,
29) children at risk for mental health problems.
The changing diagnostic profile of young people admitted to the hospital following intentional self-injury could indicate a more focused approach for especially high-risk youth. Between 1990 and 2000, the proportion of discharges in which a mood disorder or substance use disorder was the first listed mental disorder significantly increased, whereas the proportion of adjustment disorder or no mental disorder discharges significantly declined. Psychological autopsy studies reveal that mood disorders occur in approximately two-thirds of youth suicides
(30–
32) and that substance use disorders occur in up to two-thirds of older boys who complete suicide
(30,
32). By contrast, young people with adjustment disorders or no mental disorder are considerably less common among youth suicides
(30,
32).
A trend toward more severe mental disorder diagnoses among inpatient youth discharges suggests the importance of developing rapid and efficient diagnostic procedures to identify young people with high-risk conditions
(33). In one recent study, a school-based program for high school students that focused on depression and suicide risk was associated with a reduction in suicide attempts
(34).
The trends in mental disorder diagnoses among youths hospitalized following self-inflicted injuries may reflect broad changes in diagnostic practices or clinical decision making in response to managed care restrictions on inpatient care for less severe mental disorders. To explore this possibility, we performed a set of post hoc Healthcare Costs and Utilization Project analyses. The trends observed among admissions with self-inflicted injuries were also apparent in the larger sample of youth admissions with a primary mental disorder diagnosis. For example, among youth admissions with primary mental disorder diagnoses, the proportion who were diagnosed with an adjustment disorder declined from 1990 (16.8%) to 2000 (6.5%), whereas increases were seen in depressive disorder (25.7% to 34.4%) and bipolar disorder (4.2% to 12.2%). Because similar trends were further observed among youth whose admissions were self-pay or not charged (adjustment disorder: 19.4% to 7.9%; depressive disorder: 18.4% to 31.1%; bipolar disorder: 2.0% to 9.6%), it is unlikely that the diagnostic trends are simply a coding response to restrictive utilization management policies.
During the decade under study, there was a particularly impressive increase in the proportion of hospitalizations in which bipolar disorder was the leading mental disorder diagnosis. Bipolar disorder in young people has been associated with an increased risk of suicide attempts
(35) and completion
(2,
36). In one case/control study of youth suicide, the odds ratio of suicide completion for bipolar disorder approached that for substance use disorders
(36). However, manic or manic-like symptoms in young people may be difficult to distinguish from symptoms of ADHD
(37,
38), and concern exists that there has been a trend toward overdiagnosis of youth bipolar disorder
(39). From the available data, it is not possible to determine the extent to which the increase in discharges associated with bipolar disorder represents a true change in diagnostic composition as opposed to a change in diagnostic practices. Little attention has thus far been focused on early intervention in young people with bipolar disorder
(40).
There was also a trend toward shorter hospitalizations for young people with self-inflicted injuries. Together with the trend toward limiting care to those with more severe diagnoses, the shortening of inpatient treatment may be placing inpatient staff under increased time pressures to locate appropriate outpatient care. Under these constraints, it is perhaps not surprising that an increasing proportion of inpatients were transferred to other inpatient facilities.
In the acute outpatient management of suicidal young people, encouraging results have been reported with rapid-response outpatient psychiatric teams
(41), home-based interventions
(42,
43), interpersonal problem-solving skills training
(44), and brief cognitive behavior therapy for family members
(45). It is not known whether access to these and other relevant outpatient mental health services has expanded to help compensate for the narrowing role of short-term hospitalization in the care of young people with intentional self-inflicted injuries.
Several changes occurred in the pattern of intentional self-injury methods. Methods associated with high case fatality rates, including gas asphyxiation, hanging/suffocating, and firearms
(23), remained relatively uncommon, possibly because of deaths in the community or the emergency room before hospital admission. Although ingestions declined as a proportion of admissions for intentional self-injury, there were proportionate increases in ingestion of acetaminophen, antidepressants, and opiates. These proportionate increases, together with proportionate decreases in barbiturate and salicylate ingestions, may reflect changes in the general use of these substances
(46). The increase in acetaminophen ingestion is especially noteworthy because it poses a serious risk of potentially fatal hepatic toxicity
(47) that may not be appreciated by young people
(48).
During the study period, there was also an increase in the inpatient treatment of intentional self-inflicted injury involving cutting. Self-mutilation in young people tends to have a very low potential for lethality
(23). In the United States, six adolescents (age range: 15–19 years) committed suicide by injury with a sharp object in 2000
(12). As compared with other types of self-injury, self-mutilation is clinically associated with greater patient perceived likelihood of rescue
(13), lower perceived certainty of death
(13), and lower rates of mood disorders
(49). When these presumably less clinically severe discharges were excluded from the analysis, there was a statistically significant decline in the rate of youths hospitalized with intentional self-injury: from 47.2 to 39.4 discharges per 100,000 youth.
This study has several limitations. First, diagnostic data are only a crude index of illness severity and risk of subsequent suicide. No information was available concerning several known suicide risk factors in young people including prior suicide attempts
(50), precipitating stressful life events
(51,
52), access to firearms
(2), and family psychiatric history
(51,
53). Second, no independent assessment was available of the clinical diagnostic codes. A growth in managed care and concepts of medical necessity
(54) may have resulted in a tendency to code patients as having more severe psychiatric disorders to justify admission under precertification utilization management policies. Third, the data permit no means of distinguishing admissions primarily for medical care associated with attempted suicide from admissions primarily for treatment of the underlying psychiatric disturbance. Fourth, the reported rates measure the total number of hospitalizations rather than the individual persons hospitalized. It would be useful to quantify the extent and characteristics of repeat admissions for attempted suicide. Fifth, stigma associated with suicide attempts may have resulted in systematic underreporting of intentional self-injury. Last, the analysis was limited to admissions to short-term community hospitals and does not include the large number of young people admitted directly to other types of inpatient facilities
(55).
Over the last several years, there has been little change in the overall rate of community hospital inpatient hospitalizations of children and adolescents with intentional self-inflicted injuries. However, the proportion of young self-injurious inpatients with high-risk conditions (including depressive, bipolar, and substance use disorders) has increased, and the length of their inpatient stays has declined. These changes, especially in light of increasing injurious youth suicide attempts in the community, indicate that inpatient care may have assumed a narrower and more limited role in the treatment of suicidal young people. As mental health care professionals have come to rely less extensively on inpatient treatment for the acute management of self-injurious young people, community service needs have likely increased for rapid-response, crisis-oriented outpatient care.