In the mid-1950s, the serendipitous convergence of two career paths resulted in a profound boost to what Lipowski (
1) termed the important “organizational development phase” of consultation-liaison psychiatry.
Herrman Blumgart was born in 1895 and attended Harvard College. With a special interest in psychology and social ethics, he entered Harvard Medical School, where he attached himself to Francis Peabody (
2), author of the oft-quoted classic paper on the “care of the patient.” He collaborated with Peabody on research and publications, and he claimed Peabody as his mentor and physician-model. Later, as Director of Medical Research and Assistant Professor of Medicine at Beth Israel Hospital in Boston, he inaugurated with Walter Cannon elective clinics for medical students that integrated principles of physiology, biochemistry, and pharmacology with problems of patient care. After a leave of absence to serve as consultant in the 2nd U.S. Army Service Command in the India-Burma-China theater, he returned from active duty in 1946 to be Physician-in-Chief at Beth Israel Hospital and Professor of Medicine at Harvard Medical School.
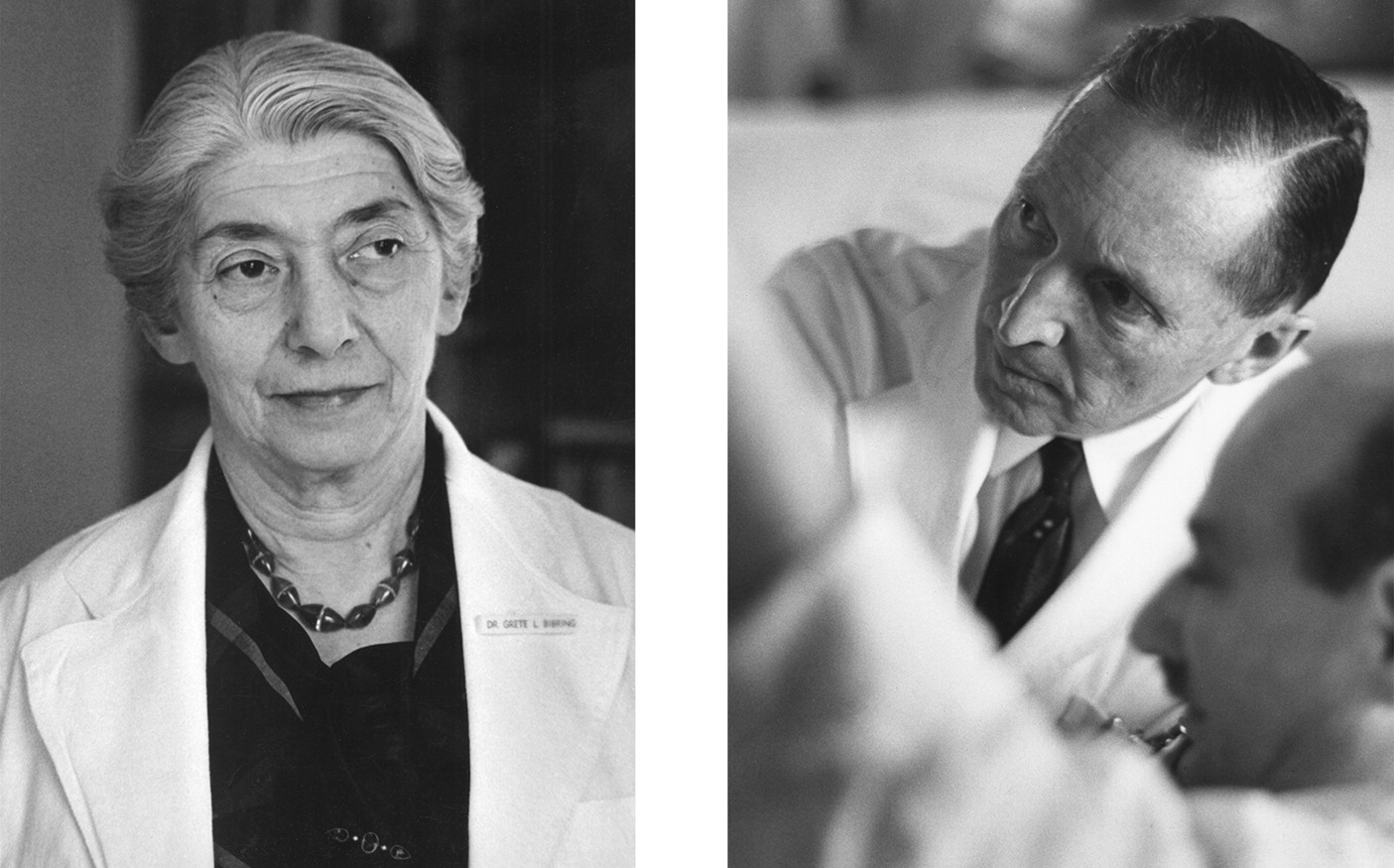
Herrman was intent on developing a strong Department of Psychiatry at Beth Israel Hospital. He was impressed with the value of psychiatry in treating “psychogenic” disorders at the battlefield, had an abiding interest in psychology and psychiatry, and may have been influenced by his psychoanalyst brother Leonard, who was President of the New York Psychoanalytic Society during the same years that Herrman was in the military and, like Herrman, was a member of the American Psychosomatic Society in 1953. Unfamiliar with psychoanalyst Dr. Grete Bibring, he nonetheless invited her to accept the position as head of the psychiatry department.
Grete Lehner (Bibring) was born in 1899 into the rich cultural ambience of fin de siècle Vienna. At Vienna University she joined with three other medical students (Otto Fenichel, Wilhelm Reich, and Edward Bibring) to approach Freud in quest of answers to psychological questions. She attended and then graduated from the Vienna Psychoanalytic Institute, but then with the Nazi Anschluss in 1938, they all fled with Freud’s family to England, where Grete gained recognition in psychoanalytic circles as an outstanding teacher and clinician. She accepted an invitation to Boston and immigrated there with her family in 1941, rapidly immersing herself in its rich psychoanalytic community, teaching, supervising psychoanalytic candidates, and treating patients.
In the country only 5 years when Blumgart asked her to head the new psychiatry department, she considered herself “so thoroughly involved in psychoanalysis” that she was not properly qualified for such a position in a medical setting (
3). She declined the position and evoked from Blumgart a gentle chastisement, the remark that psychoanalysts were always ready to offer explanations but reluctant to make a major commitment. In a Festschrift for Blumgart (
4) in 1962, Bibring said, “This was a serious point… [that] really influenced me to a large extent to accept this most disconcerting job.”
In 1946 she became the first woman to head a clinical department at Harvard Medical School, and in 1955 she was designated Psychiatrist-in-Chief. In 1961 she became the first woman appointed to a full professorship at Harvard Medical School.
Psychiatry at Beth Israel Hospital flourished under Bibring's directorship and Blumgart’s support. Daily “medical” rounds were shared by medicine and psychiatry. A very strong emphasis on the personal role of the physician in caring for patients was propagated through an active Medical Psychology Consultation Service (later renamed Consultation-Liaison Service). Again, in the Festschrift (
4), Bibring remarked on how little Blumgart had known her but how gradually Blumgart's “system of values” influenced her and the department psychiatrists. “This is how our team began...in these first and difficult years…. Herrman Blumgart with his leadership stood behind us; he had confidence and understanding and supported the Psychiatry Department constantly and unobtrusively.
Such support is of decisive and critical significance for our kind of assignment” (italics added).
With shared values—Blumgart’s “caring for patients” (
5) and Bibring’s “medicopsychotherapeutic approach” (
6)—these two pioneers brought insight and wisdom to physicians “at the interface.” Their collaboration lends credence to the belief that the fate of psychiatry in the general medical hospital depends greatly on the appreciation and support of the chief of medicine.