Insomnia Definitions
“Insomnia” is used to refer to both a symptom and a disorder. The
symptom of insomnia is defined as a subjective complaint of difficulty falling asleep, difficulty staying asleep, or poor quality sleep. In DSM-IV-TR
(1), insomnia symptoms are included among the diagnostic criteria for several other mental disorders, including major depressive disorder and generalized anxiety disorder. Insomnia
disorders are characterized by insomnia symptoms accompanied by significant distress or impairment. In DSM-IV-TR the specific diagnosis of primary insomnia is further defined by a duration of at least 1 month and by symptoms that do not occur exclusively during the course of another sleep disorder, mental disorder, or medical disorder or result from use of substances or medications. Finally, DSM-IV-TR includes diagnoses of “secondary” insomnia disorders, that is, insomnia that causes significant distress or impairment or warrants independent clinical attention but is believed to be directly related to a coexisting mental disorder or medical disorder or to the effects of substances or medications.
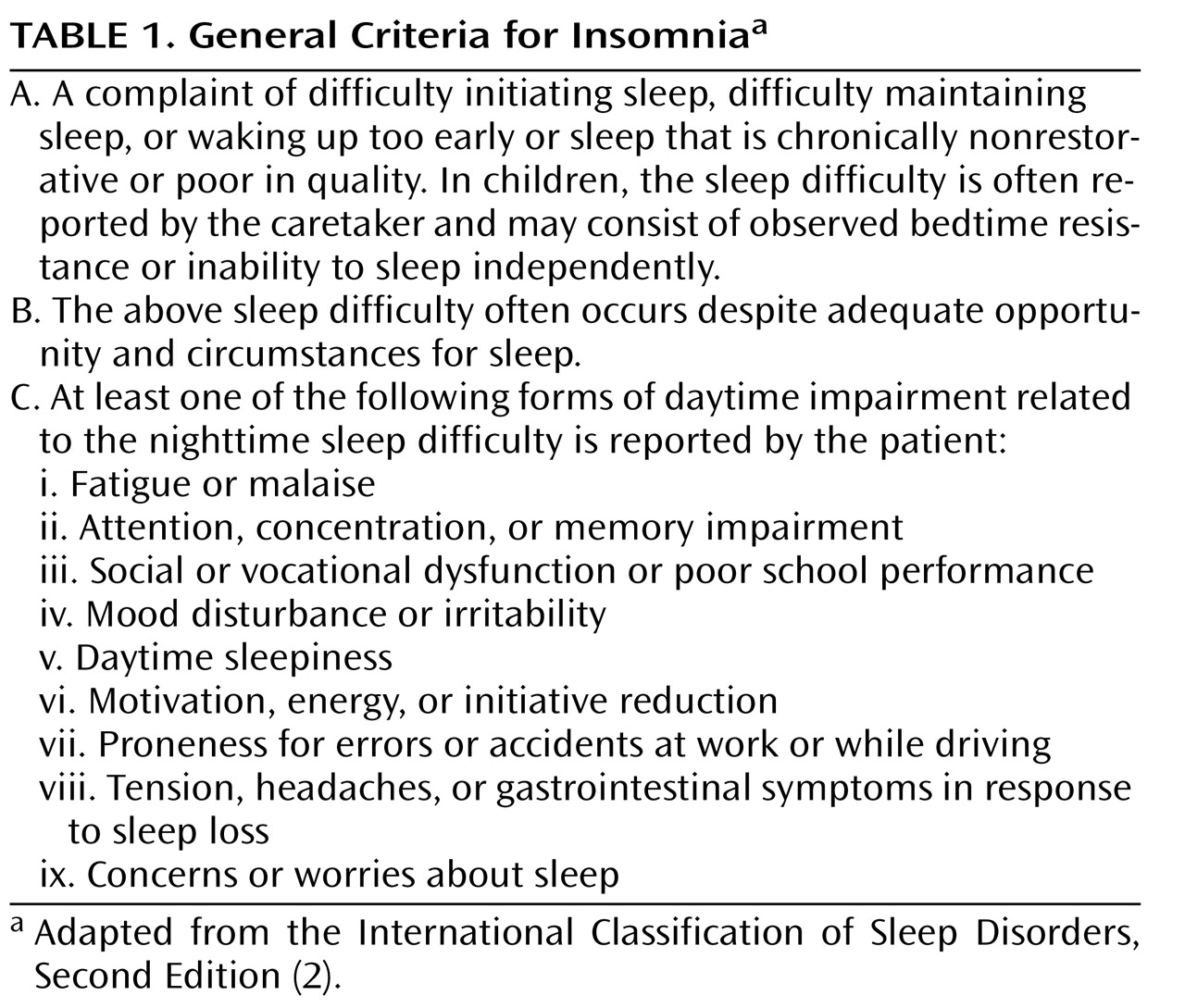
Sleep medicine specialists use the International Classification of Sleep Disorders, Second Edition (ICSD-2)
(2), to diagnose sleep disorders. ICSD-2 describes general criteria that are common to all insomnia disorders (
Table 1 ) as well as eight specific insomnia disorders (in addition to “unspecified” and “not otherwise specified” categories), each of which meets the general criteria along with more specific diagnostic criteria. For most purposes, the general insomnia criteria proposed in ICSD-2 serve as a useful basis for discussing insomnia as a clinical disorder.
Other classification schemes for insomnia have also been used. For instance, symptom-based classifications distinguish between sleep-onset and sleep-maintenance insomnia. However, longitudinal studies suggest that these specific symptoms have limited stability over time
(3) ; patients who present with sleep-onset insomnia at one time may present with frequent awakenings at a later time. Moreover, a majority of patients present with some combination of symptoms. Duration-based classifications (acute, short-term, and chronic) have also been suggested
(4) . Such classifications may provide clues to the cause of insomnia. For instance, acute and short-term insomnia are more often related to life stresses, acute illnesses, or medications, whereas chronic insomnia is more likely to be related to behavioral factors or the effects of chronic mental or medical disorders. However, the majority of patients in clinical trials and in clinical practice have chronic symptoms, which is the focus of this review.
Distinctions have also been drawn between primary and secondary insomnia disorders. The underlying rationale is that secondary insomnia is caused by another disorder, whereas primary insomnia has no other identifiable cause. However, as noted in the 2005 National Institutes of Health (NIH) State of the Science Conference statement on the Manifestations and Management of Chronic Insomnia in Adults
(5), such distinctions may not be helpful clinically. Insomnia often has multiple causes, and distinguishing when another condition “causes” insomnia can be difficult. For instance, the course of insomnia may not follow the course of the other disorder, and the two conditions may require different treatments. For this reason, the NIH conference commended the term “comorbid insomnia” as a preferable alternative to the term “secondary insomnia.”
Epidemiology
The prevalence of insomnia differs depending on the specific case definition used and the population assessed. However, whatever definition is used, insomnia remains the most prevalent sleep disorder in the population. Insomnia symptoms—that is, the complaint in the absence of specific duration or distress criteria—occur in some 30%–40% of adults, and specific insomnia disorders—that is, the complaint together with meeting duration and impairment criteria—occur in 5%–10% of adults
(6) . The latter is most relevant to clinical practice, since the majority of individuals with insomnia symptoms do not present for medical evaluation or treatment unless they have significant distress or impairment. Rates of insomnia are higher in medical and psychiatric care settings than in the general population.
A number of consistent risk factors for insomnia have been identified
(6,
7) . The strongest of these is concurrent depressive symptoms. Female sex is also consistently associated with insomnia, with a ratio of approximately 1.4:1. Increasing age, comorbid medical disorders, and comorbid psychiatric disorders are other consistent risk factors. Additional evidence also suggests that being separated or divorced, having lower income, lower socioeconomic status, increased chronic life stress, and black race are also associated with insomnia prevalence.
Insomnia often runs a chronic course. Longitudinal studies suggest that approximately 50% of individuals with insomnia continue to have symptoms after follow-up periods of 1 year or longer, and most cross-sectional studies of insomnia patients report a duration of several years
(8 –
10) . Although the number of true longitudinal insomnia studies is small, evidence suggests that improvement in medical and psychiatric conditions is associated with improvement in insomnia
(11) . As noted above, cross-sectional associations between insomnia and psychiatric disorders are strong, but additional evidence suggests that insomnia is a risk factor for the development of psychiatric disorders and for poor outcomes in these disorders. For instance, approximately a dozen longitudinal studies have demonstrated that insomnia is an independent risk factor for subsequent development of depression
(12) . This relationship has been observed from adolescence to later adulthood and is maintained after adjustment for concurrent depressive symptoms. In addition, insomnia is one of the most common persistent symptoms in individuals treated for depression, and its presence is a risk factor for nonresponse to depression treatment and for recurrence following remission
(13 –
15) .
Evaluation
A thorough clinical history is the cornerstone of evaluation for chronic insomnia
(16) . The evaluation should focus on the description of current symptoms, including not only the type of sleep disturbance at night but also sleep habits and patterns. In particular, the clinician should inquire about times of going to bed and getting out of bed, variability in sleep timing from day to day, and emotional, cognitive, and physical states surrounding sleep. Symptoms of other specific sleep disorders should also be considered. These include loud snoring and witnessed breathing pauses, which might suggest sleep apnea, and motor restlessness and involuntary leg movements, which might suggest restless legs syndrome.
Daytime consequences associated with insomnia should also be evaluated. The most common complaints include mood disturbance (typically described as irritability and mood lability, rather than depression or anxiety), fatigue, and complaints of cognitive inefficiency or difficulty concentrating. The majority of patients with chronic insomnia do not actually complain of daytime sleepiness, that is, the tendency to fall asleep in inappropriate situations. Rather, insomnia appears to be associated with difficulty sleeping at any time during the 24-hour day.
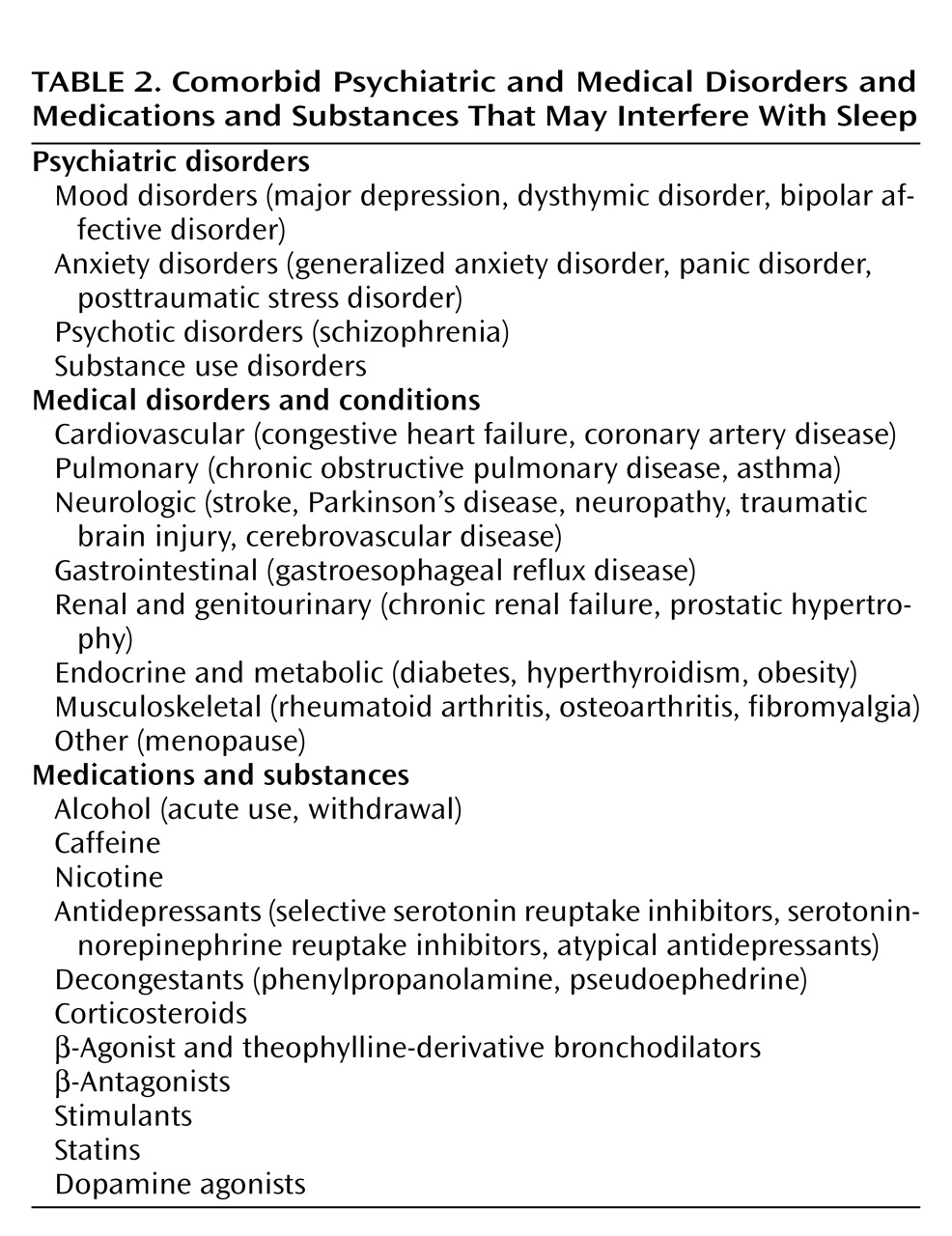
The evaluation of insomnia should also include careful consideration of comorbid psychiatric and medical disorders as well as medications and substances that might interfere with sleep (
Table 2 ). Virtually any psychiatric disorder can be associated with insomnia, but depressive and anxiety disorders are especially common. Likewise, a wide range of medical and neurologic conditions can be associated with insomnia. Particular attention should be given to those conditions that are associated with pain, breathing difficulty, and impaired mobility. Medications that affect any CNS neurotransmitter can be associated with insomnia. Common examples include high doses of caffeine, alcohol, and antidepressants, particularly selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and atypical antidepressants.
It is often useful to view the insomnia history in terms of predisposing, precipitating, and perpetuating factors
(17) . These factors can help identify potential causes of insomnia and treatment targets. Predisposing factors include family/genetic diathesis and chronic mental or medical disorders that increase the likelihood of insomnia symptoms. Precipitating factors are acute events or experiences that may push vulnerable individuals over the threshold into acute insomnia. Perpetuating factors include behavioral patterns (e.g., spending excessive time in bed) and medical or medication factors that maintain insomnia symptoms over time.
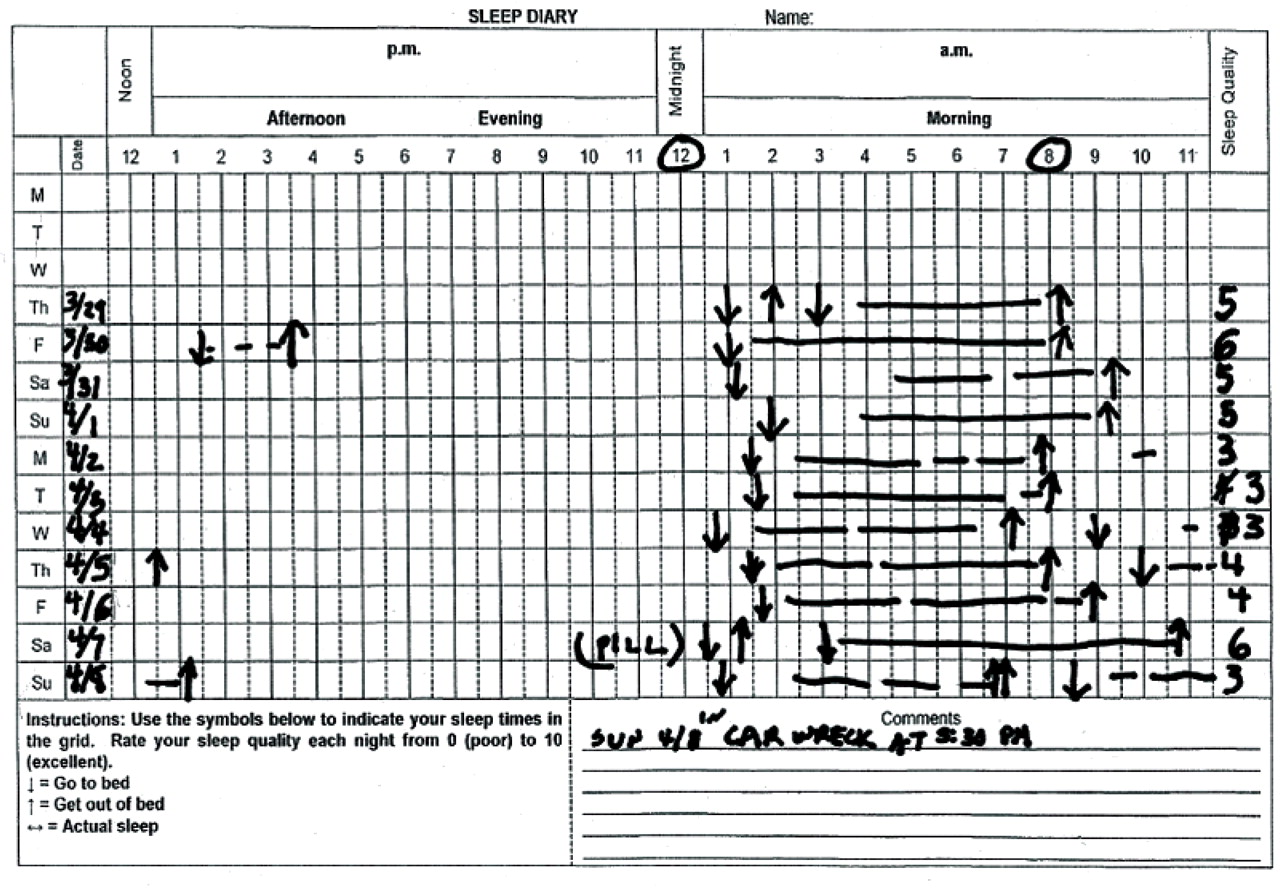
The clinical history can be usefully supplemented by collection of a 2-week sleep-wake diary. This is a prospective charting of a patient’s actual sleep hours and habits, and it can usefully identify variability in sleep patterns and specific daytime correlates that may provide targets for subsequent intervention (
Figure 1 ).
Specific laboratory testing has limited utility in the diagnosis and assessment of insomnia. However, in specific situations, general metabolic panels, CBC, or endocrine testing (e.g., thyroid hormone) may be useful. Overnight sleep studies with polysomnography are not routinely indicated in the evaluation of chronic insomnia. However, in specific situations, such testing may be useful. For example, individuals with a high index of suspicion for sleep apnea should be referred for polysomnographic testing. Risk factors include obesity, loud snoring, witnessed pauses in breathing, craniofacial abnormalities, or factors that might lead to a central dysregulation of breathing, such as congestive heart failure and stroke. Insomnia patients with unusual behaviors during sleep, such as violent behavior, should also be considered for polysomnography. Finally, failure to respond to usual insomnia treatments may warrant referral to a sleep specialist and, in some cases, polysomnography.
Psychological and Behavioral Treatment
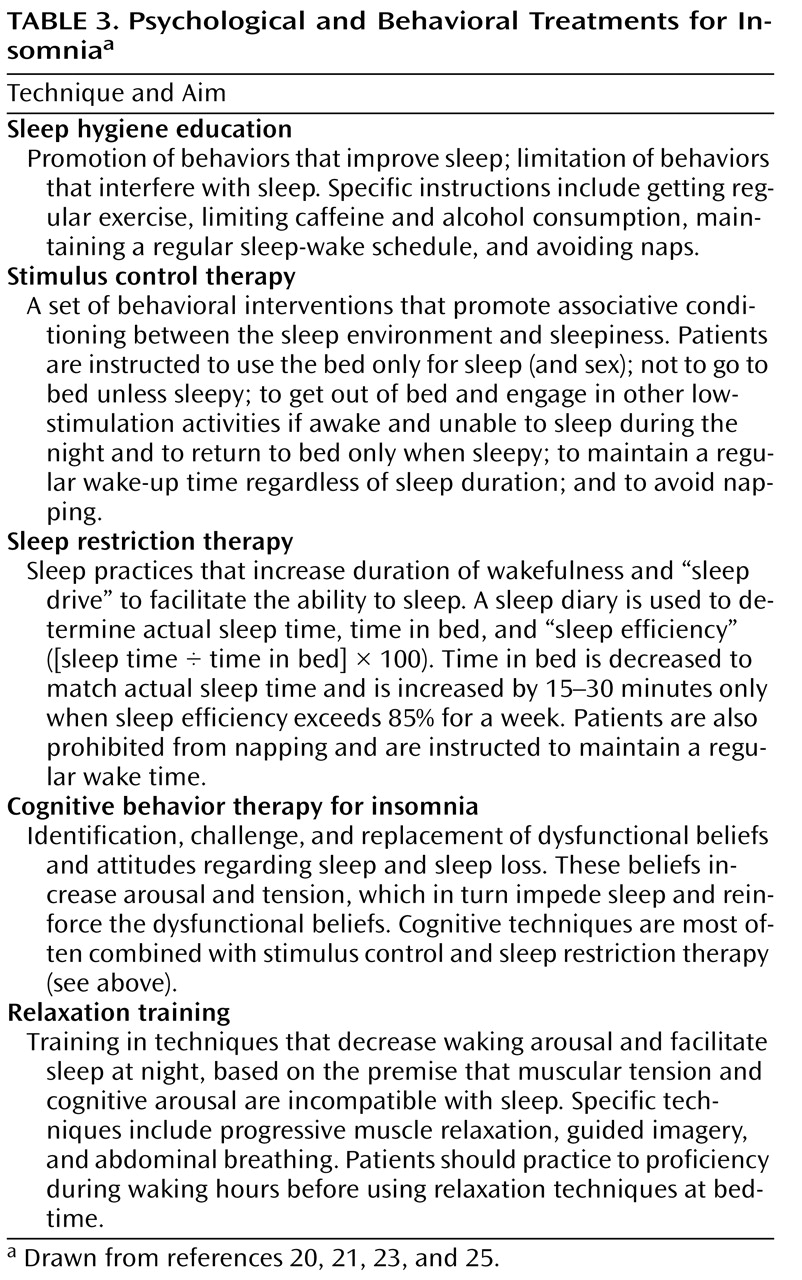
Both psychological-behavioral treatments and pharmacologic treatments have demonstrated efficacy in the treatment of chronic insomnia. A variety of psychological and behavioral techniques have been evaluated in well-designed controlled clinical trials. Specific techniques include sleep restriction therapy, stimulus control therapy, relaxation approaches, and multimodal cognitive-behavioral treatment for insomnia
(20) . The general features of these treatments are summarized in
Table 3 . Qualitative and quantitative analyses of treatment studies using these techniques have indicated robust treatment effects on a variety of self-report sleep outcome measures and a smaller number of objective sleep outcome measures using polysomnography
(21) . Published treatment manuals and self-help books describe the specific techniques for these treatments, which are simple enough to implement in routine clinical practice
(22 –
25) .
The various psychological and behavioral treatments for insomnia share several common elements that have been combined into briefer forms of treatment. Common elements to many of these treatments include 1) education regarding sleep, sleep needs, and physiological regulation of sleep; 2) the establishing of more regular sleep hours, with particular emphasis on the time of arising in the morning; 3) limitation of time in bed to more closely match the individual’s actual sleep hours; 4) reinforcement of the bed and bedroom as a stimulus for sleep rather than for wakefulness and frustration about sleep. The mechanisms of psychological-behavioral treatments are unknown, but these common elements suggest the potential importance of augmenting homeostatic sleep drive, providing regular sleep-wake (and dark-light) cues for the circadian timing system, and reducing cognitive-affective arousal.
Psychological-behavioral treatments for chronic insomnia may be provided by psychologists and other behavioral medicine specialists with adequate training. In addition, certification in behavioral sleep medicine is provided by the American Academy of Sleep Medicine. More basic forms of psychological-behavioral treatments may be provided by other health professionals, including nurses as well as physicians.
Pharmacologic Treatment
Numerous prescription and nonprescription agents have been used to treat insomnia. Agents currently approved by the U.S. Food and Drug Administration (FDA) for treatment of insomnia include eight benzodiazepine receptor agonists (BzRAs) and one melatonin receptor agonist. Although several barbiturate and miscellaneous nonbarbiturate drugs (e.g., chloral hydrate, ethchlorvynol) are also approved as sedative-hypnotics, they are not recommended for clinical use given their low therapeutic index. Approved BzRAs include a set of drugs that are true benzodiazepines as defined by their chemical structure and a set of drugs that are not benzodiazepines but appear to share a common mechanism of action. BzRAs act at a specific recognition site on g-aminobutyric acid type A (GABA
A ) receptors in the CNS; this recognition site is distinct from the GABA recognition site itself
(26) . Benzodiazepines have affinity for several subtypes of GABA
A receptors, which are defined by the specific composition of five protein subunits. Some nonbenzodiazepine BzRAs have greater selectivity for GABA receptors containing an alpha
1 protein subunit. The sedating and amnestic effects of BzRAs both appear to be related to affinity for alpha
1 -containing GABA
A receptors, but the clinical significance of drug specificity in vivo is uncertain.
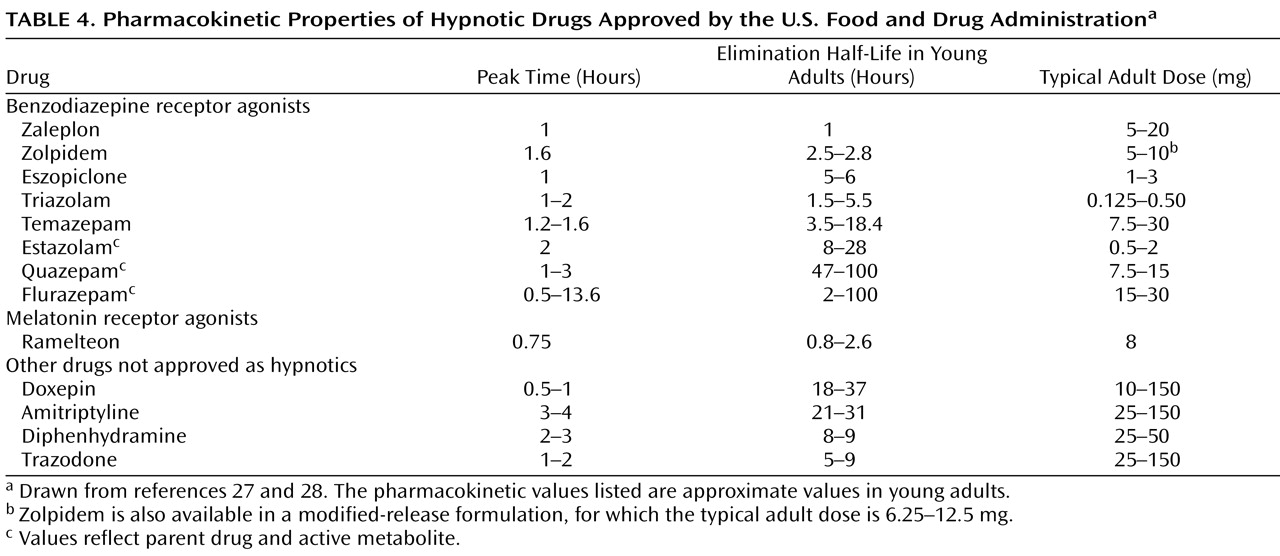
BzRAs differ from each other mainly in terms of pharmacokinetic properties, and particularly in terminal elimination half-life (
Table 4 ). Available agents have terminal elimination half-lives ranging from 1 to 120 hours. The duration of action of a drug is most strongly, although not exclusively, related to half-life. Therefore, selection of a particular drug often depends on the ideal duration of action for a particular patient, rather than on any specific distinctions between drugs.
BzRA drugs as a class reduce sleep onset latency and increase total sleep time; depending on the specific pharmacokinetics of the drug in question, decreased wakefulness after sleep onset may also result. Qualitative and quantitative analyses of clinical trials with BzRAs demonstrate their efficacy as judged by self-report and objective outcomes
(29,
30) . However, as is the case with psychological and behavioral treatments, few studies have paid attention to functional outcomes or to the broader insomnia syndrome.
BzRAs also share a similar set of adverse effects, which include anterograde amnesia, postural instability, and sleepiness
(16,
31) . The presence of such side effects may be related to the specific drug’s half-life; impaired memory and daytime sedation are more likely with agents having long half-lives. A range of more serious behavioral adverse consequences, including sleep-related eating, sexual behavior, and even driving, have been reported anecdotally and in the lay press. Although most of these reports have occurred in association with zolpidem, which is the most widely prescribed drug in this class, it seems likely that similar adverse effects are possible with any agent in this class.
BzRAs may also be associated with rebound insomnia, withdrawal, tolerance, and dependence
(16,
31) . Rebound insomnia has been demonstrated predominantly with short-acting drugs, and it can be minimized by gradual dose tapering and even by alternate-day dosing after the dose has been reduced. Withdrawal symptoms can also be minimized by dose and frequency tapering. Abuse of BzRA drugs as agents of first choice is not common. However, individuals who abuse these drugs commonly abuse other substances, and the use of higher-than-prescribed doses or requests for early prescription refills should raise concern. Hypnotic dependence has both physiological and psychological determinants. Physiological aspects of dependence are related to the discontinuation effects noted above. Psychological aspects of dependence are related to the fear or belief that good sleep will not be possible without medications. This may lead some individuals to continue taking medications for extended periods, even in the absence of clear therapeutic benefits.
BzRAs have also been shown to be useful for individuals with comorbid insomnia, including those with comorbid depression
(32) . They also reduce insomnia in perimenopausal women with hot flashes
(33) . Both nightly dosing and intermittent (e.g., three times per week) dosing have been shown to be efficacious
(34) . Although most clinical trials have been conducted for 1 week or less, recent evidence from double-blind studies shows continued evidence for efficacy for up to 6 months of nightly use
(35) .
One melatonin receptor agonist, ramelteon, has been shown to be efficacious for treatment of insomnia
(36) . Its primary effect appears to be on sleep onset latency, with little effect on wakefulness during the middle of the night. Its side effect profile appears to be relatively benign, although increased blood levels have been observed in older adults, and some hormonal alterations (e.g., reduced testosterone) have been observed.
A wide variety of drugs that have not been approved by the FDA for the treatment of insomnia have been used in clinical practice. These include sedating antidepressant drugs, sedating antipsychotic drugs, and sedating anticonvulsant drugs, often used in low doses. Small clinical trials have supported the efficacy of low doses of trazodone and sedating tricyclic drugs for treatment of insomnia
(16) . Their role in the routine treatment of chronic insomnia has not been defined, but they are likely to be most useful in patients who have a history of substance use and those who have a contraindication or poor response to BzRAs. Important side effects of these drugs include orthostatic hypotension and anticholinergic effects, which are of particular concern in the elderly. Even greater concerns are raised by the use of sedating antipsychotic drugs, which may have metabolic and neurologic side effects. Therefore, their use for treatment of sleep disturbance is recommended only in cases of insomnia that is comorbid with psychiatric disorders that independently warrant their use, such as severe bipolar disorder.
Alcohol and antihistamines are the most commonly used self-treatments for insomnia. Alcohol may help promote sleep initially, but it disrupts sleep for the remainder of the night and raises the additional issues associated with chronic alcohol use. Very little evidence is available supporting the efficacy or safety of diphenhydramine or other antihistamines for the treatment of insomnia. In addition, their anticholinergic properties raise safety questions, particularly in older people. Finally, naturopathic remedies such as valerian
(37) have been assessed in some clinical trials. However, substantial difficulties arise in the standardization of these products, and their overall efficacy is marginal at best.
Treatment Implementation
Before initiating any treatment, the clinician should determine whether the patient’s insomnia symptoms warrant treatment, as indicated by the severity of sleep symptoms, daytime symptoms, and distress. Reasonable treatment goals should also be discussed. For instance, patients should recognize that some degree of night-to-night variability in sleep quality is natural and may be experienced even after treatment. Their sleep problems should become more manageable with treatment, however, and their daytime function can improve. Treatment outcomes should focus not only on the quantitative sleep parameters, such as sleep latency, wakefulness after sleep onset, and sleep duration, but also on qualitative aspects of the individual’s sleep and daytime function.
Psychological and behavioral treatments are appropriate in almost all cases of chronic insomnia. A simplified approach focusing on education and behavioral principles, as outlined above, may result in substantial improvement in some cases. Referral to individuals with specific training in behavioral sleep medicine or the use of cognitive-behavioral approaches may also be appropriate.
Pharmacologic treatment may be appropriate when the insomnia causes significant symptoms, distress, or impairment. Medication effects and side effects should be discussed with the patient. In most cases, initial treatment with a short-acting BzRA is a reasonable first step. Depending on initial treatment response, a second BzRA with either a shorter or longer half-life may be tried. In the event of nonresponse, or in the case of individuals with a history of substance abuse, a trial of a sedating antidepressant at a low dose may be a reasonable approach.
Unresolved Issues
Although a great deal has been learned about the epidemiology, pathophysiology, and treatment of chronic insomnia, other questions remain to be answered. First, the optimal method of combining behavioral and pharmacologic treatments remains to be determined. Some evidence suggests that psychological-behavioral treatment alone may provide superior long-term outcomes, but the combination may provide better short-term outcomes
(38) . A second unresolved issue is the length of treatment, particularly pharmacologic treatment. Although previous assumptions about a rapid development of tolerance have not been borne out in recent double-blind placebo-controlled studies, it is a common clinical observation that patients say the drug is “no longer working.” In addition, discontinuation of long-term treatment with hypnotics often results in further improvements in sleep
(39) . Third, the benefits of intermittent or as-needed medication use, as opposed to nightly treatment, remain to be defined. Finally, it has not been clearly demonstrated whether treating insomnia leads to consistent improvements in comorbid conditions or other more general aspects of daytime functioning. Early evidence suggests that treatment of insomnia may improve outcomes of comorbid depression
(40,
41), but further controlled trials are needed.