Most patients with bipolar I or bipolar II disorder spend more time in the depressed than the manic phase of their illness
(1). Antidepressant medications play a pivotal role as adjunctive treatment to mood stabilizers for depressive episodes. Concerns exist, however, about the potential of antidepressants to cause patients to switch into hypomania or mania
(2,
3). Data in some
(4,
5) but not all
(6) studies suggest that patients with bipolar II disorder may be less vulnerable to switching poles when treated with antidepressants. We sought to explore whether a differential risk for switching exists, hypothesizing that there would be no significant differences in switch rates between depressed patients with bipolar I versus II disorder treated adjunctively with antidepressants.
Method
Patients who were participants in the Stanley Foundation Bipolar Network
(7–
9) provided written informed consent for participation in a 10-week randomized clinical trial for bipolar depression as approved by each local institutional review board. Inclusion criteria included having a DSM-IV depressive episode despite ongoing treatment with mood stabilizers within minimum specified blood level guidelines (lithium >0.7 meq/liter; valproate ≥50 μg/ml; carbamazepine ≥4 μg/ml). To exclude any patient with mixed mania, patients were included only if they had a score ≥16 on the Inventory of Depressive Symptomatology
(10) and a mania subscale score of 1 (not ill) on the Clinical Global Impression (CGI) bipolar illness scale
(11).
One hundred eighty-four bipolar depressed patients (134 [73%] with bipolar I disorder; 48 [26%] with bipolar II disorder; two [1%] with bipolar disorder not otherwise specified) were randomly assigned to receive one of three mechanistically different antidepressants—bupropion (N=55), sertraline (N=62), or venlafaxine (N=67)—as adjunctive treatment to one or more mood stabilizers. Patients were followed for 10 weeks. Doses of mood stabilizers, antipsychotics, and any ongoing benzodiazepines were held steady. Each antidepressant had an identically matched placebo, and all patients took two sets of study drug compounds throughout (one active and one placebo). Starting and maximal doses were 75 and 450 mg/day for bupropion; 50 and 200 mg/day for sertraline; and 37.5 and 375 mg/day for venlafaxine.
Patients were seen weekly for 2 weeks, then biweekly for 8 weeks. Assessments based on the Inventory of Depressive Symptomatology, the mania subscale of the CGI bipolar disorder scale, and the Young Mania Rating Scale (YMRS)
(12) were obtained at each visit. The reliability and sensitivity of the latter two scales for detecting different severities of hypomania/mania have been documented
(11,
12). A switch into hypomania/mania was operationalized as a score ≥3 (mildly ill) on the CGI mania subscale, or, more conservatively, a score >13 on the YMRS.
Results
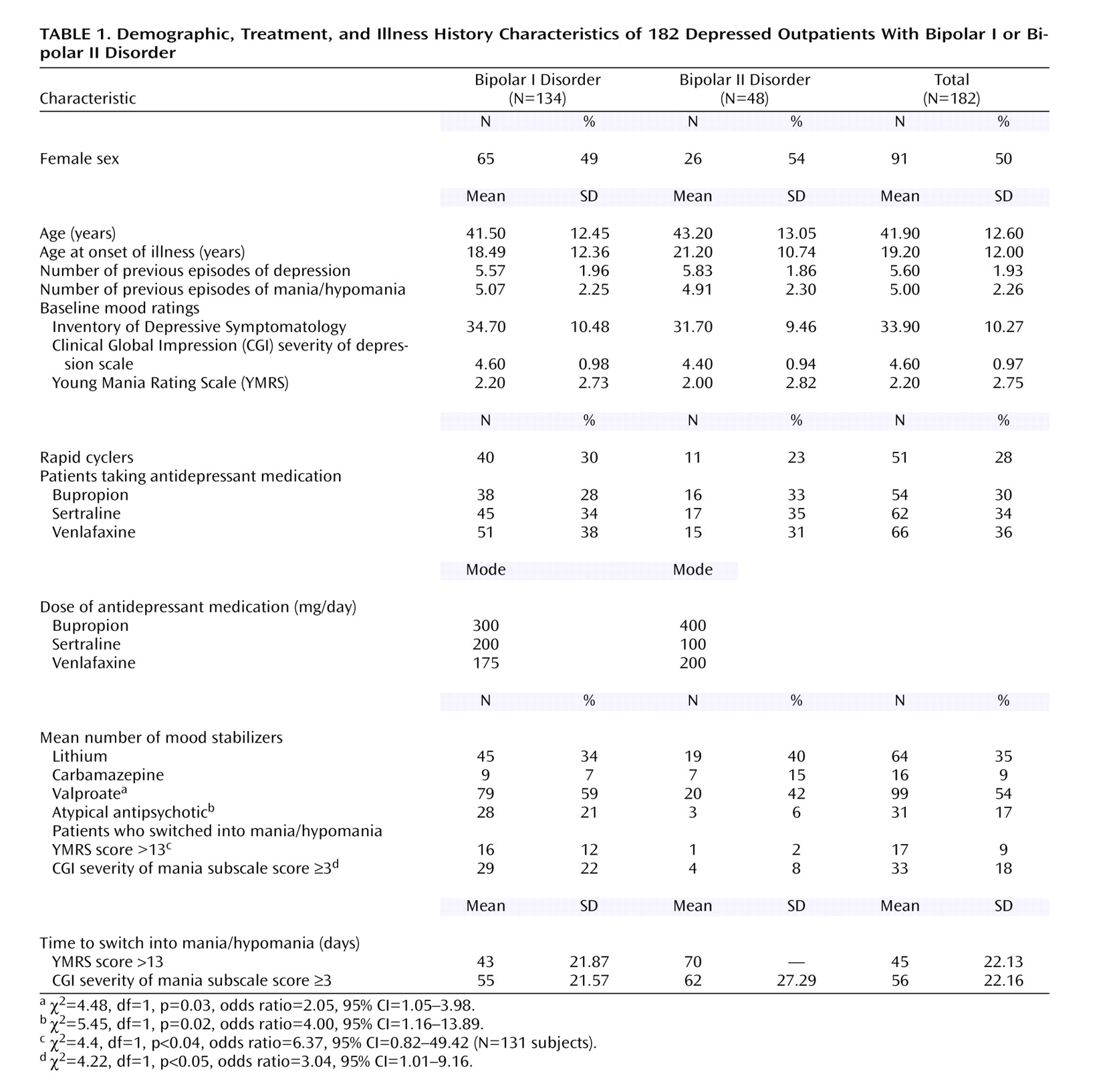
Table 1 displays demographic, course of illness, and medication variables for the 182 depressed patients with bipolar I or bipolar II disorder. There were no significant demographic differences between groups. Antidepressant medications were distributed equally in patients with bipolar I and bipolar II disorder (χ
2=0.53, df=2, p=0.77). Significantly more patients with bipolar I disorder than those with bipolar II disorder were taking valproate or atypical antipsychotics.
Switch rates into hypomania or mania based on YMRS criteria over the 10-week trial were low. Patients with bipolar II disorder were significantly less likely than those with bipolar I disorder to switch: 16 (12%) of the 134 patients with bipolar I disorder met YMRS criteria for a switch into mania, compared with one (2%) of the 48 patients with bipolar II disorder (χ2=4.4, df=1, p<0.04). Eleven patients with bipolar I disorder (8%) switched into hypomania (YMRS score=14–19), and five (4%) switched into mania (YMRS score=20–25). The one patient with bipolar II disorder who made a switch switched into hypomania (YMRS score=13.5). Two patients with bipolar I disorder (2%) and no patients with bipolar II disorder were hospitalized for mania. Using the less conservative CGI criteria, we found that 29 subjects with bipolar I disorder (22%) and four subjects with bipolar II disorder (8%) switched into hypomania/mania (χ2=4.22, df=1, p<0.05).
Our data add to a small literature
(4,
5,
13,
14) suggesting lower acute switch rates as a function of bipolar subtype. Our study suggests that depressed patients with bipolar II disorder may be less vulnerable than those with bipolar I disorder to switch poles even into mild hypomania when given an antidepressant adjunctively with a mood stabilizer. Two other treatment studies
(15,
16) suggested that antidepressant monotherapy may result in very low switch rates into hypomania or mania in depressed subjects with bipolar II disorder. Although antidepressant monotherapy is not supported in bipolar depression treatment guidelines, these studies nonetheless suggest a low vulnerability to switching in the bipolar II disorder population.
Several limitations exist in the current study. First, significantly more patients with bipolar I disorder than patients with bipolar II disorder received valproate and antipsychotics. However, this should have conferred greater protection against switch for the patients with bipolar I disorder, biasing results toward the null. Second, it is possible that standard rating scales for mania are less sensitive for measuring hypomania, and thus the switch of subjects with bipolar II disorder would be less likely to be observed. We used low cutoffs on the scales, however, to capture very minor changes in mood.
Since depression is a major cause of disability, finding the optimal treatment approach is critical, but the task of identifying patients vulnerable to switching and effectively treating such patients without causing harm (e.g., causing a switch into hypomania or mania or cycling) remains a challenge. Our study reports switch rates from an acute 10-week trial. A recent study employing NIMH Life Chart Methodology
(17) also demonstrated lower switch rates in patients with bipolar II disorder than patients with bipolar I disorder during longer-term follow-up. If low switch rates in patients with bipolar II disorder with acute and continuation antidepressant exposure are confirmed, different treatment algorithms for bipolar II disorder versus bipolar I disorder may be recommended.