Patients with PTSD from experiences during the World Trade Center attack responded better to paroxetine, up to 50 mg/day, than placebo over 10 weeks of exposure therapy that included weekly 90-minute guided imagery sessions and cognitive-behavioral exercises. By week 10, 42% of patients in the paroxetine group remitted, compared with 17% in the placebo group. The differences did not persist for patients who continued therapies beyond 10 weeks; by week 22, the remission rate was 45% for both treatments among those remaining in the study.
Abstract
Objective:
Selective serotonin reuptake inhibitors (SSRIs) are often recommended in combination with established cognitive-behavioral therapies (CBTs) for posttraumatic stress disorder (PTSD), but combined initial treatment of PTSD has not been studied under controlled conditions. There are also few studies of either SSRIs or CBT in treating PTSD related to terrorism. The authors compared prolonged exposure therapy (a CBT) plus paroxetine (an SSRI) with prolonged exposure plus placebo in the treatment of terrorism-related PTSD.
Method:
Adult survivors of the World Trade Center attack of September 11, 2001, with PTSD were randomly assigned to 10 weeks of treatment with prolonged exposure (10 sessions) plus paroxetine (N=19) or prolonged exposure plus placebo (N=18). After week 10, patients discontinued prolonged exposure and were offered 12 additional weeks of continued randomized treatment.
Results:
Patients treated with prolonged exposure plus paroxetine experienced significantly greater improvement in PTSD symptoms (incidence rate ratio=0.50, 95% CI=0.30–0.85) and remission status (odds ratio=12.6, 95% CI=1.23–129) during 10 weeks of combined treatment than patients treated with prolonged exposure plus placebo. Response rate and quality of life were also significantly more improved with combined treatment. The subset of patients who continued randomized treatment for 12 additional weeks showed no group differences.
Conclusions:
Initial treatment with paroxetine plus prolonged exposure was more efficacious than prolonged exposure plus placebo for PTSD related to the World Trade Center attack. Combined treatment medication and prolonged exposure therapy deserves further study in larger samples with diverse forms of PTSD and over longer follow-up periods.
Posttraumatic stress disorder (PTSD) has a lifetime prevalence of 8%–12% and is associated with significant comorbidity and impaired quality of life (1, 2). Traumas commonly associated with PTSD include combat, rape, and natural disasters, but there has been relatively little study of treatment for terrorism-related PTSD. Six months after September 11, 2001, some 91,000 New York City residents were estimated to have PTSD related to the World Trade Center attack (3). To date, only one single randomized clinical trial has assessed treatment for PTSD related to this attack, and it was limited to rescue workers (4).
Although the selective serotonin reuptake inhibitors (SSRIs) paroxetine and sertraline have a U.S. Food and Drug Administration indication for PTSD based on efficacy in several randomized clinical trials (5–7), the role of medication in the treatment of PTSD remains unclear (8–10). Some PTSD guidelines recommend SSRIs among first-line treatments for the disorder (8, 10), but others question the magnitude of treatment response and recommend that SSRIs be a second-line treatment or adjunct to cognitive-behavioral therapy (CBT) (9, 10). Trauma-focused CBT approaches, such as prolonged exposure therapy, have strong empirical support based on more than two dozen randomized clinical trials (10, 11), but remission rates among those who complete therapy have been under 50% in some studies (12). Because medication and CBT monotherapies each have limitations and yet are very different approaches, combining these treatments might maximize efficacy (13).
No randomized clinical trials, to our knowledge, have studied combined treatment with medication and trauma-focused CBT for PTSD from the outset of treatment in a sample that was not preselected for treatment resistance. One small trial (N=10) and a subgroup analysis of a second trial reported an advantage for combined SSRI and CBT treatment over SSRI monotherapy for adults with PTSD who did not respond to pharmacotherapy (14, 15). Another small study of patients who remained unremitted after 8 weeks of CBT (N=23) reported that augmentation with an SSRI was not superior to augmentation with placebo (16). However, a meta-analysis of 11 studies across all anxiety disorders found combined CBT and medication to be significantly more effective than CBT and placebo at the end of treatment but not at the 6-month follow-up assessment (17), supporting the need for further study of this issue in the treatment of PTSD.
The purpose of the present study was to compare combined medication and CBT with the widely recommended first-line treatment of CBT alone in the initial treatment of PTSD. Enrollment was limited to persons with PTSD related to the World Trade Center attack in order to obtain a sample that would be relatively homogeneous with respect to the stressor and to learn more about the treatment of PTSD related to terrorism. The primary hypothesis was that 10 weeks of combined treatment with prolonged exposure therapy and paroxetine compared with prolonged exposure and placebo would be more efficacious in reducing symptoms and increasing remission rates in persons with PTSD related to the World Trade Center attack.
Method
Design
This study was approved by an institutional review board and conducted at the Anxiety Disorders Clinic of New York State Psychiatric Institute/Columbia University from December 2004 to February 2009. After participants received a complete description of the study, they provided written informed consent. Individuals with chronic PTSD related to the World Trade Center attack were randomly assigned to 10 weeks of double-blind treatment with prolonged exposure therapy plus paroxetine or prolonged exposure therapy plus placebo. To examine maintenance of gains, those who completed 10 weeks of treatment were offered 12 additional weeks of continued double-blind treatment with paroxetine or placebo alone.
Participants
The sample consisted of 37 adults who were referred by clinicians, responded to advertisements, or responded to direct mail to individuals who had either sought help for World Trade Center attack-related difficulties from the Mental Health Association of New York City or participated in the World Trade Center Health Registry and screened positive for possible PTSD (score of ≥50 on the PTSD Checklist [18]).
Eligibility was determined by clinical interview, the Clinician-Administered PTSD Scale (CAPS [19]), and DSM-IV criteria (20, 21). Participants were ages 18–70 years, with a principal DSM-IV diagnosis of PTSD that was related to the World Trade Center attack and a symptom duration ≥3 months of at least moderate severity (CAPS score ≥45). Exclusion criteria were prominent suicidal ideation; current psychotic disorder; unstable medical illness; pregnancy or nursing; alcohol or substance use disorder in the past 3 months; history of seizure disorder; unwillingness to use contraception (for women of childbearing potential); conditions that contraindicated study treatments (such as an unsuccessful trial or intolerance of paroxetine, three unsuccessful SSRI trials, or an unsuccessful trial of prolonged exposure therapy); and use of psychotropic medication during the 2 weeks (4 weeks for fluoxetine or monoamine oxidase inhibitors) before randomization, except zolpidem for insomnia.
Randomization and Blinding
Participants were randomly assigned in blocks of 10 to prolonged exposure therapy plus paroxetine or prolonged exposure therapy plus matching pill placebo by the data manager, who had no patient contact. Controlled-release paroxetine (22) and matching placebo tablets were provided by GlaxoSmithKline (Brentford, United Kingdom). The tablets were packed in bottles, consecutively numbered for each patient according to the randomization schedule, by a pharmacist with no patient contact. Each patient's allocation was concealed from all research personnel for the full duration of the patient's participation in the study. To minimize risk of unblinding of independent evaluators in particular, secondary outcome measures of depressive symptoms and adverse effects were administered by pharmacotherapists.
Treatments
Paroxetine and placebo were administered by psychiatrists experienced in pharmacotherapy for PTSD. Visits were 30 minutes weekly for 6 weeks, every 2 weeks for 4 weeks, and then every 4 weeks. Pharmacotherapists offered support, monitored compliance using pill counts, and reviewed symptoms. They also prescribed paroxetine at a dosage of 12.5 mg/day, or matching placebo, for 1 week, then 25 mg/day for 3 weeks, and then increased the dosage as tolerated to a maximum of 50 mg/day.
Prolonged exposure therapy uses guided exposure to traumatic memories and situations to enhance emotional processing. In this study, it was conducted in 10 weekly 90-minute sessions using methods described by Foa and Rothbaum (23). Therapy sessions were conducted by psychiatrists and doctoral-level psychologists experienced in CBT who completed a 2- to 4-day training course as well as a supervised training case. Therapist adherence was monitored in individual and group supervision. All sessions were videotaped, and 10% were randomly selected and reviewed by two independent raters using a treatment fidelity manual. Therapists completed 89% of essential components. Three sessions were rated independently by both raters, and interrater reliability (percentage agreement) was 0.88.
Assessments
Independent evaluators were master's- or doctoral-level clinicians. They conducted major assessments at weeks 0, 5, and 10 and, for participants in the maintenance phase, at weeks 14, 18, and 22. PTSD severity was assessed using the CAPS and the 7-point Clinical Global Impressions of Change scale (CGI-C [24]) (ratings range from very much worse to very much improved).
Pharmacotherapists administered the 17-item Hamilton Depression Rating Scale (25) at major assessments and used a checklist (data available on request from the authors) to rate 29 potential adverse effects at every visit on a 0- to 3-point scale (none, mild, moderate, or severe). An adverse event was considered treatment-emergent if its severity at any point during the study was at least one point greater than that at baseline.
Patients completed the Quality of Life Enjoyment and Satisfaction Questionnaire (26), a reliable and valid measure of enjoyment and satisfaction in eight domains.
Statistical Analyses
Primary outcome variables were CAPS score and remission status at weeks 5 and 10. Remission is considered an important goal for treatment of PTSD (27), and it is particularly relevant for a study combining two efficacious treatments to maximize improvement. Remission was defined as a CAPS score ≤ 20 and a CGI-C score of 1 (very much improved). Treatment response was a secondary outcome measure, defined as a CGI-C score of 1 or 2 (much improved or very much improved).
Continuous variables were modeled using longitudinal mixed-effect analyses with appropriate link functions (28, 29). For instance, because CAPS scores were overdispersed (mean < variance) and had a right-skewed distribution, they were modeled using negative binomial distribution with log link function (30). Binary outcome variables were modeled using longitudinal logistic mixed-effect analyses (log mixed-effect models) (28, 29, 31).
All models included predictors of time, treatment, and time-by-treatment interactions as well as adjustment for baseline values transformed according to used link function. Participants were modeled as random factors, with temporal within-subject autoregressive (AR[1]) correlation structure. If the time-by-treatment interaction was not significant, the outcome variable was modeled using main effects of time and treatment, adjusted for the baseline CAPS score. Results are reported using incidence rate ratios (models with negative binomial link function) or odds ratios (models with logistic link function). Three-way interaction of baseline CAPS score-by-treatment-by-time in the model was used to assess the moderator effect of the dichotomized (above and below the median) baseline CAPS score on treatment over time.
Tests of main effects were considered significant at an alpha of 0.05, and tests of interaction terms were considered significant at an alpha of 0.15 (32). All tests were two-tailed and used intent-to-treat samples. Missing observations were investigated using logistic regression. Because no significant predictors of missingness were found, missing observations were assumed to be missing at random (i.e., no imputation methods were used). Analyses were performed using PROC GLIMMIX in the SAS software package (SAS Institute, Cary, N.C.).
Results
Sample
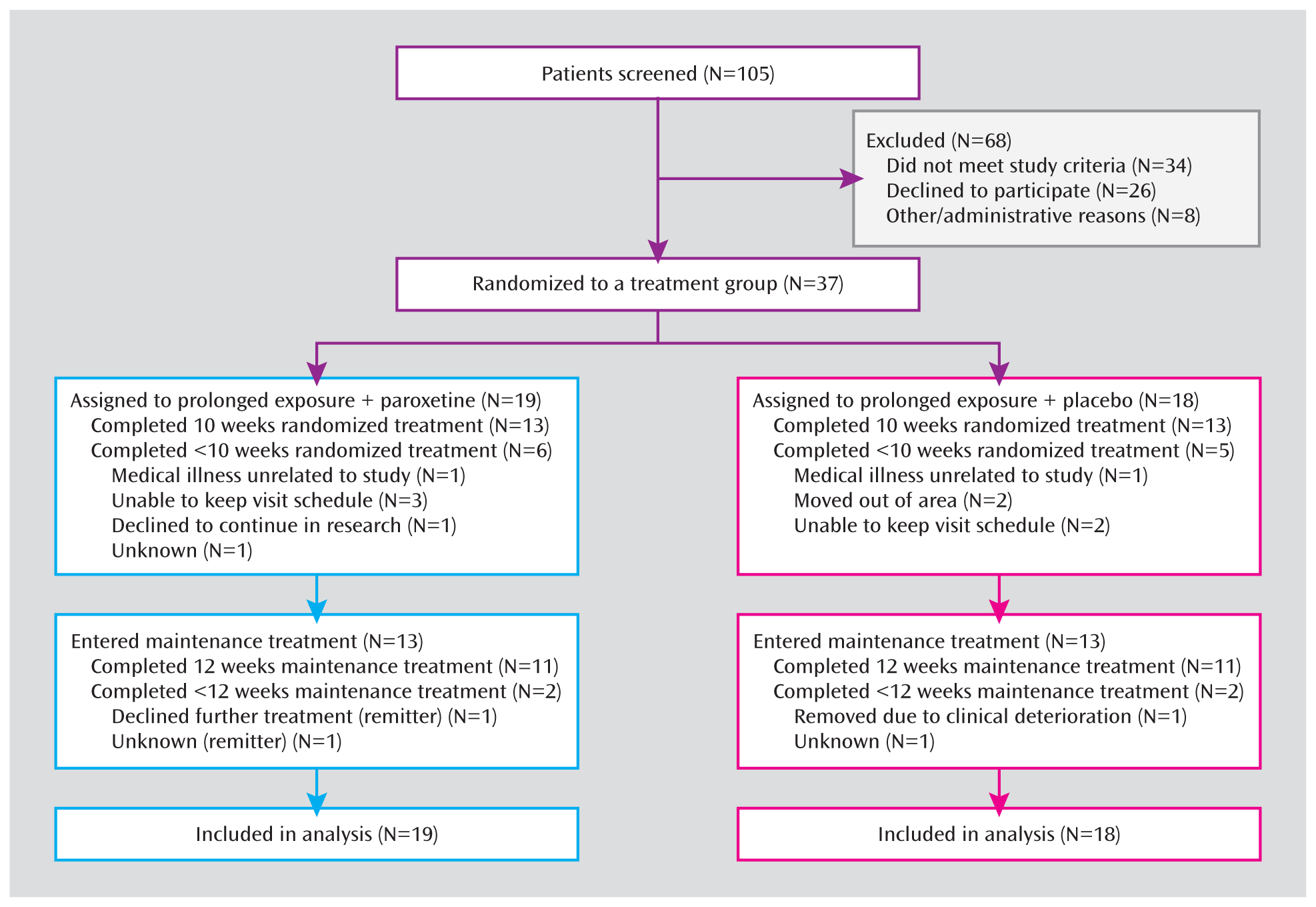
Figure 1 summarizes the flow of participants through the study. The paroxetine and placebo groups did not differ in rates of discontinuation prior to week 10 (six [31.6%] and five [27.8%] participants, respectively) or prior to week 22 (eight [42.1%] and seven [33.3%] participants, respectively). Participants who discontinued prematurely did not differ on baseline measures from those who completed each phase. After week 10, 13 participants continued receiving paroxetine and 13 continued to receive placebo, and 11 participants in each group completed the 12-week maintenance phase.
FIGURE 1. Flow Diagram of Study Participants With PTSD Related to the World Trade Center Attack
The randomized groups did not differ significantly in demographic or clinical characteristics, except for years of education (p=0.02) (Table 1). All participants reported having been in the vicinity of the World Trade Center at the time of the attack or building collapse (in the World Trade Center [N=8], in nearby lower Manhattan [N=24], arrived in immediate aftermath to help [N=5]). Thirty-one participants (83.8%) were emergently evacuated; 12 (32.4%) reported loss of an immediate family member or close friend; and 25 (67.6%) reported at least some prior treatment of the index episode of PTSD. Adequacy of prior PTSD treatment was not systematically documented, but of the 15 previously medicated individuals, only nine (three in the placebo group, six in the paroxetine group) reported any prior SSRI treatment, and of the 20 individuals reporting prior therapy, none reported an adequate course of ≥ 10 sessions of trauma-focused CBT. The most common current psychiatric comorbidities were mood disorders (N=25 [65.8%]), and treatment groups did not differ significantly in the rate of comorbidity or in the severity of PTSD or depressive symptoms at baseline.
TABLE 1. Baseline Demographic and Clinical Characteristics of Patients Treated With Combined Prolonged Exposure Therapy and Paroxetine or Prolonged Exposure Therapy Plus Placebo for PTSD Related to the World Trade Center Attack
Characteristic
Paroxetine Plus Prolonged Exposure Therapy (N=19)
Placebo Plus Prolonged Exposure Therapy (N=18)
N
%
N
%
Female
8
42.1
12
66.7
Marital status
Married
6
31.6
7
38.9
Single, never married
8
42.1
5
27.8
Divorced
5
26.3
6
33.3
Ethnicity/race
Caucasian
13
68.4
12
66.7
African American
4
21.1
1
5.6
Hispanic
1
5.3
4
22.2
Other
1
5.3
1
5.6
Employment
Full-time
6
31.6
5
27.8
Part-time/homemaker/retired
6
31.6
3
16.7
Unemployed/disabled
7
36.8
10
55.6
Comorbid diagnosis
Current axis I disorder
14
73.7
12
66.7
Current axis II disorder
2
10.5
4
22.2
PTSD episode prior to September 11, 2001
2
10.5
1
5.6
History of trauma prior to September 11, 2001
5
26.3
9
50.0
Psychotherapy for PTSD after September 11, 2001
10
52.6
10
55.6
Pharmacotherapy for PTSD after September 11, 2001
8
42.1
7
38.9
Any treatment for PTSD after September 11, 2001
13
68.4
12
66.7
Mean
SD
Mean
SD
Age (years)
49.1
8.0
51.5
8.0
Education (years)
15.5
1.6
14.2
1.7
Age at PTSD onset (years)
43.3
8.2
44.3
10.3
Duration of PTSD (years)
5.8
2.7
7.2
8.3
Clinician-Administered PTSD Scale score
72.6
12.9
65.4
12.8
Hamilton Depression Rating Scale score
16.9
4.9
16.6
4.9
Primary Outcome Measures
Interactions between time (from week 5 to week 10) and treatment were not significant, reflecting parallel improvement in both groups from week 5 to week 10, and thus only change over time and treatment group effect were estimated. CAPS scores for each group improved significantly from randomization to week 10 (p<0.001), with significantly greater improvement in the combined treatment group than in the prolonged exposure plus placebo group (p=0.01 [Table 2, Figure 2]). Participants in the combined treatment group had modeled CAPS scores at weeks 5 and 10 that were one-half (incident rate ratio=0.50) the scores of participants in the prolonged exposure plus placebo group. Analysis of dichotomized baseline CAPS scores did not provide evidence for baseline severity moderating group differences in treatment outcome.
TABLE 2. Effects of Treatment and Time on Observed Values of Outcome Measures at Weeks 5 and 10 Among Patients Treated With Combined Prolonged Exposure Therapy and Paroxetine or Prolonged Exposure Therapy Plus Placebo for PTSD Related to the World Trade Center Attack
Quality of Life Enjoyment and Satisfaction Questionnaire scoref
1.4
1.10–1.82
0.02
0.88
0.76–1.01
0.08
Baseline
16
47.1
11.0
16
45.4
18.5
Week 5
13
55.5
13.4
11
59.4
17.6
Week 10
9
67.9
12.7
10
54.8
22.3
a
Sample sizes vary by time point and measure as a result of attrition and missing data.
b
Incident rate ratios are computed for modeled continuous outcome variables with negative binomial distribution.
c
Odds ratios are computed for modeled dichotomous outcome variables.
d
Analyses revealed a significant two-way time-by-treatment interaction (p=0.09).
e
Nonsignificant two-way time-by-treatment interaction (p=0.20) was omitted from the model.
f
Higher scores represent better quality of life; analyses revealed a significant two-way time-by-treatment interaction (p=0.06).
Image (ajp_169_1_80_f02_.png) is missing or otherwise invalid.
FIGURE 2. Clinician-Administered PTSD Scale Scores During Acute Treatment With Prolonged Exposure Therapy Plus Paroxetine or Prolonged Exposure Therapy Plus Placebo Among Patients With PTSD Related to the World Trade Center Attacka
a Bars indicate standard deviation.
Remission in each group increased significantly over time (p<0.007), and remission was significantly more frequent in the combined treatment group (p=0.03 [Table 2, Figure 3]). Remission rates for the intent-to-treat sample at week 10 were 8/19 (42.1%) for combined treatment compared with 3/18 (16.7%) for prolonged exposure plus placebo. Modeled data showed that combined treatment increased the odds of remission at weeks 5 and 10 to 12.6 times that for prolonged exposure plus placebo. However, the wide 95% confidence interval (1.23–129) reflects limited precision of this estimate because of the small number of participants in the study.
Image (ajp_169_1_80_f03_.png) is missing or otherwise invalid.FIGURE 3. Remission Rates During Acute Treatment With Prolonged Exposure Therapy Plus Paroxetine or Prolonged Exposure Therapy Plus Placebo Among Patients With PTSD Related to the World Trade Center Attack
Secondary Outcomes
Secondary outcomes are presented in Table 2. Response rates for the intent-to-treat sample at week 10 were 12/19 (63.2%) for combined treatment and 7/18 (38.9%) for prolonged exposure plus placebo. Interactions between time (weeks 5 and 10) and treatment were significant for response status and quality of life outcomes, and thus the treatment group effect was different at each time point, and the effect of change over time was different for each treatment group. In the prolonged exposure plus placebo group, neither response status nor quality of life outcome had a significant treatment effect at week 5 or significant change from week 5 to week 10. The combined treatment group improved significantly in quality of life (p=0.02) and in response rate (p=0.04) at week 10 compared with the prolonged exposure plus placebo group. From week 5 to week 10, only the combined treatment group response rate improved significantly (p=0.02). Both groups' depression scores improved over time (p=0.04), with no significant treatment group effect.
Among participants who continued treatment with paroxetine (N=13) or placebo (N=13) during weeks 10–22, no outcome measures showed any significant improvement or group differences. In the paroxetine group, of the eight who had remitted by week 10, two discontinued treatment prematurely (both were in remission at the time of discontinuation), five remained in remission at week 22, and one was no longer in remission at week 22; of the five who had not remitted at week 10, one remitted by week 22. In the placebo group, the three individuals who had remitted by week 10 remained in remission at week 22; of the 10 who had not remitted at week 10, two discontinued prematurely, and two remitted by week 22. Among all those who completed the 10- to 22-week assessment, the week-22 remission rate was 45.5% (5/11) for each group, and mean CAPS scores were 30.4 (SD=30.7) for the paroxetine group and 27.9 (SD=21.1) for the placebo group, which were not significantly different. For further details regarding outcomes during the additional 12-week assessment period, see the data supplement accompanying the online edition of this article.
In the combined treatment group, the mean maximum daily dose of paroxetine attained for at least 1 week was 32.2 mg/day (SD=13.4) and did not differ significantly from the paroxetine equivalent of 36.8 mg/day (SD=12.1) in the placebo group. Treatment-emergent adverse events were numerically greater in the paroxetine group but did not differ significantly from those of the placebo group.
Discussion
Combined treatment with prolonged exposure therapy and paroxetine was superior to prolonged exposure and placebo in reducing the symptoms of PTSD related to the World Trade Center attack over 10 weeks of treatment. This finding offers the strongest evidence to date that combining trauma-focused CBT with medication may be a more efficacious initial treatment strategy than CBT alone for PTSD. Both primary outcome measures (CAPS score and remission rate) and secondary measures (response rate and quality of life) demonstrated significant advantages for combined treatment. Based on remission rates for each group at week 10, the number needed to treat is three (i.e., three patients would need to be treated with combined treatment to yield one additional remission during initial CBT treatment). Given the evidence supporting trauma-focused CBT as a treatment of choice for PTSD, the findings in this study advance the field by demonstrating that a combined treatment approach can further improve acute response. However, more investigation will be needed to determine whether these benefits persist.
The advantage of combined treatment with medication and CBT in the initial treatment of PTSD may reflect additive mechanisms. Prolonged exposure therapy is believed to act through learning, including basic processes of extinction of conditioned responses and reappraisal of cognitive schemas linked to the trauma (33). Paroxetine decreases presynaptic reuptake of serotonin, which may lead to stabilization of CNS circuits mediating hyperarousal and activation of memories by conditioned aversive stimuli.
The clinically meaningful within-group effect size for CAPS score in the prolonged exposure plus placebo group (Cohen's d=1.12) suggests a specific contribution of prolonged exposure therapy to treatment response in the combined treatment group. This is within the range reported for exposure therapy for PTSD in previous trials, although larger effects have been reported at some expert sites (34). Without a group controlling for nonspecific effects of prolonged exposure, this study could not determine the contribution of techniques specific to prolonged exposure therapy to treatment response in either group.
Outcomes for the prolonged exposure plus placebo group in this study could have been influenced by factors related to the study design and implementation. This study limited prolonged exposure therapy to the 10-week course established in previous trials, but a longer course continuing through weeks 10–22 might have produced greater improvement. Both treatments in this study appear to have been adequately implemented and tolerated, based on assessment of therapy tapes, paroxetine dosages, and attrition rates of 36.8% for combined treatment and 27.8% for prolonged exposure plus placebo, which are comparable to the 30.3% and 20.5% rates reported across all PTSD randomized trials of SSRIs and exposure therapy, respectively (35, 36). Features of study treatments that may have contributed to attrition include the confrontation of traumatic memories in prolonged exposure therapy and adverse effects of medication. This is the first report of efficacy for the controlled-release form of paroxetine for the treatment of PTSD, which yields slightly more stable plasma levels than the immediate-release form of the medication that has established efficacy for PTSD (22).
Features of the sample may also have affected outcome. Characteristics of persons with PTSD, such as avoidance behavior and loss of trust, may tend to increase attrition. Although most participants reported inadequate response to some prior treatment, which might suggest treatment resistance, few had received an adequate trial of an evidence-based treatment. Features specific to the World Trade Center attack also may have affected outcomes. The violence was both intentional and catastrophic, which tends to increase the severity of PTSD (37–39). Ongoing stressors related to high rates of personal loss, additional terrorist threats following the attack, and the downward spiral of consequences of chronic illness (job loss, family conflict, divorce) could have reduced treatment responsiveness. However, good prognostic factors include relatively high educational status and the fact that the index trauma was a single event in adulthood, which generally has a better treatment outcome than severe childhood trauma or the multiple traumatic exposures typical of combat- or abuse-related PTSD. Thus, on balance, we do not believe that this sample can be characterized as treatment resistant or uniquely distinct from other traumatized populations in treatment responsiveness. Yet the generalizability of these findings will need to be tested in other PTSD samples.
The sample was also distinguished by openness to trying both medication and CBT treatments, as was required by the study design. Persons with PTSD have been shown to have strong treatment preferences, especially favoring nonmedication treatments (40). Participants in this study may have been less compliant with their less-favored treatment than participants entering studies of a single treatment modality. Future studies of combined treatment should assess treatment preferences and their effect on outcome.
Over the 12 weeks after prolonged exposure therapy was discontinued and patients were maintained on double-blind paroxetine or placebo, no group differences were observed. Interpretation is subject to important limitations. The diminished sample size in this phase limited power to detect smaller effects, and patients who entered this phase were not a random selection, which may have further obscured treatment differences. Future studies with larger samples will need to address the important question of whether the initial advantage of combined treatment persists over time.
The primary limitation of this study is its relatively small sample. However, the full sample of 37 patients represents the largest randomized clinical trial to date among persons with World Trade Center-related PTSD. The findings of superiority for combined treatment diverge somewhat from those of Simon et al. (16), who conducted the one PTSD study that did not find an advantage for paroxetine over placebo augmentation among patients who did not remit with 8 weeks of prolonged exposure therapy. Design differences in that study included a smaller randomized sample (N=23), randomization of only those patients who remained symptomatic after a course of prolonged exposure therapy, and continued provision of prolonged exposure therapy during placebo-controlled augmentation, which could have obscured any drug-specific effects. Nevertheless, the remission rate for the paroxetine group in that study was more than double that of the placebo group (33% compared with 14%), although the effect was not statistically significant in the small sample. A methodological advantage shared by our study and the Simon et al. study is the incorporation of pill placebo as a control. None of the PTSD studies that have reported superiority of CBT augmentation of SSRIs over SSRI treatment alone incorporated any form of placebo therapy to control for nonspecific effects of CBT, such as therapist attention.
Our study findings support clinical consideration of combined treatment with paroxetine and prolonged exposure therapy at the outset for patients with PTSD because of superior efficacy for the initial treatment of PTSD symptoms. These advantages must be weighed against potential disadvantages of the greater cost of combined treatments, the risk of adverse effects of medication, and the risk that eventual discontinuation of medication might be associated with risk of relapse, which has been shown after discontinuation of SSRI monotherapy (41). Future studies should assess moderators of response to combined treatments and monotherapy, with the goal of developing clinically useful predictors of treatment selection. The finding of medication effects also underscores the importance of assessing the effect of concurrent medication use in any studies assessing psychosocial treatments for PTSD.
Patient Perspective
On September 11, 2001, “Mr. J,” a 35-year-old married man with two daughters, was working for a financial company at the World Trade Center. After the planes hit, he was evacuated from his building and eventually made his way to safety. He had no prior psychiatric history and recalls thinking—immediately after the event—that he would be fine if he resumed work and went back to his usual optimistic coping style. As time went by, however, he noticed that he had intrusive memories, was emotionally disconnected from his family, had trouble getting to work in downtown Manhattan, and was increasingly avoidant of trains and airports. By the time he presented for treatment, he had lost his job, his marriage had ended, and he had become distant from his children. He also reported feeling “panicky, anxious, and for the first time in [his] life, hopeless.”
Mr. J enrolled in the study, believing that it was his last chance to get help, and he threw himself into the prolonged exposure treatment with a deliberate seriousness. During imaginal exposure exercises, he described his September 11 experience with great affect: “I watched over and over as people jumped off the tower. I can still clearly see them—hear their bodies hitting the ground.” After evacuating from his building, he had remained by the towers, as others ran away, to wait for his close friend Peter to emerge. Suddenly, the tower collapsed, and he was overtaken by a choking cloud of white debris: “I put my newspaper around my face and dove under a car for cover. I was thinking, 'You are going to die,' and then I thought, 'Oh no, I cannot die like this, I have a 3-month-old who needs me,' and then I lost consciousness.” The next thing he remembered was a police officer pulling him out of the debris by his feet and yelling, “This one's still alive.” Others around him were dead, and he recalled seeing hundreds of women's shoes that must have been abandoned in the streets as people fled. When he finally got home that night, he cleaned up and went to Peter's house: “It was full of people crying and praying. Peter's wife was crying and asked me if Peter made it out. I lied and told her he was probably in a hospital, but after what I saw, I knew he was dead.” During the first imaginal exposure session, Mr. J was intensely distressed (subjective units of distress score=100), but his distress decreased with each retelling. Between sessions, he conscientiously completed his behavioral exposure exercises to confront his multiple avoidances. Afterward, he explained: “I'm a straightforward sort of person, and I liked this therapy because it was straightforward. You explained everything and told me exactly what to do. I did it, and I got a lot better.” He also received the study medication daily (he had been randomly assigned to paroxetine), which he tolerated without significant side effects. After 10 weeks of combined treatment, Mr. J was significantly improved, with minimal anxiety or avoidance symptoms: “I'm back to my old self. I can connect to my kids, planes do not scare me anymore, and I was even able to visit the memorial stone for Peter for the first time. I'm feeling optimistic again, and I think I can work in Manhattan without freaking out.”
Footnotes
Received Feb. 25, 2011; revisions received May 20 and June 17, 2011; accepted June 24, 2011.
GlaxoSmithKline provided the paroxetine and matching placebo tablets used in this study.
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS: Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 1994; 51:8–19
Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE: Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005; 62:617–627
Galea S, Vlahov D, Resnick H, Ahern J, Susser E, Gold J, Bucuvalas M, Kilpatrick D: Trends of probable post-traumatic stress disorder in New York City after the September 11 terrorist attacks. Am J Epidemiol 2003; 158:514–524
Difede J, Malta LS, Best S, Henn-Haase C, Metzler T, Bryant R, Marmar C: A randomized controlled clinical treatment trial for World Trade Center attack-related PTSD in disaster workers. J Nerv Ment Dis 2007; 195:861–865
Marshall RD, Beebe KL, Oldham M, Zaninelli R: Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001; 158:1982–1988
American Psychiatric Association: Practice Guideline for Treatment of Patients With Acute Stress Disorder and Posttraumatic Stress Disorder. Am J Psychiatry 2004; 161 (Nov suppl)
National Institute of Clinical Excellence: Posttraumatic Stress Disorder: The Management of PTSD in Adults and Children in Primary and Secondary Care. London, National Collaborating Centre for Mental Health, 2005 (http://guidance.nice.org/CG26)
Forbes D, Creamer M, Bisson JI, Cohen JA, Crow BE, Foa EB, Friedman MJ, Keane TM, Kudler HS, Ursano RJ: A guide to guidelines for the treatment of PTSD and related conditions. J Trauma Stress 2010; 23:537–552
Otto MW, Hinton D, Korbly NB, Chea A, Ba P, Gershuny BS, Pollack MH: Treatment of pharmacotherapy-refractory posttraumatic stress disorder among Cambodian refugees: a pilot study of combination treatment with cognitive-behavior therapy vs sertraline alone. Behav Res Ther 2003; 41:1271–1276
Hofmann SG, Sawyer AT, Korte KJ, Smits JA: Is it beneficial to add pharmacotherapy to cognitive-behavioral therapy when treating anxiety disorders? a meta-analytic review. Int J Cogn Ther 2009; 2:160–175
Spitzer RL, Williams JB, Gibbon M, First MB: Structured Clinical Interview for DSM-IV–Patient Version (SCID-P). Washington, DC, American Psychiatric Press, 1995
First M, Spitzer R, Gibbon M, Williams J, Benjamin L: Structured Clinical Interview for DSM-IV Axis II Disorders (SCID-II). Washington, DC, American Psychiatric Press, 1997
Guy W: ECDEU Assessment Manual for Psychopharmacology—Revised (DHEW publ no ADM 76-338). Rockville, Md, US Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, NIMH Psychopharmacology Research Branch, Division of Extramural Research Programs, 1976, pp 218–222
Endicott J, Nee J, Harrison W, Blumenthal R: Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol Bull 1993; 29:321–326
Hu MC, Pavlicova M, Nunes EV: Zero-inflated and hurdle models of count data with extra zeros: example from an HIV risk reduction intervention trial. Am J Drug Alcohol Abuse 2011 (in press)
Hedeker D: Generalized linear mixed models, in Encyclopedia of Statistics in Behavioral Science. Edited by, Everitt B, Howell D. New York, John Wiley & Sons, 2005
Hembree EA, Foa EB, Dorfan NM, Street GP, Kowalski J, Tu X: Do patients drop out prematurely from exposure therapy for PTSD? J Trauma Stress 2003; 16:555–562
Norris FH, Friedman MJ, Watson PJ: 60,000 disaster victims speak, part II: summary and implications of the disaster mental health research. Psychiatry 2002; 65:240–260
Feeny NC, Zoellner LA, Mavissakalian MR, Roy-Byrne PP: What would you choose? sertraline or prolonged exposure in community and PTSD treatment seeking women. Depress Anxiety 2009; 26:724–731
From the Trauma and Post Traumatic Stress Disorder Program, Anxiety Disorders Clinic, New York State Psychiatric Institute, New York; the Departments of Psychiatry and Biostatistics, Columbia University, New York; and the Department of Psychiatry, University of Pennsylvania, Philadelphia.
From the Trauma and Post Traumatic Stress Disorder Program, Anxiety Disorders Clinic, New York State Psychiatric Institute, New York; the Departments of Psychiatry and Biostatistics, Columbia University, New York; and the Department of Psychiatry, University of Pennsylvania, Philadelphia.
From the Trauma and Post Traumatic Stress Disorder Program, Anxiety Disorders Clinic, New York State Psychiatric Institute, New York; the Departments of Psychiatry and Biostatistics, Columbia University, New York; and the Department of Psychiatry, University of Pennsylvania, Philadelphia.
From the Trauma and Post Traumatic Stress Disorder Program, Anxiety Disorders Clinic, New York State Psychiatric Institute, New York; the Departments of Psychiatry and Biostatistics, Columbia University, New York; and the Department of Psychiatry, University of Pennsylvania, Philadelphia.
From the Trauma and Post Traumatic Stress Disorder Program, Anxiety Disorders Clinic, New York State Psychiatric Institute, New York; the Departments of Psychiatry and Biostatistics, Columbia University, New York; and the Department of Psychiatry, University of Pennsylvania, Philadelphia.
From the Trauma and Post Traumatic Stress Disorder Program, Anxiety Disorders Clinic, New York State Psychiatric Institute, New York; the Departments of Psychiatry and Biostatistics, Columbia University, New York; and the Department of Psychiatry, University of Pennsylvania, Philadelphia.
From the Trauma and Post Traumatic Stress Disorder Program, Anxiety Disorders Clinic, New York State Psychiatric Institute, New York; the Departments of Psychiatry and Biostatistics, Columbia University, New York; and the Department of Psychiatry, University of Pennsylvania, Philadelphia.
Dr. Schneier has received research funding from Forest Laboratories. Dr. Marshall is currently employed by Sunovion Pharmaceuticals. All other authors report no financial relationships with commercial interests.Supported by NIMH grant MH-068173 to Drs. Marshall and Schneier.
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.