The Schizophrenia Prodrome
A 13-year-old girl, currently in the eighth grade and with a history of attention deficit hyperactivity disorder, was brought by her mother to a university-affiliated outpatient psychiatric clinic after a gradual decline in her academic performance was noted. She had a previous history of receiving grades of B and C in all her classes, but currently she was getting Ds and Fs. At age 8 years she had begun receiving stimulant medication, with some benefit. She had tasted alcohol in the past but denied current use. She had also used marijuana a half-dozen times. She reported having a small number of close friends. Although she said that there were no recent changes in her peer relationships, her parents claimed that she had been withdrawn and had appeared sad and that at times they needed to prompt her to take a shower. She had a maternal aunt with bipolar affective disorder and a great uncle who had been institutionalized for unknown reasons. During the clinical interview, she was dressed in Goth attire, including a black T-shirt with images of letters dripping blood; she had dyed black hair. Her affect was blunted but was slightly more animated when her parents left the room. She denied thoughts of suicide. She reported occasionally hearing whispering voices calling her name and saying that she is worthless. She also reported the belief that her friends did not like her as much as they had. Her mother, who recently met a parent of a child with schizophrenia, posed the question of whether her daughter has schizophrenia.
Challenges of the Schizophrenia Prodrome
Developmental Pathophysiology and Psychopathology
Differential Diagnosis
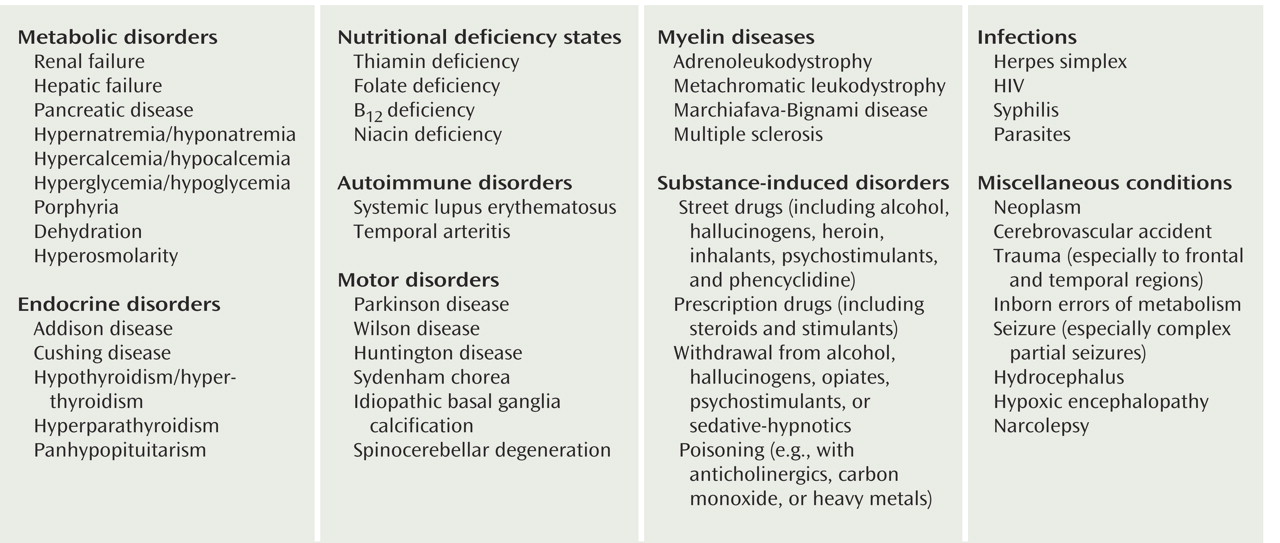
Nonpsychiatric Disorders
Affective Disorders
Substance Use Disorders
Pervasive Developmental Disorders
Personality Disorders
PTSD
Cognitive Problems
Assessment and Treatment
Conclusions
Footnote
References
Information & Authors
Information
Published In


History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).