“The Golden Gate Bridge is practically suicide proof. Suicide from the bridge is neither possible nor probable.”
–Chief Engineer Joseph Strauss, 1936
The Golden Gate Bridge is a magnificent architectural accomplishment. At its completion in 1937 it was the longest suspension bridge in the world. On May 27, the day before the bridge opened to traffic, a weeklong Golden Gate Fiesta began. Al Jolson sang, fireworks went off nightly, caravans came from the western states and from Mexico and Guatemala. Canadian Mounties, Alaskan dogsleds, and even a Chilean naval vessel took part in the festivities. By the end of that first day, as many as 200,000 people had crossed the bridge. On May 28, President Franklin Delano Roosevelt pressed a telegraph key in Washington announcing to the world the opening of the Golden Gate Bridge
(1) .
The bridge is 1.7 miles long and 90 feet wide. The roadway sits 220 feet above the water, and the towers rise another 500 feet above that. Two main cables containing 80,000 miles of wire pass over the towers. The bridge is painted international orange, blending with the sea and land. Driving or walking across the bridge offers vistas of San Francisco, Oakland, Berkeley, Alcatraz, and the San Francisco-Oakland Bay Bridge to the east and the Pacific Ocean to the west. More than 100,000 cars cross the bridge daily, or about 40 million annually. It is reportedly the most photographed man-made structure in the world.
But this colossal edifice has another, darker, side. Arguably the most beautiful bridge in the world, it is also the most lethal. The Golden Gate Bridge is the number one suicide site in the world. Bridge suicide counts are based on bodies recovered, which by 2008 was over 1,300. Bodies washed out to sea, jumpers witnessed but not found, and unclaimed cars in the parking lot are not counted. The actual number of deaths is probably closer to 2,000.
Three Vignettes
Billy
Billy was an 18-year-old high school student whose father was a physician and whose mother was an artist. His mother had a remote history of depression prior to Billy’s birth, and his paternal grandmother had a psychotic depression that was responsive to ECT. At age 13, Billy told his father that he had thoughts of jumping off something high. The family persuaded him to enter therapy, which he did from ages 13 to 15. He never took medication. He attended a private school, where he was doing well, although his homework was frequently late. He scored 1400 on the SAT and received early college acceptance. He did not smoke, drink, or take drugs.
His parents did not see him as depressed. He was well liked and had a girlfriend. As he once told his mother, “I’m not the most popular kid, but there’s no one who doesn’t like me.” The week of his suicide he was behind on a school paper and could not push himself to complete it. After arguing with his mother, he told her, “All I can think about is death.” Since the late paper was about the Space Shuttle Challenger disaster, she did not appreciate any suicidal intent.
The following day, Billy did not show up at school. He was seen jumping from the bridge later that afternoon wearing a backpack. At his funeral, the entire student body turned out.
Melissa
Melissa was a 49-year-old single woman with schizophrenia who lived at a board-and-care home in San Francisco, where one of the authors (M.B.) was the house doctor. She was raised in Kansas, the youngest of four children; her father, who may have been mentally ill, left the family when she was 6 years old. Melissa completed high school and some college in San Francisco and held various jobs, including with the telephone company, secretarial agencies, and the Department of Social Services. Her first psychotic break occurred at age 27. She had approximately 10 hospitalizations over the next 12 years. She made five suicide attempts by overdose during this time, plus two trips to the Golden Gate Bridge.
At age 34, she had a daughter, who was adopted by her sister. She entered the board-and-care home at age 39 and did well for 10 years. She had periodic exacerbations of her auditory hallucinations but no hospitalizations. After this period of stability, she had three hospitalizations within a year and a half. After her third hospitalization, she said, “I’m sick and tired of everything. I wish I could throw myself in front of the BART train.” After her discharge, she began a trial of clozapine, at that time the newest and most promising of the antipsychotic medications. She experienced many side effects, and she talked of being “over the hill” and feeling hopeless about her continuing hallucinations.
One month shy of her 50th birthday, she took a bus to the Golden Gate Bridge and jumped. She left her Social Security check and a note for her daughter.
Steve
Steve committed suicide at age 46, leaving behind his wife of 10 years and two young children. Three years before his death, he earned $1 billion for his investors and was recognized in financial publications.
Steve was raised in an affluent area north of the Golden Gate Bridge. His father was a corporate attorney with depression, and his mother was described as rejecting and critical. His parents divorced when he was 17, and his father’s career went downhill from there, with financial losses, alcoholism, and depression. Steve put himself through college, graduating magna cum laude, and completed graduate school in engineering at a top university.
He met his wife at college. They dated for 6 years and married when he was 33 and she 29. Six years later, the first of their two children was born. Steve did well in the financial industry. He was outgoing and social and very successful—“the last guy to have depression,” according to his wife. During the dot-com crash his investments did not do well, and he was fired. He had many offers in the subsequent years, but nothing seemed to fit.
Steve was seeing a psychiatrist on a regular basis during the last 5 years of his life. He was being treated for anxiety, depression, and alcoholism. His drinking had escalated after his job loss. There were periods of alcohol abuse and inappropriate use of prescribed medications.
In the last year of his life his psychiatric sessions were permeated with depressive themes—“blown opportunities,” “washed up,” “so much pressure,” “don’t think there’s a place for me.” During the 2 days before his death, he did not sleep and was described by his wife as anxious, teary, and restless. He saw his psychiatrist the day before his death and denied being suicidal, saying he could never do that to his children.
Steve left the house late that night and drove to the Golden Gate Bridge, crossing over the northern side and returning to stop mid-bridge. He jumped at 2 a.m., facing away from the city, toward the Pacific Ocean.
He left a note to his wife telling her how much he loved her and the children and saying, “I wish I had been stronger and better able to handle life’s pressures.”
Why the Golden Gate Bridge?
What attracted these three individuals to the Golden Gate Bridge? In the case of Billy, his mother reports that he was always fascinated by heights. Melissa had made several trips to the bridge. Steve’s wife said that her husband loved the bay and loved to sail. She believed the bridge was a logical choice to give him “freedom from his pain.”
The Golden Gate Bridge is an iconic suicide magnet. For some, the bridge is an easily accessible site—pedestrian access, a 4-foot railing, a bus stop, and a parking lot. For others, the bridge is a romantic final exit. Some believe bridge suicide is a painless death. One jumper reportedly left a note on the bridge reading, “Why do you make it so easy?”
The first author is the medical director at one of the hospitals closest to the bridge. From 2005 to 2008, he interviewed 63 individuals who had threatened to go to the bridge to commit suicide (49 of them were male; their mean age was 38 years, with a range from 18 to 72). The reasons they gave for selecting the bridge included “accessible/easy” (N=36), “romantic” (N=15), “painless” (N=6), and other reasons listed as “not categorized” (N=16). Representative of the “accessible/easy” category were comments such as “didn’t have a gun,” “close to my house,” and “a quick way to go.” Responses in the “romantic” category included “looks so majestic,” “the only golden way of getting into heaven,” and “you’re with all those people who jumped before.” Responses in the “painless” category included “they claim you don’t feel nothing” and “it would be over in a matter of seconds.” The “not categorized” responses included “don’t make no difference,” “tired of life,” and “isn’t that what most people do?”
There is a misconception that jumping to one’s death from a bridge into a body of water is painless. Jumpers from the Golden Gate Bridge fall over 200 feet and hit the water in 4 seconds at 75 mph. They die from massive cardiothoracic and CNS injuries or by drowning.
The fatality rate is about 99%. The first author interviewed three of the 28 known survivors. One survivor wrote that he had previously tried pills and alcohol but wanted something definitive. “I had to do something that was going to work. The statistics were pretty good that I would die and never be found. That’s really what I wanted, to be lost and never found.” Another survivor also had tried pills previously and went to the bridge because it was “for sure.”
A third male jump survivor said, “It’s the easiest way to die.… It’s beautiful, the only bridge I could get to from my house.… My disease was driving me nuts … voices were saying you must die.… I’m just tired of fighting this … I’m tired of being sick.… I figured if I jumped I’d just die.”
A 22-year-old depressed man who was taken twice from the Golden Gate Bridge in 2009 and hospitalized but did go on to commit suicide from the bridge told the first author that it was “scenic … a place to commit suicide.”
Rosen
(2) interviewed six bridge survivors. All of them said their suicide plans involved only the Golden Gate Bridge. In explaining their choice of the bridge, their comments included “an affinity between me, the Golden Gate Bridge, and death,” “entering the golden doors,” “certain death in a painless way,” and “notorious fame.”
Demographic Characteristics of Bridge Suicides
The Golden Gate Bridge is the most popular suicide site in the world.
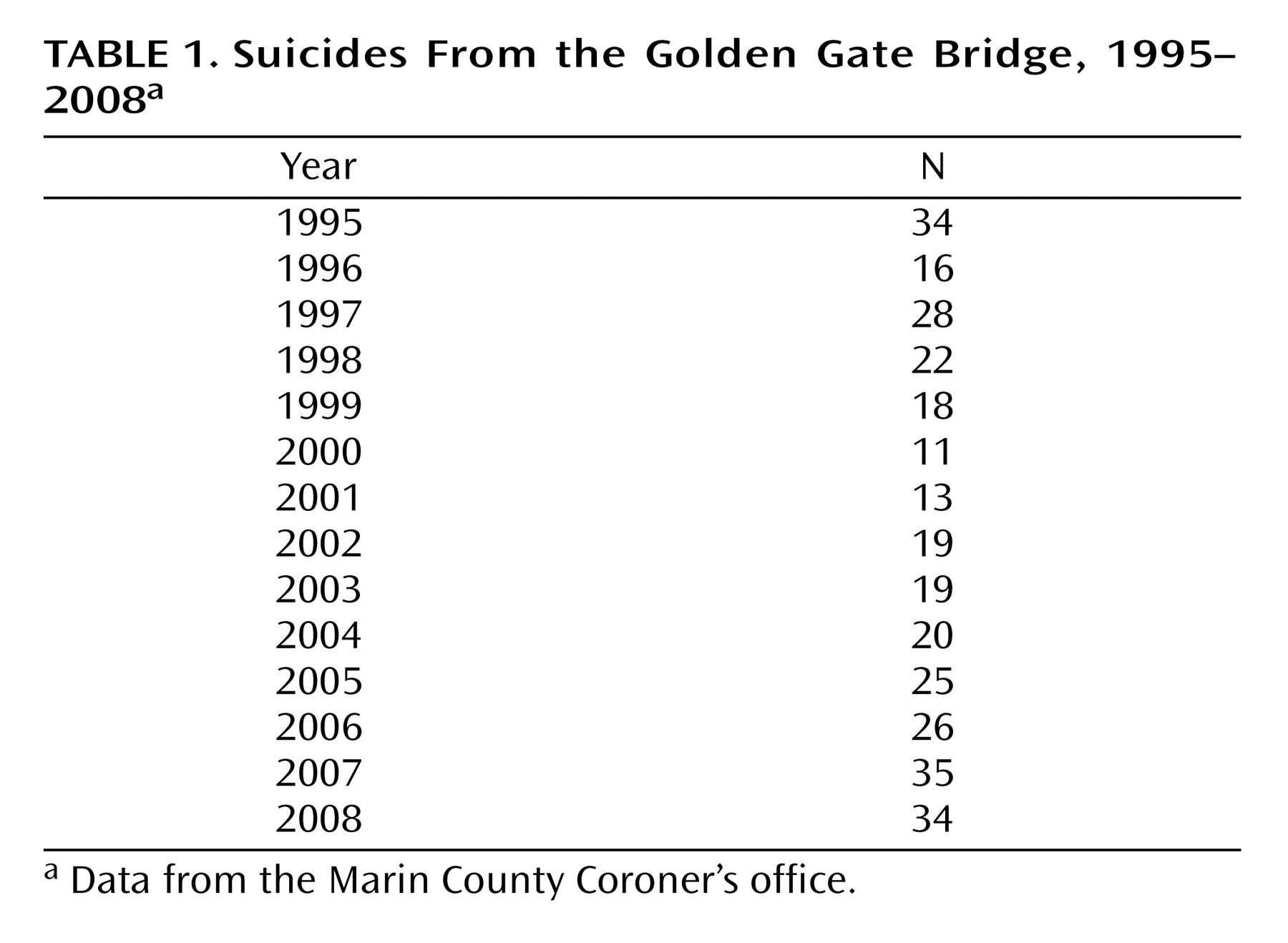
Table 1 presents data from the Marin County Coroner’s office on bridge suicides for the past 14 years. The toll is about two deaths per month, over 20 annually. The highest number in recent years was in 2007, with 35 deaths, but in actuality there were four more deaths based on witnessed jumps and surveillance camera records.
A report on data from the Centers for Disease Control and Prevention through 2005
(3) lists suicide as the 11th leading cause of death in the United States. Of the 32,637 deaths by suicide in 2005, 683 were by falls—2.1% or 0.2 per 100,000 population. The report does not distinguish bridge suicides from other falls from heights.
We reviewed data from the Marin County Coroner’s office (unpublished 2006 data) to examine demographic characteristics of bridge jumpers from 1995 through 2005. In that 11-year period, 225 bodies were recovered. The majority were male (74%) and white (82%). Ages ranged from 14 to 85 with a median of 40. Overall, 55% had never married, 23% were divorced, and 21% were married.
Those who commit suicide from the Golden Gate Bridge do not appear to be a more mentally ill population than suicides in general. The Marin County Coroner’s data from 1995 to 2005 indicate that approximately 40% were under psychiatric care at the time of their deaths. Twenty-two percent had made prior attempts, and one-quarter left suicide notes. The majority were believed to be employed, but we do not have firm data on employment.
Bridge suicides are committed by local residents. The Coroner’s data for “last known hometown” indicate that 87% lived in the nine counties adjacent to the bridge, with San Francisco County representing 30% of the sample. It is commonly believed that people come from all over to jump from the Golden Gate Bridge. In fact, only 5% of jumpers in the 1995–2005 period were non-Californians. This local phenomenon is mirrored at Niagara Falls, another tourist attraction and suicide magnet. A study of the period between 1978 and 1988 found that the 141 individuals who committed suicide at Niagara Falls lived within a 10-mile radius, in the United States (N=60) or Canada (N=81)
(4) .
Discussion of Cases
Golden Gate Bridge jumpers come from all walks of life. While depression is the most common cause of suicide, many jumpers act impulsively as a consequence of acute stress, shame, humiliation, rejection, or other trauma. Jumpers have included a county medical society president, a pastor of a Lutheran church, a president of the Oakland Real Estate Board, the founder of Victoria’s Secret, and the son of President Kennedy’s press secretary.
Our cases include an 18-year-old male adolescent, a 49-year-old mentally ill woman, and a 46-year-old married man. They all chose to end their lives at the Golden Gate Bridge.
Billy
Suicide by young people is especially tragic. Suicide is the third leading cause of death among 15- to 24-year-olds in the United States. In the Coroner’s 1995–2005 survey, suicide among those under age 24 accounted for 34 of 225 deaths (15%).
Billy’s profile does not include many of the predictive factors for adolescent suicide
(5), such as prior attempts, mood disorder, substance abuse, chaotic family life, recent loss of family or friends, hopelessness, and social isolation. In fact, the only areas where he does fit is male sex, Caucasian race, family history of depression, and experience of a recent stressor.
No one expected Billy to go to the bridge that day. As his best friend later wrote to one of the city papers as well as the mayor and the Golden Gate Bridge Board of Directors, Billy’s life provided more reasons for him to be happy than to be suicidal. “Why, then, did he jump?” asked Billy’s friend. “The only explanation I can find is that he never stopped to think it through. He didn’t tell anyone and he didn’t leave a note.” His friend’s comments underline the impulsive nature of Billy’s suicide. We should add that adolescents are especially prone to suggestion and copycat behavior, but we are unaware of any recent deaths among Billy’s peers.
Melissa
The prevalence of suicide among patients with schizophrenia is estimated to be as high as 10%
(6) . Melissa had been ill for more than 20 years, but her death was a surprise. She had many protective factors. She was living in a supportive setting. Her mother and sister lived in the neighborhood. She was able to visit her daughter, who was in her sister’s custody. She did not abuse alcohol or drugs. She was attending a day care center and was being seen regularly by the house psychiatrist, who led groups and monitored medications. The home was a lovely Victorian mansion where Melissa lived for over 10 years with 25 other residents as well as the owners and their children.
Melissa was also in good health. She was on the newest antipsychotic, clozapine, which has been shown to reduce the risk of suicide
(7) . However, she had been hospitalized three times in the last year and a half of her life. The most recent admission preceded her death by 5 months. She was depressed and felt hopeless, discouraged that the new “miracle drug” had not stopped the voices, which repeated “Hosanna” to her. Another resident had committed suicide that year. Melissa’s relationship with her boyfriend was rocky. She told him her plans; he told no one.
Steve
Depression and substance abuse are significant risk factors for suicide. Steve is the most typical of those who commit suicide from the bridge: male, white, middle-aged, depressed, drinking—all factors associated with an increased risk of suicide
(8) .
Steve’s wife reports that when they met in college, he did not drink. With the loss of his job, drinking and anxiety medications became problematic. At the end of his life he was attempting to withdraw from alcohol and benzodiazepines, but on the night of his death he was drinking. His ongoing therapy indicated a depressive disorder with themes of failure, low self-esteem, and shame.
He was unable to find work after a 4-year period of unemployment. One could conjecture that he had a narcissistic character style, not allowing him to accept a position below his self-image. Steve’s death was a product of many currents—depression, substance abuse, and possible character pathology and impulsivity.
Steve left his car and jumped from the west side facing the ocean, unlike the more than 80% of people who jump facing the city, perhaps taking a last look at civilization. The sidewalk on the east side has longer hours and both pedestrian and bicycle access, while the sidewalk on the west side has limited hours and only bicycle access.
Prevention
The cases of Billy, Melissa, and Steve highlight the tragedy of the many lives lost at the Golden Gate Bridge, and this tragedy raises the question of whether suicides from the bridge are preventable. There is little debate that barriers are effective in reducing suicides at a given location. Deterrents at other monuments, such as the Eiffel Tower, the Empire State Building, and the Harbor Bridge in Sydney, Australia, have virtually eliminated suicides at these sites. However, it is not as clear whether barriers would prevent suicides or instead divert individuals to other locations or methods, leaving the total number of suicides unchanged. Below we examine the evidence as to whether a barrier on the Golden Gate Bridge would likely be effective.
It is difficult to evaluate the efficacy of suicide barriers. All studies of barriers are necessarily observational. Also, in all published studies, suicides at the studied site have constituted a low proportion of total suicides in the surrounding area, making it difficult to determine whether a barrier reduced the overall suicide rate. However, there is an extensive literature on suicide prevention through the reduction of access to lethal means, and this literature can provide insight into the potential efficacy of suicide prevention barriers.
Many observational studies suggest that reducing access to lethal means is an effective strategy in reducing suicide. For example, Kreitman
(9) examined the effect of a change in the gas supplied to homes on the suicide rate in England. When lethal coal gas was used, one-third of suicides in England were due to asphyxiation by this gas. After nonlethal natural gas was substituted, the suicide rate in England fell by over 25%. Kreitman concluded that this drop in the national suicide rate was a direct result of the change in the lethality of the gas. Gunnell et al.
(10) found a 50% reduction over 10 years in the suicide rate in Sri Lanka after several highly lethal pesticides were banned. In a 2006 systematic review of suicide prevention strategies conducted by experts from 15 countries
(11), the authors found that reducing access to lethal means was an effective way to prevent suicide. The overall efficacy of means reduction supports the hypothesis that a suicide barrier would also be effective in reducing suicide.
In addition to the data on means reduction, there are some data specifically about suicide barriers. In 1985, a suicide prevention barrier was built on the Duke Ellington Memorial Bridge in Washington, D.C. In the 7 years before the barrier was built, 24 people committed suicide at the site, whereas only one person died by suicide in the 5 years after. Although the nearby Taft Bridge is visible from the Ellington Bridge, has no barrier, and is a short walk away, there was no increase in suicides from the Taft Bridge following the construction of the Ellington barrier. In addition, there was a significant decrease in the suicide rate in Washington, D.C.
(12) . However, this decrease (from an average of 76.5 to 71 people a year) was greater than the annual number of people who jumped from the Ellington Bridge. It is possible that the Ellington Bridge barrier contributed to the decrease in total suicides, but it is also possible that other factors contributed to or accounted for the decrease.
Another set of data comes from a barrier built in 1983 on the Augusta River Bridge in Maine, where 14 people had previously jumped to their deaths. The barrier eliminated suicides from the bridge. A study of suicides in the area during the two decades before and after installation of the barrier
(13) found no increase in jumping from nearby high structures, and the city of Augusta had a greater reduction in its suicide rate than the reduction seen in the surrounding area during the same period. Another example is the safety net installed in 1998 at Muenster Terrace in Bern, Switzerland, a former suicide “hot spot” in that country. There were no further suicides from the site even though the net did not completely cover the terrace and it was still possible, although more difficult, to jump from the site. There are two other high bridges within a 5-minute walk of Muenster Terrace, but there was no increase in jumps off other high structures in the city. After the installation of the net, there was a significant reduction in jumping fatalities in Bern
(14) . Similar to the partial net in Bern, a barrier was installed in 1998 on the Clifton Suspension Bridge in Bristol, England. Even though the barrier does not cover the entire bridge, it halved the number of suicides at that site (from 8.2 to 4 a year), and no increase was seen in jumps from surrounding structures
(15) . These four examples suggest that constructing a barrier does not divert suicidal individuals to jump off other high structures and possibly also reduces total suicides.
As opposed to the previous examples in which a barrier was newly constructed, Beautrais
(16) looked at an example of a bridge at which a suicide barrier was removed. Comparing the 3 years before and after the removal of the barrier, the author found that suicides increased from three with the barrier in place to 15 after it was removed—a statistically significant result. However, the overall rate of suicide by jumping in the city did not change, as jumping deaths from other structures decreased—although this decrease was not statistically significant.
Reisch et al.
(17) examined the association between access to jumping sites and suicide rate. They conducted an analysis of suicide rates throughout Switzerland, comparing areas with and without high bridges. They found lower suicide rates in areas without high bridges. The authors concluded that two-thirds of suicides from high bridges would be prevented if no bridge were available and that only one-third of people who died by jumping would be expected to substitute a different method.
Overall, the data on barriers at jumping sites show that they are effective in reducing suicides from the site itself. In addition, no study has found an increase in suicides from other nearby structures after a barrier is built. Finally, some studies have found a reduction in the local suicide rate after the construction of a barrier, although no study has found a statistically significant reduction.
There are some data specifically about the Golden Gate Bridge. In 1978, Seiden
(18) studied people who had been physically restrained from jumping off the bridge by the California Highway Patrol or workers on the bridge. He traced 515 people who had attempted to jump off the bridge between 1937 and 1971. As of 1978, he found that 94% either were still alive or had died of natural causes, and only 6% had committed suicide or died in accidents suggestive of suicide. His study supports the idea that suicide from the Golden Gate Bridge is preventable; that is, if someone is prevented from jumping off the Golden Gate Bridge, they are not likely to go on to commit suicide elsewhere or in the future.
We have several hypotheses for how a suicide barrier at the Golden Gate Bridge might work to prevent suicide. The first is that a barrier would reduce access to lethal means, and this is an effective method of suicide prevention. The second is that given the high lethality of jumping from the Golden Gate Bridge, even if some people are diverted to another method, the attempt is less likely to be lethal, and they are more likely to survive. A third, proposed by Reisch and Michel
(14) is that a barrier may be interpreted by suicidal individuals as “a sign of care” and possibly reduce their despair. Finally, and most speculatively, there is the hypothesis that certain sites become “suicide magnets” and may even catalyze or amplify suicidal feelings in vulnerable individuals. Glenn
(19) has written about suicide magnets: easily accessible, romanticized places that become associated with suicide in the public mind.
Evidence that the Golden Gate Bridge serves as a suicide magnet is provided by Seiden and Spence’s study
(20) of individuals who jumped from either the Golden Gate Bridge or the Bay Bridge, both of which connect to San Francisco. The bridges were built within 1 year of each other, have similar heights, and are similarly lethal to jumpers. Seiden and Spence looked at individuals who drove onto either bridge to kill themselves. (They excluded suicides in which the person walked onto either bridge, as the Golden Gate Bridge has pedestrian access while the Bay Bridge does not.) They found that between 1937 and 1979, 58 people drove across the Bay Bridge to commit suicide from the Golden Gate Bridge. However, no one drove across the Golden Gate Bridge to commit suicide from the Bay Bridge. This suggests that the Golden Gate Bridge has a powerful association with suicide in the minds of some individuals, to the extent that they would drive over one potentially lethal bridge to die at another.
Given the suggestible nature of suicide
(19) and the powerful association of the Golden Gate Bridge and suicide, it is possible that the Golden Gate Bridge and other suicide “icons” not only function as easily accessible, highly lethal spots for suicide but also may trigger or amplify suicidal feelings in vulnerable individuals. If so, a barrier at such a site could be particularly effective in reducing suicide.
While it is impossible to make a conclusive statement about the potential efficacy of a suicide barrier on the Golden Gate Bridge, the strong evidence that reducing access to lethal means prevents suicide supports the hypothesis that a suicide barrier would be effective. In addition, the limited data specifically regarding barriers also support the hypothesis that a barrier would be effective.
Concluding Comments
A suicide barrier might have saved the lives of Billy, Melissa, and Steve. Here is what one survivor had to say about his walk to the middle of the span:
I just looked out over the water to the city and it was beautiful. I felt that this was the right time and place to kill myself. The last thing I saw leave the bridge was my hands. It was at that time that I realized what a stupid thing I was doing. And there was nothing I could do but fall. The next thing I knew I was in the water hoping that someone would save me, saying, “Please God save me, somebody save me.” It was incredible how quickly I had decided that I wanted to live once I realized everything that I was going to lose, my wife, my daughter, the rest of my family.
He is currently in his thirtieth year of marriage. He is a high school teacher and part-time coach. His daughter is an elementary school teacher.
Postscript
After years of effort on the part of multiple organizations, the Psychiatric Foundation of Northern California, with the support of its task force, family members of suicide victims, mental health advocates, the press, and others, persuaded the 19-member Golden Gate Bridge Board of Directors to approve a barrier. The public was divided because of aesthetic issues, financial concerns, and ignorance about suicide. On October 10, 2008, the Board voted 14 to 1 to build a flexible stainless steel net below the bridge. This approval is an important first step. Construction of the net is pending, however, until further environmental studies are completed and a funding plan developed and approved. No start date for construction has been established.