T
o the E
ditor: Converging preclinical data suggest that stimulating a warm-sensitive thermoafferent spinoparabrachial pathway that projects from the skin (and other epithelial linings) to specific midbrain serotonergic nuclei produces antidepressant-like effects in animal models, while simultaneously inducing thermoregulatory cooling (
1). Interestingly, several lines of evidence indicate that major depressive disorder may be characterized by suboptimal activity in this pathway, based on repeated observations that the disorder is associated with increased core body temperature, reduced thermoregulatory cooling (e.g., sweating), and alterations in peripheral measures of serotonin (5-HT) activity, all of which are expected manifestations of impaired activity in the skin-to-brain-to-skin thermoregulatory circuit within which the ascending spinoparabrachial pathway and its CNS projections form core components (
1).
We used ongoing clinical activities at a private alternative treatment hospital in Switzerland to evaluate the relevance of these observations for the treatment of depression by examining the acute antidepressant effects of mild whole-body hyperthermia in 16 medically healthy adults who were clinically diagnosed with major depressive disorder. Our interest in whole-body hyperthermia was based on animal data from our group demonstrating that exposure to warm temperature activates the spinoparabrachial pathway and the midbrain 5-HT nuclei to which it projects (
1).
Mild-intensity whole-body hyperthermia was induced using a Heckel 2000 device, which uses water-cooled infrared lamps to heat the body (Heckel Medizintechnik GmbH, Esslingen, Germany). Using the Centers for Epidemiologic Studies Depression Scale (CES-D) (
2), we found that a single session (mean session time, 126.7 minutes [SD=18.0]) induced a rapid, robust, and sustained reduction in depressive symptoms (CES-D score before treatment, mean=29.9 [SD=10.6]; 5 days after treatment, mean=19.2 [SD=12.3]; t=4.53, df=15, p<0.001, effect size=1.13). Thirteen of these patients received no other pharmacologic or psychotherapeutic intervention during the 5 days following whole-body hyperthermia, whereas three patients were being chronically treated with a selective serotonin reuptake inhibitor (SSRI), with no change in dosage during the study period. Interestingly, when examined separately, whole-body hyperthermia appeared to have no effect in the three individuals receiving SSRI treatment. With these three individuals removed from analysis, the effect size of the hyperthermia increased (t=5.15, df=12, p<0.001, effect size=1.4).
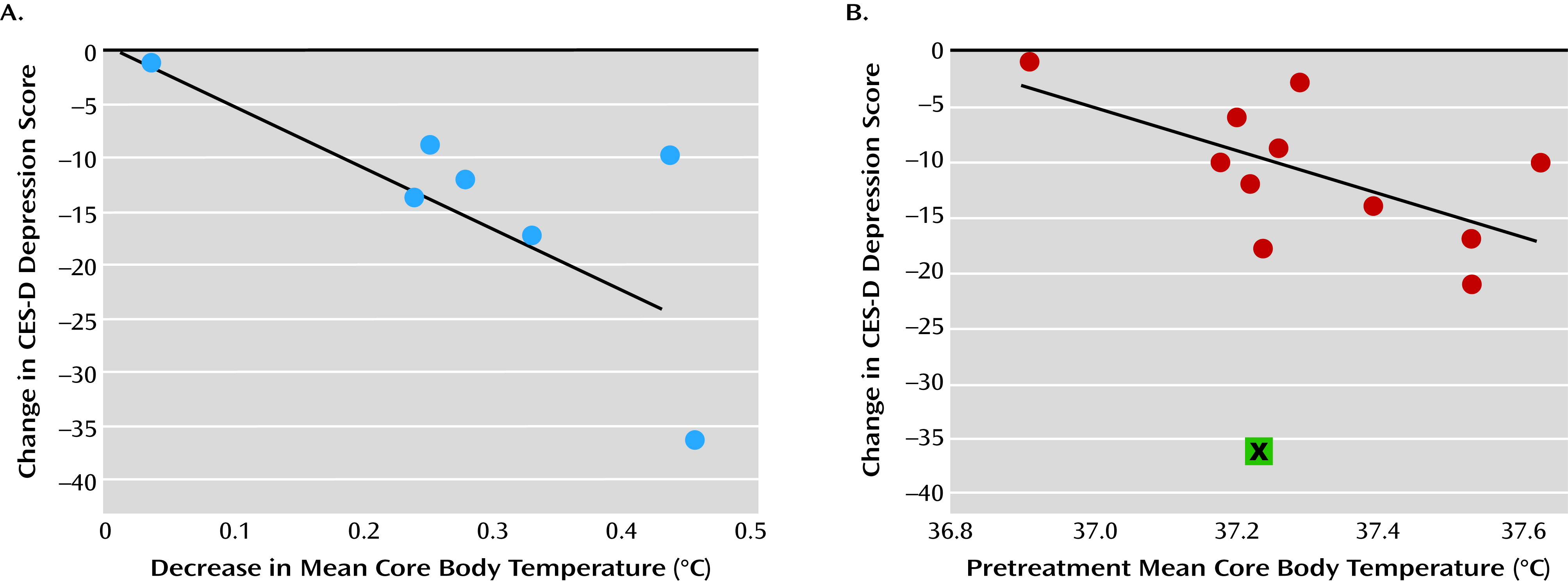
Mean core body temperature data were obtained in 12 patients before whole-body hyperthermia and in seven patients both before and 5 days after the intervention. Core temperature was assessed with either an indwelling temperature sensor (EndoTherm GmbH) inserted rectally in male patients or vaginally in female patients or by hourly measurement of rectal temperature while awake. The same method was used for both assessments in patients who had their core body temperature measured twice (i.e., before and 5 days after whole-body hyperthermia). The treatment induced significant and persistent thermoregulatory cooling, as reflected by a drop in mean core body temperature from 37.3°C (SD=0.24) before treatment to 37.0°C (SD=0.14) 5 days after treatment (t=5.5, df=6, p=0.002, effect size=2.1). Moreover, a trend-level large effect size correlation was observed between reductions in CES-D scores and reductions in mean core body temperatures in the same period (r=0.73, df=4, p=0.06) (
Figure 1A). Finally, higher mean core body temperature prior to hyperthermia strongly correlated with degree of antidepressant response 5 days after treatment (r=0.62, df=9, p=0.043), with one statistical outlier removed (
Figure 1B).
Taken together, these findings suggest that whole-body hyperthermia provides rapid and sustained relief of depressive symptoms and may do so by sensitizing physiological pathways important for thermoregulatory cooling that also affect brain regions implicated in the regulation of mood. Although this is the first study, to our knowledge, to examine this intervention specifically for major depressive disorder, our findings are consistent with reports that hyperthermia improves mood and quality of life when used in medically ill patients (
3,
4).