DSM-5 Criteria for Substance Use Disorders: Recommendations and Rationale
Abstract
| Name | Degree(s) | Specialization | Country |
|---|---|---|---|
| Charles O’Brien (chair)b | M.D., Ph.D. | Addiction psychiatry | USA |
| Marc Auriacombe | M.D. | Addiction psychiatry | France |
| Guilherme Borges | Sc.D. | Epidemiology | Mexico |
| Kathleen Bucholz | Ph.D. | Epidemiology | USA |
| Alan Budney | Ph.D. | Substance use disorder treatment, marijuana | USA |
| Wilson Comptonb | M.D., M.P.E | Epidemiology, addiction psychiatry | USA |
| Thomas Crowleyc | M.D. | Psychiatry | USA |
| Bridget F. Grantb | Ph.D., Ph.D. | Epidemiology, biostatistics, survey research | USA |
| Deborah S. Hasin | Ph.D. | Epidemiology of substance use and psychiatric disorders | USA |
| Walter Ling | M.D. | Addiction psychiatry | USA |
| Nancy M. Petry | Ph.D. | Substance use and gambling treatment | USA |
| Marc Schuckit | M.D. | Genetics and comorbidity | USA |
Overarching Issues
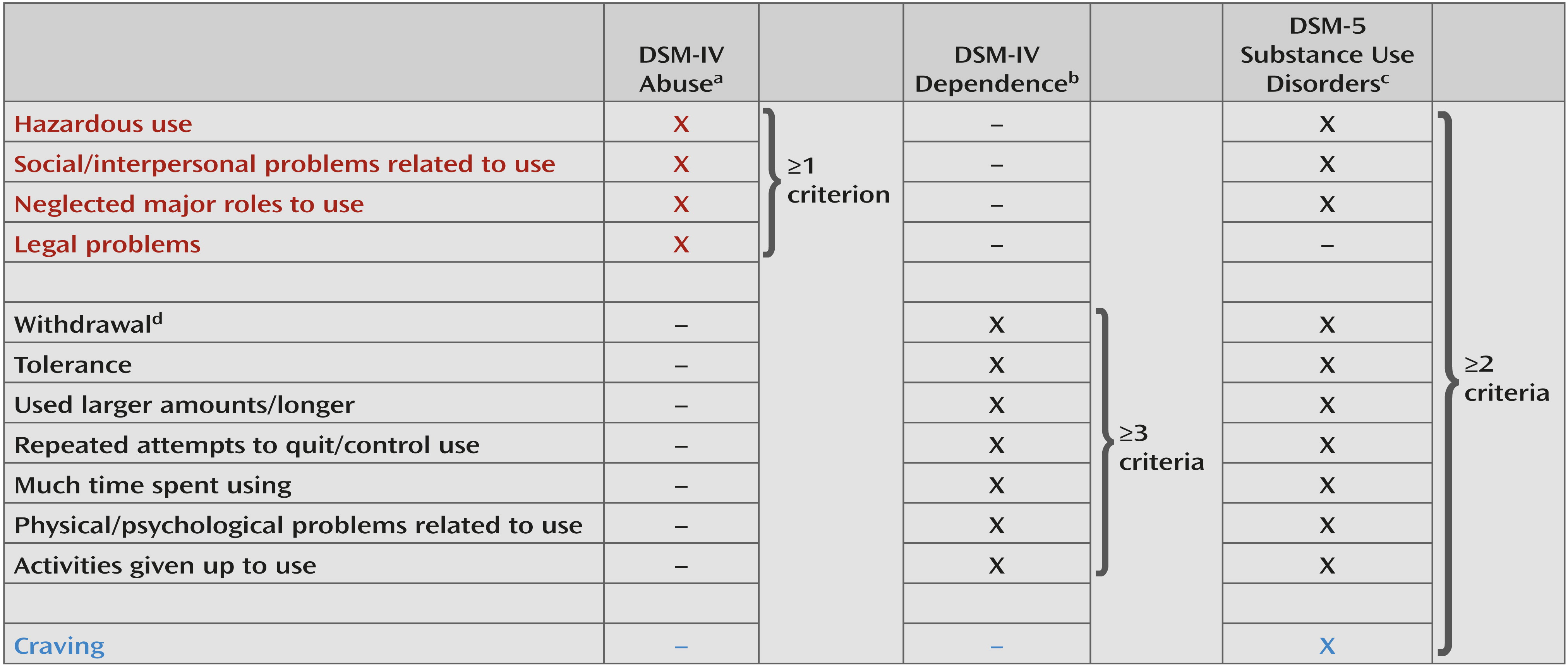
Should Abuse and Dependence Be Kept as Two Separate Diagnoses?
| Authors, Year (Source) | Substance | Country | Survey/Samplea | Sample Size | Diagnosis Instrumentb | Year of Data Collection | Time Frame | Unidimensionality Shown? |
|---|---|---|---|---|---|---|---|---|
| Adult, general population | ||||||||
| Saha et al., 2006 (35) | Alcohol | USA | NESARC | 20,846 | AUDADIS-IV | 2001–2002 | Current | Yes |
| Saha et al., 2007 (36) | Alcohol | USA | NESARC | 20,846 | AUDADIS-IV | 2001–2002 | Current | Yes |
| Gillespie et al., 2007 (31) | Cannabis | USA | Adult twins | 1,491 | SCID | 1990s | Lifetime | Yes |
| Lynskey and Agrawal, 2007 (37) | Amphetamine | USA | NESARC | 2,025 | AUDADIS-IV | 2001–2002 | Lifetime | Yes |
| Cannabis | USA | NESARC | 8,933 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Cocaine | USA | NESARC | 2,672 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Hallucinogens | USA | NESARC | 2,525 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Inhalants | USA | NESARC | 728 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Opioids | USA | NESARC | 2,060 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Sedatives | USA | NESARC | 1,896 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Tranquilizers | USA | NESARC | 1,487 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Compton et al., 2009 (38) | Cannabis | USA | NESARC | 1,603 | AUDADIS-IV | 2001–2002 | Current | Yes |
| McBride et al., 2010 (39) | Nicotine | USA | NESARC | 6,185 | AUDADIS-IV | 2001–2002 2004–2005 | Current and lifetime | Yes (dependence only) |
| Saha et al., 2010 (40) | Nicotine | USA | NESARC | 7,852 | AUDADIS-IV | 2001–2002 2004–2005 | Current | Yes (dependence only) |
| Shmulewitz et al., 2010 (41) | Alcohol | Israel | Household | 1,160 | AUDADIS-IV | 2007–2009 | Current and lifetime | Yes |
| Keyes et al., 2011 (42) | Alcohol | USA | NLAES | 18,352 | AUDADIS-IV | 1991–1992 | Current | Yes |
| Kerridge et al., 2011 (43) | Hallucinogens | USA | NESARC | 2,176 | AUDADIS-IV | 2001–2002 | Lifetime | Yes |
| Inhalants | USA | NESARC | 664 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Saha et al., 2012 (44) | Amphetamine | USA | NESARC | 1,750 | AUDADIS-IV | 2001–2002 | Lifetime | Yes |
| Cocaine | USA | NESARC | 2,528 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Opioids | USA | NESARC | 1,815 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Sedatives | USA | NESARC | 1,609 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Tranquilizers | USA | NESARC | 1,301 | AUDADIS-IV | 2001–2002 | Lifetime | Yes | |
| Shmulewitz et al., 2011 (45) | Nicotine | Israel | Household | 727 | AUDADIS-IV | 2007–2009 | Lifetime | Yes |
| Wu et al., 2011 (46) | Opioids | USA | NSDUH | 2,824 | Survey-specific instrument | 2007 | Current | Yes |
| Mewton et al., 2011 (47) | Alcohol | Australia | NSMHWB | 7,746 | CIDI version 2.0 (modified) | 1997 | Current | Yes |
| Gilder et al., 2011 (48) | Alcohol | USA | American Indians | 530 | SSAGA | 1990s | Lifetime | Yes |
| Casey et al., 2012 (49) | Alcohol | USA | NESARC | 22,177 | AUDADIS-IV | 2004–2005 | Current | Yes |
| Wu et al., 2012 (50) | Cannabis | USA | NSDUH | 6,917 | Survey-specific instrument | 2008 | Current | Yes |
| Adult, clinical or mixed | ||||||||
| Langenbucher et al., 2004 (51) | Alcohol | USA | Clinical | 372 | CIDI–SAM | 1990s | Lifetime | Yes |
| Cannabis | USA | Clinical | 262 | CIDI–SAM | 1990s | Lifetime | Yes | |
| Cocaine | USA | Clinical | 225 | CIDI–SAM | 1990s | Lifetime | Yes | |
| Wu et al., 2009 (52) | Cocaine | USA | Clinical | 366 | DSM-IV checklist | 2001–2003 | Current | Yes (dependence only) |
| Opioids | USA | Clinical | 354 | DSM-IV checklist | 2001–2003 | Current | Yes (dependence only) | |
| Wu et al., 2009 (53) | Alcohol | USA | Clinical | 462 | DSM-IV checklist | 2001–2003 | Current | Yes (dependence only) |
| Cannabis | USA | Clinical | 311 | DSM-IV checklist | 2001–2003 | Current | Yes (dependence only) | |
| Borges et al., 2010 (54) | Alcohol | Multinational | ED | 3,191 | Adapted CIDI | 1995–2003 | Current | Yes |
| Alcohol | Argentina | ED | 662 | Adapted CIDI | 2001 | Current | Yes | |
| Alcohol | Mexico | ED | 547 | Adapted CIDI | 1996–1997 | Current | Yes | |
| Alcohol | Poland | ED | 1,098 | Adapted CIDI | 2002–2003 | Current | Yes | |
| Alcohol | USA | ED | 884 | Adapted CIDI | 1995–1996 | Current | Yes | |
| Borges et al., 2011 (55) | Alcohol | Argentina, Mexico, Poland, USA | ED | 3,191 | CIDI | 1995–2003 | Current | Yes |
| McCutcheon et al., 2011 (56) | Alcohol | USA | COGA | 8,605 | SSAGA | 1989–1996 | Lifetime | Yes |
| Hasin et al., 2012 (57) | Alcohol | USA | Clinical | 543 | PRISM | 1994–1999 | Current | Yes |
| Cannabis | USA | Clinical | 340 | PRISM | 1994–1999 | Current | Yes | |
| Cocaine | USA | Clinical | 483 | PRISM | 1994–1999 | Current | Yes | |
| Opioids | USA | Clinical | 364 | PRISM | 1994–1999 | Current | Yes | |
| Adolescent, general population | ||||||||
| Harford et al., 2009 (58) | Alcohol | USA | NSDUH | 133,231 | Survey-specific instrument | 2002–2005 | Current | Yes |
| Strong et al., 2009 (59) | Nicotine | USA | 6th–10th graders | 296 | DSM-IV nicotine dependence measure; mFTQ; NDSS | 2003 | Current | Yes (dependence only) |
| Wu et al., 2009 (60) | Opioids | USA | NSDUH | 1,290 | Survey-specific instrument | 2006 | Current | Yes |
| Beseler et al., 2010 (61) | Alcohol | USA | College students | 353 | 11-item self-report measure (based on DSM criteria) | 2007 | Current | Yes |
| Rose and Dierker, 2010 (62) | Nicotine | USA | NSDUH | 2,758 | Survey-specific instrument | 1995–1998 | Current | Yes (dependence only) |
| Wu et al., 2010 (63) | Hallucinogens | USA | NSDUH | 1,548 | Survey-specific instrument | 2004–2006 | Current | Yes |
| Hagman and Cohn, 2011 (64) | Alcohol | USA | College students | 396 | Survey-specific instrument | 2010 | Current | Yes |
| Mewton et al., 2011 (65) | Alcohol | Australia | NSMHWB | 853 | CIDI version 2.0 (modified) | 1997 | Current | Yes (“little evidence for DSM-IV abuse/ dependence distinction in young adulthood”) |
| Piontek et al., 2011 (66) | Cannabis | France | SHCDDP | 3,641 | M-CIDI | 2008 | Current | Yes |
| Strong et al., 2012 (67) | Nicotine | USA | 6th–10th graders and relatives | 556 | DSM-IV nicotine dependence measure; mFTQ; NDSS | 2003 | Current | Yes (dependence only) |
| Adolescent, clinical or mixed | ||||||||
| Martin et al., 2006 (28) | Alcohol | USA | Clinical | 464 | SCID | 2002 | Lifetime | Yes |
| Cannabis | USA | Clinical | 417 | SCID | 2002 | Lifetime | Yes | |
| Gelhorn et al., 2008 (68) | Alcohol | USA | Mixed | 5,587 | CIDI-SAM | 1993–2007 | Lifetime | Yes |
| Hartman et al., 2008 (69) | Cannabis | USA | Mixed | 5,587 | CIDI-SAM | 1993–2007 | Lifetime | Yes |
| Perron et al., 2010 (70) | Inhalants | USA | Clinical | 279 | DIS-IV | 2004 | Lifetime | Yes |
| Chung et al., 2012 (71) | Nicotine | USA | Clinical | 471 | SCID | 1990–2009 | Lifetime | Yes |
Should Any Diagnostic Criteria Be Dropped?
Legal problems.
Tolerance.
Should Any Criteria Be Added?
Craving.
Consumption.
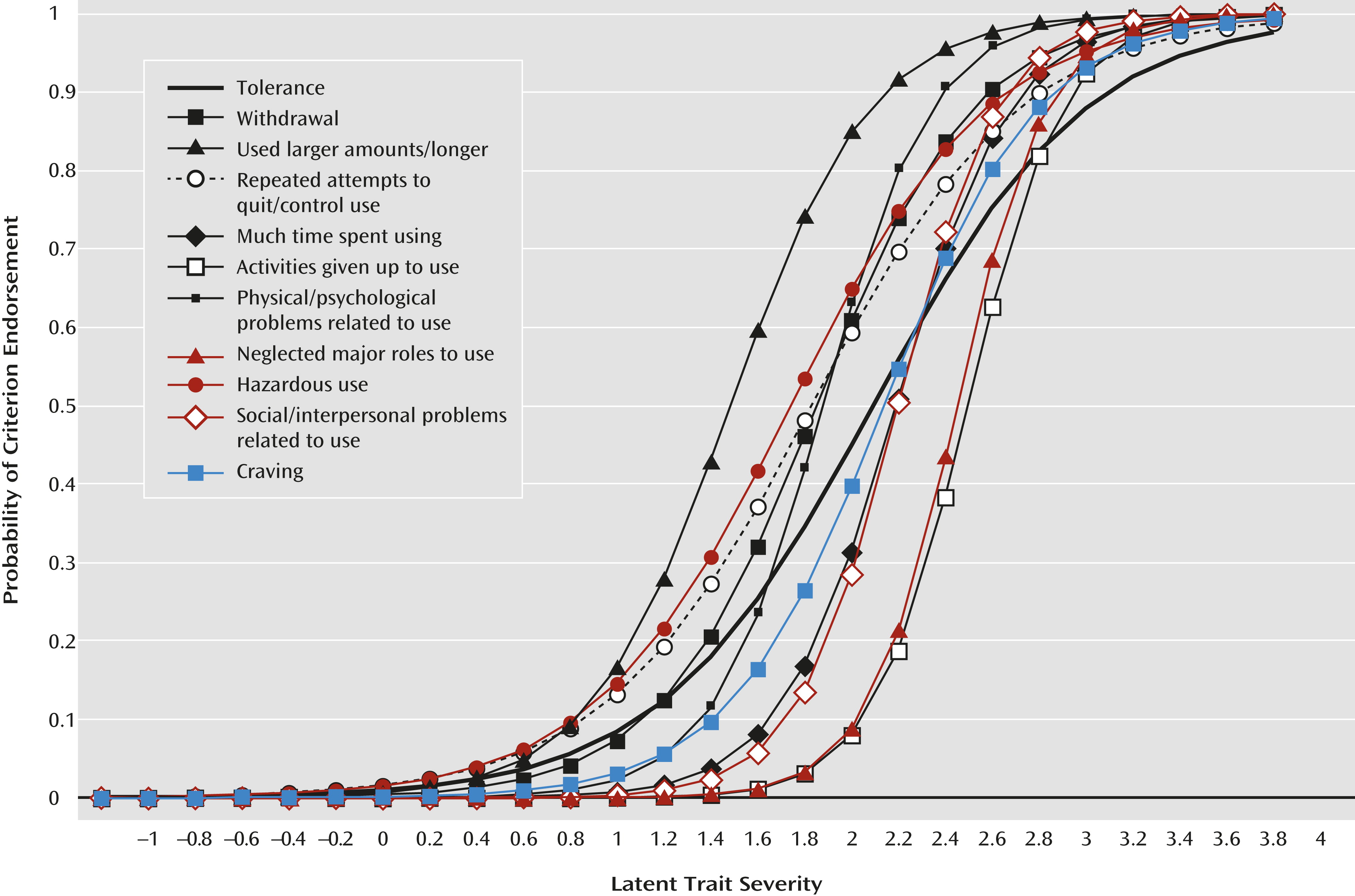
What Should the Diagnostic Threshold Be?
| Sample (source) | Sample Size | Prevalence | Kappa |
|---|---|---|---|
| National Epidemiologic Survey on Alcohol and Related Conditions (6) | |||
| Drinkers, last 12 monthsa | 20,836 | ||
| DSM-IV alcohol | 0.10 | ||
| DSM-5, ≥2 criteria | 0.11 | 0.73 | |
| DSM-5, ≥3 criteria | 0.06 | 0.73 | |
| Collaborative studies on genetics of alcoholism nonproband adults (56) | |||
| Drinkers, lifetime | 6,673 | ||
| DSM-IV alcohol | 0.43 | ||
| DSM-5, ≥2 criteria | 0.43 | 0.80 | |
| DSM-5, ≥3 criteria | 0.32 | 0.74 | |
| Cannabis users, lifetime | 4,569 | ||
| DSM-IV cannabis | 0.35 | ||
| DSM-5, ≥2 criteria | 0.33 | 0.82 | |
| DSM-5, ≥3 criteria | 0.26 | 0.75 | |
| Cross-national emergency departments (54) | |||
| Drinkers, last 12 monthsa | 3,191 | ||
| DSM-IV alcohol | 0.21 | ||
| DSM-5, ≥2 criteria | 0.21 | 0.80 | |
| DSM-5, ≥3 criteria | 0.15 | 0.79 | |
| Metropolitan clinical sample (N=663) (57) | |||
| Drinkers, last 12 monthsa | 534 | ||
| DSM-IV current alcohol | 46.9 | ||
| DSM-5, ≥2 criteria | 48.7 | 0.94 | |
| DSM-5, ≥3 criteria | 45.7 | 0.96 | |
| DSM-5, ≥4 criteria | 42.8 | 0.92 | |
| Cannabis users, last 12 monthsa | 340 | ||
| DSM-IV cannabis | 21.1 | ||
| DSM-5, ≥ 2 criteria | 19.6 | 0.85 | |
| DSM-5, ≥ 3 criteria | 16.4 | 0.83 | |
| DSM-5, ≥ 4 criteria | 13.4 | 0.73 | |
| Cocaine users, last 12 monthsa | 483 | ||
| DSM-IV cocaine | 52.9 | ||
| DSM-5, ≥2 criteria | 54.5 | 0.93 | |
| DSM-5, ≥3 criteria | 51.7 | 0.96 | |
| DSM-5, ≥4 criteria | 48.9 | 0.93 | |
| Heroin users, last 12 monthsa | 364 | ||
| DSM-IV heroin | 40.0 | ||
| DSM-5, ≥2 criteria | 41.6 | 0.95 | |
| DSM-5, ≥3 criteria | 39.2 | 0.97 | |
| DSM-5, ≥4 criteria | 36.5 | 0.96 |
How Should Severity Be Represented?
Specifiers
Physiological cases.
Course.
Could the Definitions of Substance-Induced Mental Disorders Be Improved?
Could Biomarkers Be Utilized in Making Substance Use Disorder Diagnoses?
Should Polysubstance Dependence Be Retained?
Substance-Specific Issues
Should Cannabis, Caffeine, Inhalant, and Ecstasy Withdrawal Disorders Be Added?
Cannabis.
Inhalants/hallucinogens.
Caffeine.
Could the Nicotine Criteria Be Aligned With the Diagnostic Criteria for the Other Substance Use Disorders?
Should Neurobehavioral Disorder Associated With Prenatal Alcohol Exposure Be Added?
Issues Not Related To Substances
Should Gambling Disorder and Other Putative Behavioral “Addictions” Be Added to the Substance Disorders Chapter?
Gambling.
Other non-substance-related disorders.
Should the Name of the Chapter Be Changed?
Present Status and Future Directions
Footnotes
Supplementary Material
- View/Download
- 32.78 KB
References
Information & Authors
Information
Published In


History
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).