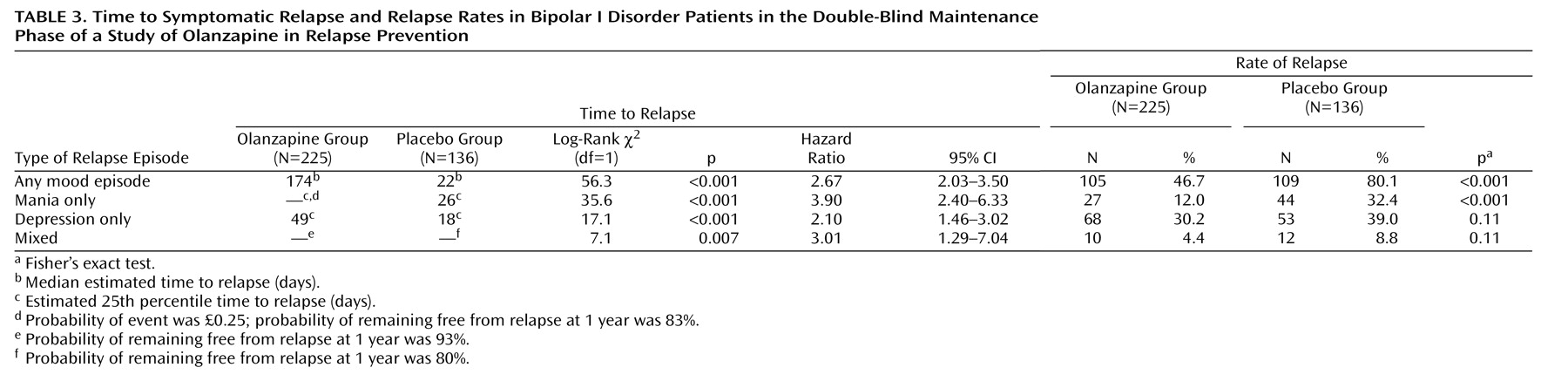
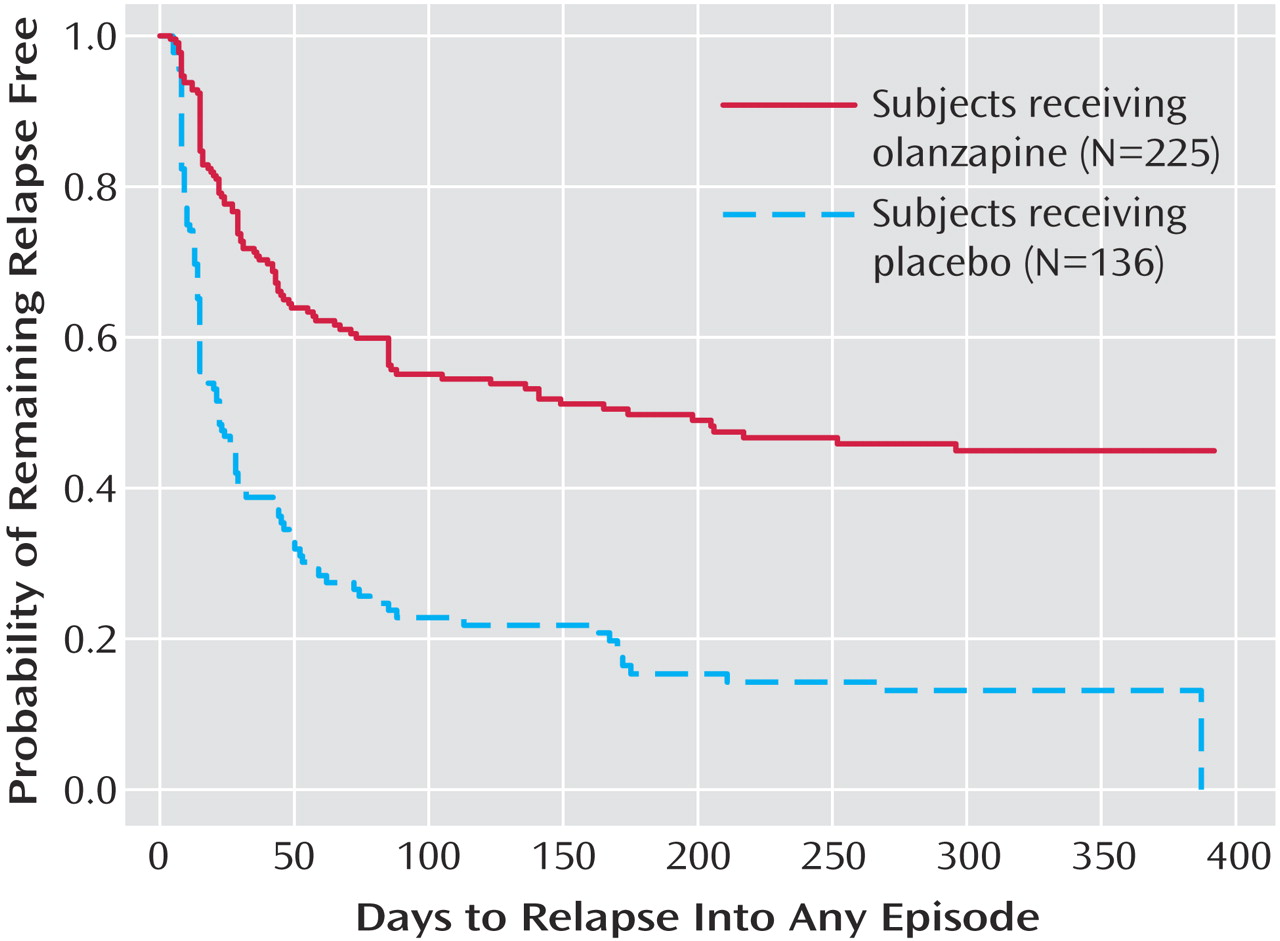
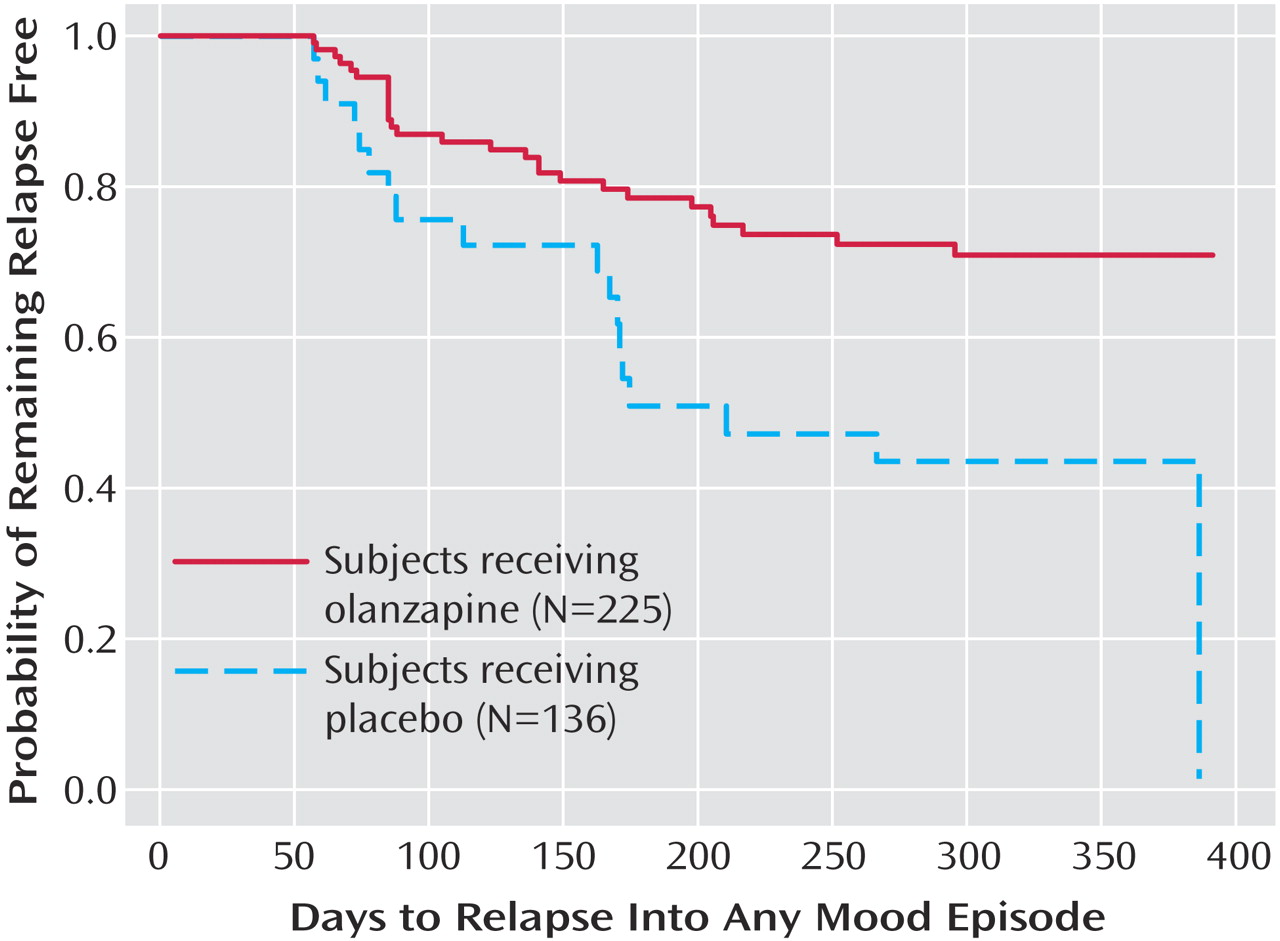
The primary outcome measure, time to symptomatic relapse into any mood episode during double-blind maintenance treatment, was significantly longer for patients who received olanzapine than for patients who received placebo (
Table 3). The median estimated time to symptomatic relapse into any mood episode was 22 days for the placebo group and 174 days for the olanzapine group (
Figure 1) (log-rank χ
2=56.3, df=1, p<0.001). Post hoc stratified Cox regression analysis with site or country as stratification factors provided results that were similar to those of the primary analysis (site: hazard ratio=2.89, p<0.001, 95% CI=2.15–3.88; country: hazard ratio=2.79, p<0.001, 95% CI=2.13–3.66). For relapse into mania (
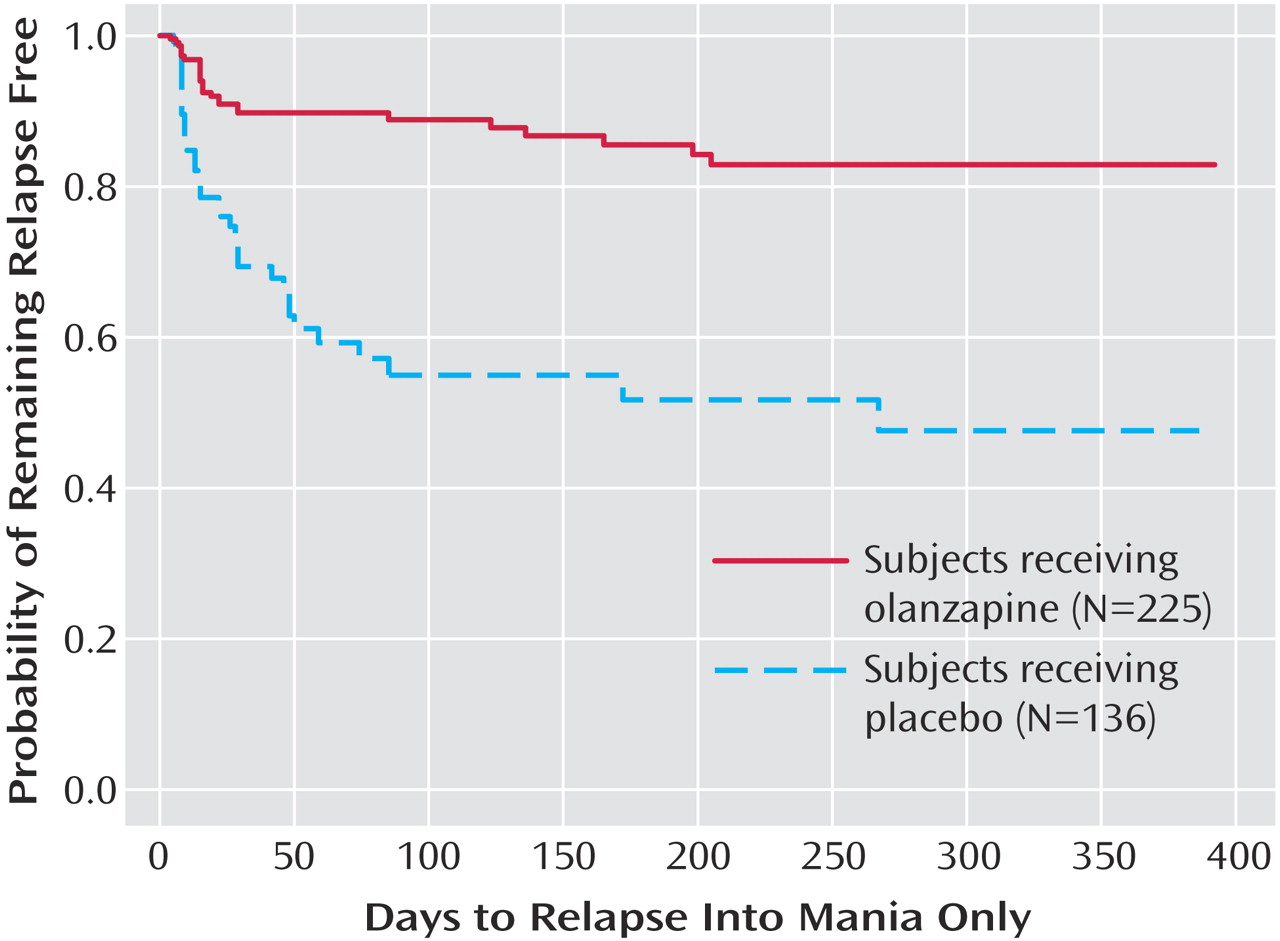
Figure 2), the estimated 25th percentile time to relapse was 26 days for the patients who received placebo and was not calculable for the olanzapine group; however, the patients who received olanzapine had an 83% probability of remaining free from manic relapse for at least 1 year (χ
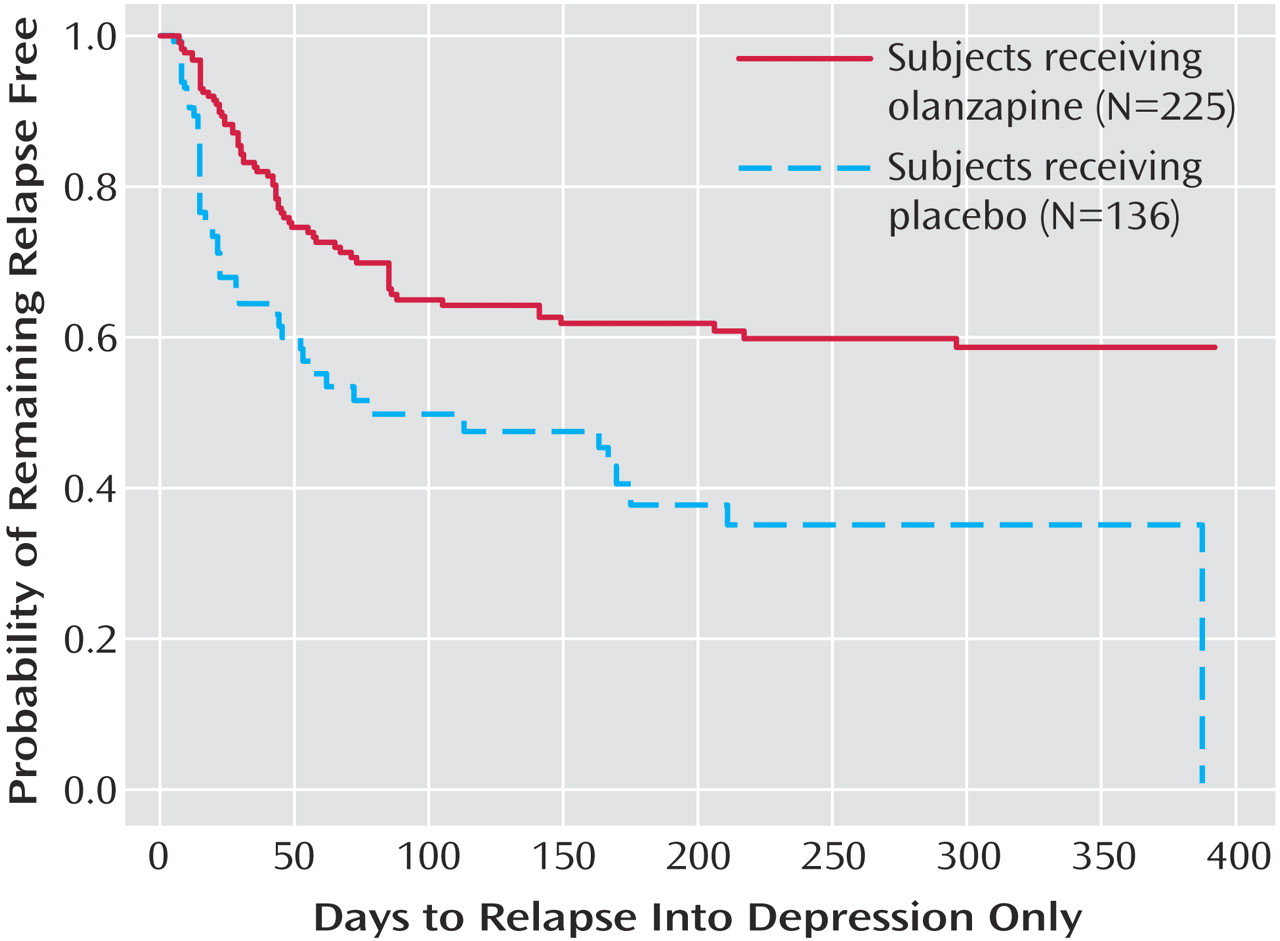
2=35.6, df=1, p<0.001). For relapse into depression (
Figure 3), the estimated 25th percentile time to relapse was 18 days for the placebo group and 49 days for the olanzapine group (χ
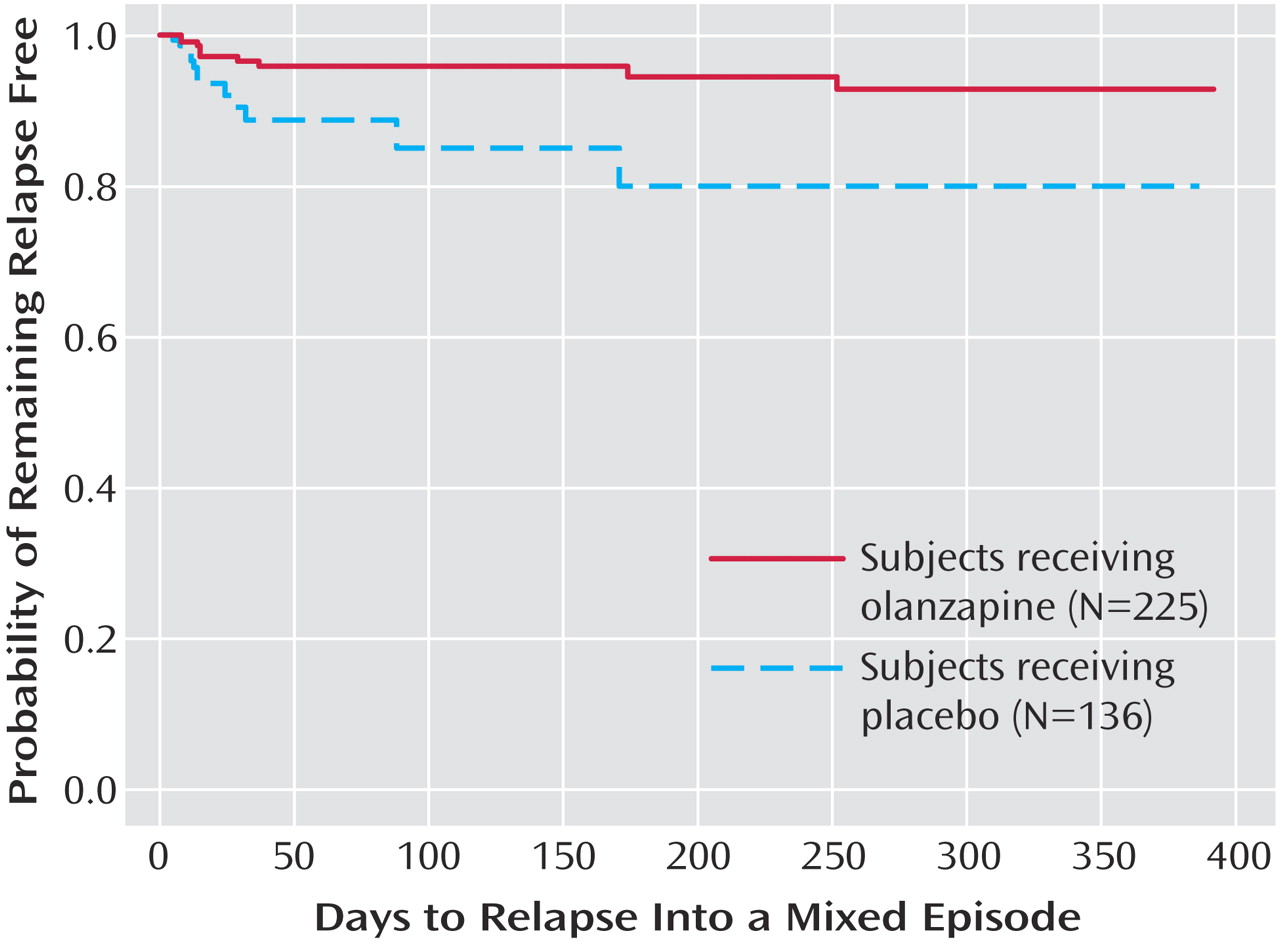
2=17.1, df=1, p<0.001). Because of the small number of events, time to mixed episode relapse (
Figure 4) could not be estimated for either group; however, at 1 year, the probability of remaining free from a mixed episode relapse was 80% for the placebo group and 93% for the olanzapine group (χ
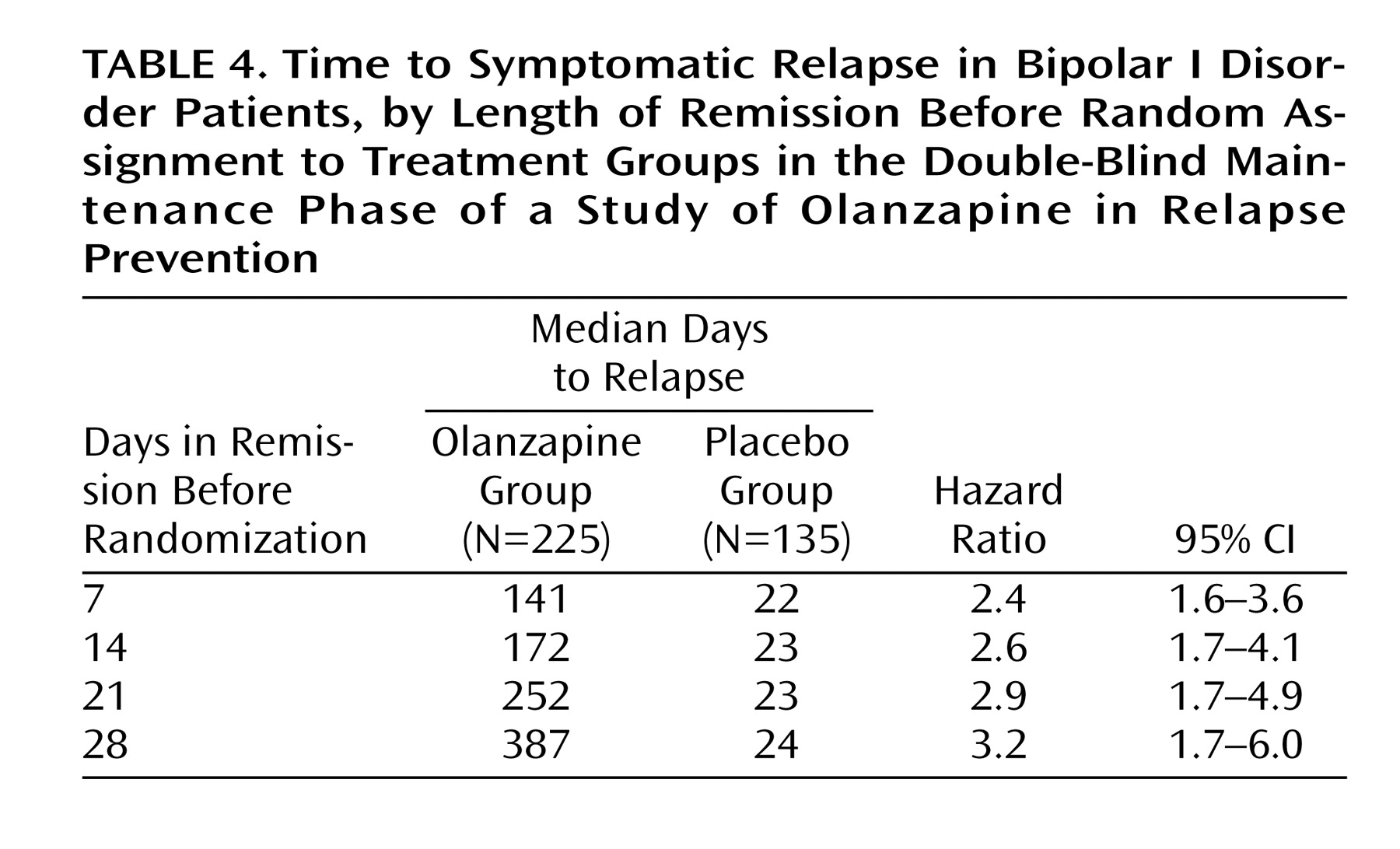
2=7.1, df=1, p=0.007). Post hoc analyses were conducted to determine if time in remission was associated with time to relapse. A proportional hazards regression analysis that included length of remission before randomization as a covariate was used to predict time to symptomatic relapse into any mood episode. Remission lengths of 7, 14, 21, and 28 days had minimal effects on the estimated median time to relapse for patients who received placebo (
Table 4). The data, however, show that longer time in remission before randomization was numerically but not statistically significant associated with longer time to relapse (χ
2=2.61, df=1, p=0.11).
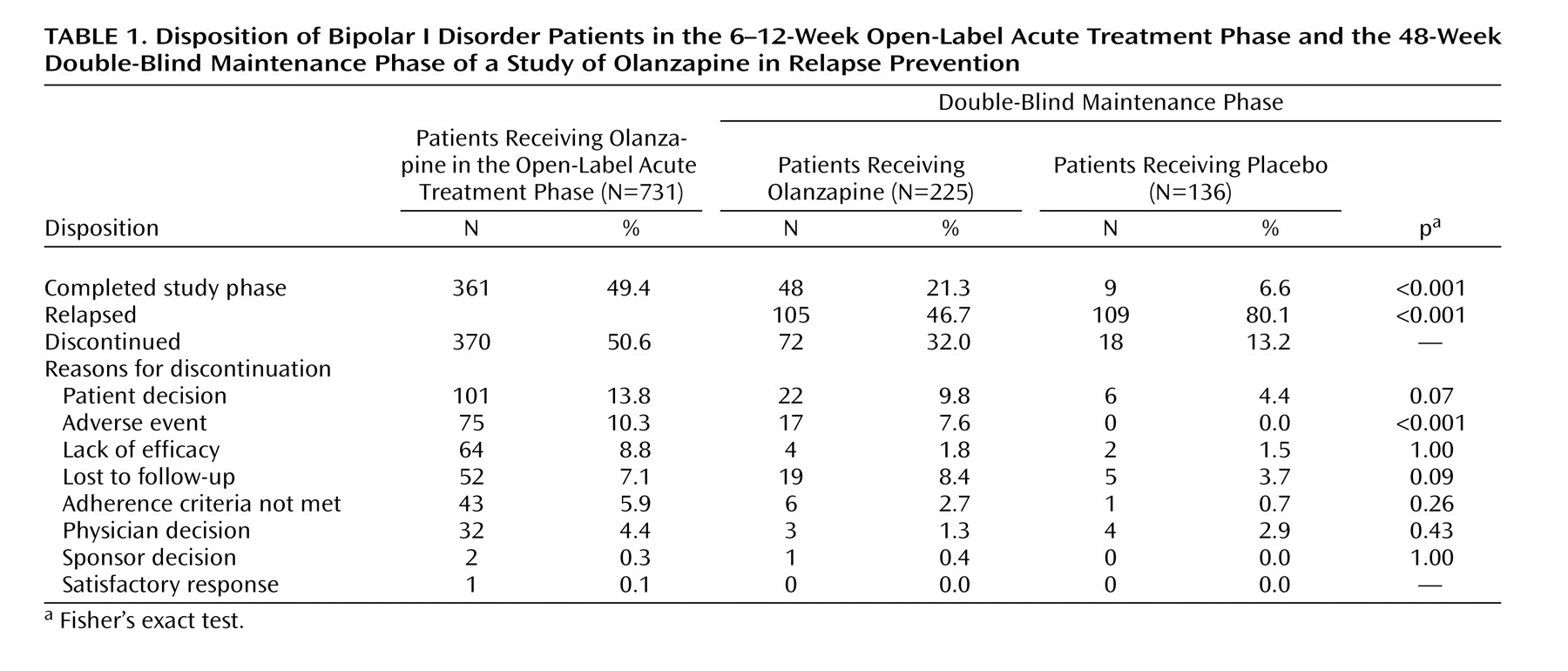
Rates of relapse during the double-blind maintenance phase are reported in
Table 3. Symptomatic relapse into any mood episode occurred in 105 (46.7%) of 225 patients in the olanzapine group and 109 (80.1%) of 136 patients in the placebo group (odds ratio=4.61, 95% CI=2.81–7.58). These risk-of-relapse results correspond to a number needed to treat of 3.0 (95% CI=2.3–4.1), indicating that treating three patients with olanzapine prevents one relapse that would otherwise have occurred with placebo. It is noteworthy that most relapses were identified on the basis of YMRS and/or HAM-D scores; the relapses of only nine patients (olanzapine group: N=2; placebo group: N=7) involved hospitalization, and the YMRS or HAM-D criteria were met by eight of these nine relapsing patients when they were assessed within a few days after hospital admission. Post hoc analyses were conducted to control for early relapses in the double-blind phase after discontinuation of open-label treatment with olanzapine. Analyses of relapse were performed with data from the subset of patients who remained in symptomatic remission during the double-blind phase for at least the first 2 weeks (olanzapine group: N=204; placebo group: N=87) and the first 8 weeks (olanzapine group: N=112; placebo group: N=34). Among patients with a minimum remission time of 2 weeks during the double-blind phase, 43.1% (N=88) of those who received olanzapine experienced symptomatic relapse to any mood episode, compared to 71.3% (N=62) of those who received placebo (p<0.001, odds ratio=3.27, 95% CI=1.90–5.61). When patients with relapses during the first 8 weeks of the double-blind phase were excluded, symptomatic relapse to any mood episode occurred in 25.0% (N=28) of the patients who received olanzapine and 52.9% (N=18) of the patients who received placebo (p=0.003, odds ratio=3.38, 95% CI=1.52–7.49); furthermore, the median estimated time to symptomatic relapse into any mood episode was significantly longer for the olanzapine patients (median undefined) than for the placebo patients (median=211 days) (
Figure 5) (χ
2=9.0, df=1, p<0.003).
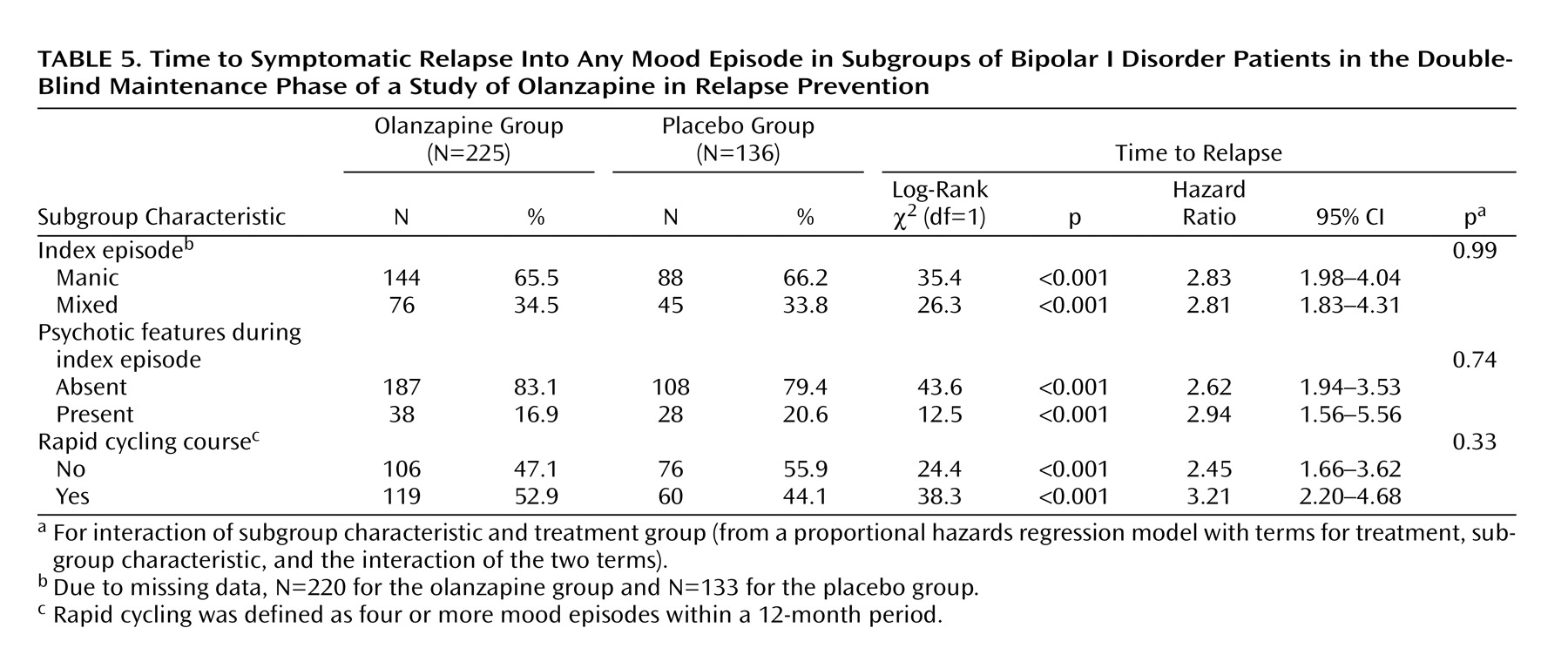
Relapse data were analyzed in terms of the patients’ demographic and baseline clinical characteristics. Factors included age (<40 versus ≥40 years), sex, racial origin (Caucasian versus other), presence versus absence of psychotic features, nature of the index episode (manic versus mixed), and presence versus absence of a rapid cycling course. Analyses of time to symptomatic relapse into any mood episode revealed no interactions between the treatment groups and subgroup characteristics.
Table 5 reports the results for nature of the index episode and the presence or absence of psychotic features and rapid cycling. Separate analyses of data from patients with a manic index episode or a mixed index episode revealed that, in both groups, time to relapse into any mood episode was significantly longer in patients who received olanzapine than in patients who received placebo. In addition, olanzapine treatment significantly lengthened time to symptomatic relapse in patients with and without a history of a rapid cycling course, as well as in those with and without psychotic features.