Child maltreatment represents a highly deleterious influence on the mental health and development of children (
1–
5). It is preventable (
6,
7) and yet alarmingly prevalent (
8), affecting 1 in 8 U.S. children. While maltreatment at any age can lead to adverse outcomes, maltreatment in early childhood is associated with particular insults to cognitive and social emotional development, as well as serious physical risk (
9,
10), resulting in enduring abnormalities of emotion regulation, social relatedness, and executive functioning (
11,
12).
Studies in the United States have found that the likelihood that a child placed in foster care for child abuse or neglect will experience maltreatment recidivism after reunification with his or her birth parents is between 30% and 37% (
13,
14). Thus, the sentinel event of placement of a young child in protective custody for child maltreatment represents a critical opportunity for preventive intervention. In a large administrative-data study of chronic, official-report child abuse or neglect, Jonson-Reid and colleagues (
15) showed that children who experienced a single episode of official-report maltreatment—but no further occurrences—incurred rates of mental health care utilization that were not significantly elevated compared with those of children in the general population. The study revealed a dose-response relationship between number of official reports of child maltreatment (over two) and adverse psychiatric outcomes.
Interventions to stabilize and enhance the outcomes of children in foster care include those that focus on 1) the quality of the foster care environment, 2) decision making about reunification, and/or 3) support of the birth parents (in the event of reunification). Regarding quality of the foster care environments, Kessler et al. (
16) demonstrated significant reductions in adult psychopathology among foster care alumni (primarily school-aged) who had been enrolled in a model case management program in which case managers had higher levels of training and lower caseloads than was the case for care as usual. The outcomes of other efforts to enhance the foster caregiving environment—for example, via multidimensional treatment foster care, a wraparound multimodal intervention for foster families of children and adolescents with challenging behavior—have been promising but mixed (
17,
18).
Over a decade ago, Zeanah and colleagues (
10) reported on the naturalistic results of a Family Court collaboration with an academic division of child psychiatry (at Tulane University in New Orleans), focused primarily on the other two domains of intervention: decision making and support of birth families in the reunification process. The program responded to a long-recognized need to assist courts and social services systems with the appraisal of the unique mental health needs of children in this age range. The Tulane model was organized around the integration of skilled child psychiatric assessment, dyadic intervention to promote parent-child attachment, and parental psychiatric care (whenever necessary or appropriate). It reduced, by over half, the occurrence of maltreatment recidivism in comparison with a matched group of children who did not receive the intervention. This reduction appeared attributable both to an overall reduction in the rate of reunification and to the enhanced mental health support that was provided to families by the clinical team during the reunification process and that was ensured by court provisions after reunification occurred.
To our knowledge, these important findings have never been replicated, or even attempted, among young children in foster care, although similar comprehensive intervention strategies have been implemented with considerable success for young children at risk (i.e., before a documented instance of child abuse or neglect has occurred). In 2011, our group secured continuous local government funding for a quasi-replication of the Tulane model in St. Louis County, Missouri, entitled the SYNCHRONY Project. Here we describe this court-based intervention as a psychiatric prototype of a two-generation intervention, which has been strongly advocated in early childhood policy recommendations (
19,
20) but for which there is a pressing need for more scientific data. We report our experience with children initially enrolled in the first 30 months of program implementation (January 2011–June 2013) and summarize the progress of the children (through March 2015) in the context of aggregate government data available for the most recent historic cohort of 300 children in the same age range who were placed in protective custody before the SYNCHRONY Project was launched, and whose cases had been closed by the St. Louis County Family Court at the time of this program analysis. We hypothesized that, in comparison to the historic cohort, children enrolled in the SYNCHRONY Project would be selected for higher-than-average risk but would demonstrate a comparable or lower maltreatment recidivism rate and shorter total time in foster care. Furthermore, among SYNCHRONY enrollees, we hypothesized that serial standardized measurements of the quality of parent-child relationships and the adaptive functioning of the children would steadily improve over the course of the intervention.
Program Evaluation
Analyses for this initial program evaluation included comparisons of key sample characteristics between the SYNCHRONY Project cohort and the historic cohort. Within the SYNCHRONY cohort, we examined time-rated change in systematically acquired outcome measures (see below). This program evaluation was reviewed by the Human Research Protection Office of the Washington University School of Medicine and fell into the category of “non-research” in that it was restricted to use of existing, de-identified, clinically acquired program data and public records.
Sample
The SYNCHRONY Project (Strengthening Young Children by Optimizing Family Support in Infancy) was launched in 2011 through funding from a locally implemented children’s services sales tax (the St. Louis County Children’s Service Fund;
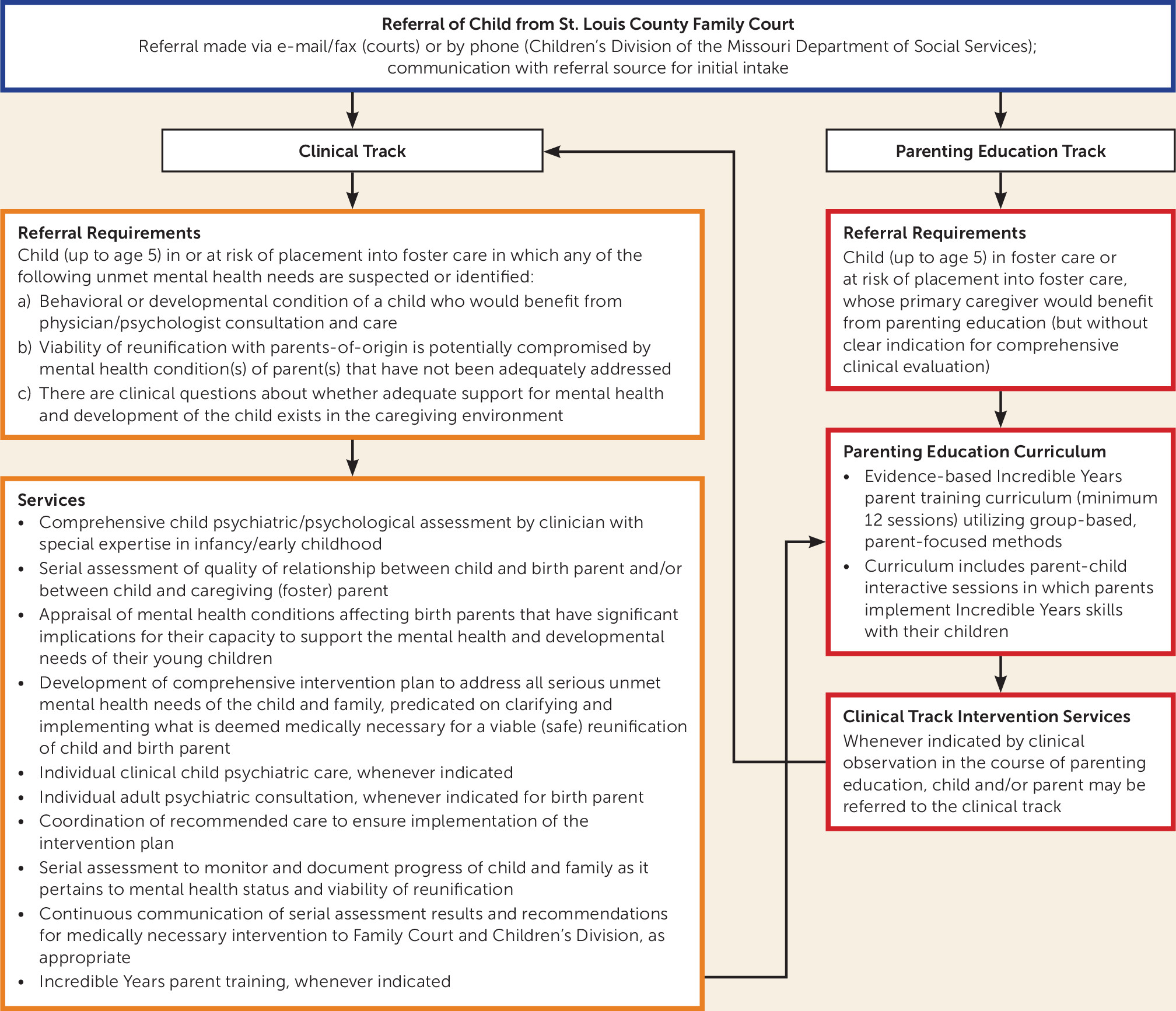
http://keepingkidsfirst.org). Families of young children (from birth through age 5) who were placed in foster care under the jurisdiction of the Family Court of St. Louis County for child abuse or neglect were referred by the court for voluntary participation in the program in one of two referral tracks—a comprehensive clinical track or a parenting education track (
Figure 1). The decision to refer and the choice of referral track were made by deputy juvenile officers of the court assigned to the children’s cases. Eighty-one percent of referred families ultimately enrolled in the program. In the clinical track, the goal was to specify and resolve suspected unmet mental health needs of children or their birth parents through the provision of comprehensive mental health service. This included two-generation assessment and intervention planning, judicious referral for clinical services indicated by the assessment, direct clinical care whenever clinically indicated services were not available in the community, and evidence-based parenting education (implementing the Incredible Years model). The parenting education track was an education-only track, although families in that track were transferred to the clinical track if mental health needs arose or became evident during the course of parenting education (this was common). This is a report on 119 young children in 106 families (first enrolled from January 2011 to June 2013) whose flow through the program is summarized in
Figure 1.
A historic cohort was assembled from summary statistics on infants and toddlers whose county child abuse/neglect cases were closed before the 2011 launch of the SYNCHRONY project. This information, which may be used for governmental reporting and monitoring of service delivery, was available in aggregate only (no individual-level data) from the court. An initial review of this most recent set of 300 cases revealed that 53 of the historic cohort children had been placed in foster care exclusively for in utero drug exposure. Such infants were never referred to SYNCHRONY unless there was an alternative primary reason for placement in protective custody. Therefore, infants with in utero drug exposure were removed from the historic cohort, leaving aggregate data on 247 children to serve as a contrast group.
Table 1 summarizes selected characteristics of the SYNCHRONY and historic cohorts.
Two-Generation Psychiatric Assessment
The program’s two-generation assessment systematically included 1) evaluation of the child; 2) ascertainment of characteristics of the parent-child relationship (historic and observed) that were relevant to the viability of reunification; 3) clinical screening for mental health conditions of the birth parent(s) that would have implications for the safety and viability of reunification; and 4) the development of a comprehensive plan for a supplemental behavioral health/developmental intervention for the family.
Comprehensive Intervention Planning
The development of a comprehensive set of recommendations for “value-added” clinically indicated intervention—i.e., supplemental intervention that the family was not already receiving at the time of referral—was a primary endpoint of the two-generation assessment. For any given family, these recommendations generally fell into one or more of the following general categories: parent-child psychotherapy/family therapy; specific revision of the visitation schedule; child individual therapy (psychotherapy or developmental therapy); child psychopharmacologic treatment; and adult psychiatric treatment.
In all cases, recommendations were communicated to the court and the Missouri Department of Social Services, and whenever medically indicated services of appropriate quality were not accessible to the family, they were provided by SYNCHRONY. Each family was subsequently seen at least quarterly for assessment of clinical progress, titration of necessary mental health services, and documentation of medical judgment regarding the safety of reunification at each juncture. In most cases, the results of serial assessment comprised a critical evidentiary basis for the court’s decision making regarding the appropriateness and viability of reunification.
Parenting Education
The SYNCHRONY Project Parenting Education program utilized the Incredible Years curriculum for toddlers (
21), a 14-session group-based curriculum keyed to video vignettes that are viewed, discussed, and role played by parents. The topics include positive parenting behaviors that reward and promote attachment, communication, self-regulation, and cooperation; these include listening, following a child’s leads, giving praise, and providing descriptive comments. In addition, techniques for preventing and managing maladaptive behaviors in children are taught and rehearsed, including clarification of expectations, ignoring, and time-out. “Hands-on practice” sessions with the parents’ own children (whenever possible) supplemented the curriculum after every third session; these sessions involved semistructured play activities that could be reimplemented at home, such as sensory play for infants, symbolic interactive (puppet) play for toddlers, creative expression (finger painting), and the building of “blanket forts” to simulate safety, intimacy, and composure. Clinicians trained in the Incredible Years curriculum were available to guide and support parents through these activities. Of the first 106 SYNCHRONY families, 55 participated in the parenting education curriculum, and 39 “graduated” by attending 75% or more of the sessions.
Serial Measurement
The Children’s Global Assessment Scale is a widely implemented clinical rating scale used to document children’s overall adaptive functioning; the normal score range is 70–100 on a scale from 1 to 100. The instrument features descriptive scoring anchors and very favorable psychometric properties (
22). The Children’s Global Assessment Scale was completed serially by doctoral-level clinicians for all clinical track children age 4 and older. The test-retest correlation was 0.57 programwide, supporting substantial reliability of the measurements.
The Caregiver-Child Social-Emotional Relationship Rating Scale is a brief scale used to measure the quality of interactions between children and their birth parents. Emotional availability of caregivers, mutuality of caregiver-child interactions, child and caregiver affect, and the extent to which the caregiver follows the child’s lead are scored according to highly descriptive scoring anchors that have been validated in previous research (
23). Ratings were completed serially by licensed clinicians. The intraclass correlation for ratings for families serially observed in the parenting education curriculum was 0.52, supporting substantial test-retest reliability of the measurements.
The Incredible Years Parenting Scale is a 30-item self-report scale of parental discipline originally developed to assess the disciplinary practices of parents of preschool children (
24). Parents indicate their tendencies to use specific discipline strategies using a 7-point Likert scale, where 1 indicates a high probability of using an effective alternative discipline strategy and 7 indicates a high probability of making a disciplinary error. Factor analyses have revealed independent contributions of three components: overreactivity (authoritarian parenting style, which includes threats and physical punishment), laxness (characterizes a caregiver who is permissive and inconsistent when providing discipline), and verbosity (describes a caregiver who tends to give lengthy verbal reprimands, rather than taking direct action).
Results
Characteristics and Outcomes of the SYNCHRONY and Historic Cohorts
Children enrolled in the SYNCHRONY Project were highly representative of historic St. Louis County populations of young children taken into court custody; the children were predominantly from minority groups and neglected, with a slight preponderance of males over females. SYNCHRONY families (closed cases) were over three times more likely than the average family in the historic cohort to have had a prior history of adjudication in the Family Court, indicative of the unusually high level of risk that characterized the initial group of families referred to the program (see
Table 1; 54% of SYNCHRONY families manifested at least two of the major risk factors presented in the table).
The threefold higher rate of prior adjudication among SYNCHRONY families established an expectation of an elevated rate of subsequent referral to the Children’s Division of the Missouri Department of Social Services for child abuse or neglect while in custody. Contrary to this expectation, there was no significant difference in rate of subsequent referral for child maltreatment between SYNCHRONY and historic cohort families, consistent with a protective effect of enrollment in the SYNCHRONY project. The rate of successful reunification in this high-acuity cohort (30%) was significantly lower than that for the historic cohort (53%, p<0.001) (
Table 2). We note that the intended impact of the program involved both the support of successful reunifications and the prevention of unsafe reunifications. On average, children in SYNCHRONY experienced a shorter period between initial placement in protective custody and case closure.
Although it is difficult to ascertain the extent to which SYNCHRONY medical recommendations independently influenced court dispositions, we note the following: 1) The vast majority of SYNCHRONY medical recommendations for therapeutic support and modification of visitation parameters were supported by the Court. 2) The prevailing disposition (reunification versus guardianship or termination of parental rights) was reversed after referral to SYNCHRONY in approximately one-fifth of the cases. 3) Since the inaugural year of the project, the St. Louis County Family Court has continuously referred a majority of its preschool protective custody cases to SYNCHRONY (excluding those for in utero drug exposure).
Clinical Mental Health Needs Identified and Addressed by the SYNCHRONY Project
For all 106 enrolled SYNCHRONY cases, unmet mental health needs of the children (untreated or inadequately addressed clinical developmental or behavioral problems), the parents (active untreated or inadequately treated psychiatric diagnoses), or the parent-child relationship (inadequate access to high-quality parenting education, nonviable visitation schedules) were identified. There were no cases in which there existed “no clinical indication” for the addition of one or more supplemental interventions in one or more of these categories, that is, over and above care as usual being provided by the child welfare system. A majority of birth parents manifested mental disorders, developmental disorders, or substance use disorders (see
Table 1); for most of these, there were gaps in what would be considered standard treatment for these disorders, and 20% directly received adult psychiatric care in SYNCHRONY. Twelve percent of the children were referred for individual psychotherapy (provided by SYNCHRONY in approximately half of the cases), 33% were newly diagnosed with a developmental disorder for which developmental therapies (usually state-supported) were initiated, 10% received pharmacotherapy via SYNCHRONY, and 30% manifested clinical indications for family therapy (all provided by SYNCHRONY). In total, 67% were recognized as being in need of one or more of these clinically indicated interventions. Of the remaining cases, initial medical recommendations included either substantive reduction (one-third) or liberalization (two-thirds) in the frequency of visitation with birth parents. Case examples of the provision of supplemental interventions and the respective children’s outcomes are presented in
Table 3.
Results of Serial Assessment of Children in the SYNCHRONY Project
Over the course of the families’ enrollment, Children’s Global Assessment Scale scores steadily improved, irrespective of the timing of enrollment of the child in the program relative to the timing of his or her placement in protective custody (which varied from days to years across cases, as shown in
Table 4, such that the observed improvement of the cohort would be inconsistent with an exclusive effect of regression toward the mean). On average, over the time from baseline evaluation to the most recent available follow-up, the mean change in Children’s Global Assessment Scale score for children in the program was 8.15 (t=5.66, df=90, p<0.001), which is highly clinically and statistically significant, representing an effect size of approximately 0.6. This improvement occurred, on average, irrespective of whether or not children were ultimately reunified with their birth parents.
Among cases closed to date, the trends for scores on the Caregiver-Child Social-Emotional Relationship Rating Scale were reflective of ultimate disposition: among closed cases in which the child was reunified with the birth parents, scores significantly improved from baseline to the most recent available measurement. In this group, most of the parents attended evidence-based parent training, most graduated, and the improvement in scores was observed over the course of the time they participated in parent training (p<0.05). In contrast, among closed cases in which the child and birth parents were not reunified, an opposite picture emerged: scores exhibited a trend for deterioration over the course of the families’ involvement in the program (see
Table 4). Many were nonadherent with parent training, with infrequent attendance, and few graduated. Incredible Years Parenting Scale test scores revealed baseline levels of verbosity, laxness, and overreactivity commensurate with published means for parents of school-age children with disruptive behavior disorders enrolled in Incredible Years clinical trials; total scores improved significantly, as detailed in
Table 4.
Conclusions
In this voluntary support program, two-generation psychiatric care and evidence-based parenting education were successfully delivered to families of young children in protective custody to supplement care as usual in the child welfare system and to offset risk for maltreatment recidivism. Such services were in short supply, and their delivery was minimally reimbursed by Medicaid. As first observed by Zeanah et al. (
10), this St. Louis quasi-replication was readily accepted by most families (who were often but not always highly motivated by the prospect of reunification with their children), embraced collaboratively by both the Family Court and the Missouri Department of Social Services, and, for the vast majority of cases, resulted in the delivery of medically indicated services that had otherwise not been implemented in the course of usual care. SYNCHRONY Project parents who actively participated in evidence-based parenting education made substantial gains from severely abnormal baseline scores both on the direct clinical observations of sensitive-responsive caregiving behavior and by their own self-appraisal on the Incredible Years Parenting Scale, and children made substantial gains from abnormal baseline scores on clinical assessments of adaptive functioning, irrespective of the timing of enrollment relative to the date of placement in protective custody. Abuse recidivism among program participants has been extremely low to date, and it has remained low for children who have been successfully reunified with their parents. To deliver medically indicated care and to integrate that care with the work of the child welfare system, this program required government subsidy over and above Medicaid reimbursement rates on the order of $1,500 per child per year.
The positive outcomes that were observed occurred in some cases as a function of intensified support of families over the course of the reunification process, and in other cases as a function of serial clinical observations that raised warning signs that an impending reunification was unsafe and should be deferred until one or both birth parents could reasonably demonstrate capacity to meet the needs of their children’s mental health and development (examples of both are provided in
Table 3). Regarding the latter, such observations were communicated to the court and often led to higher levels of surveillance by both the courts and the Missouri Department of Social Services. When cross-system observation consistently revealed an inability of birth parents to meet critical needs of their children and exhaustive attempts (across systems) to remedy the observed risks failed, the clinical observations of the SYNCHRONY project could ultimately lead to a recommendation of termination of parental rights as the mechanism by which maltreatment recidivism was averted.
It will require randomized controlled trials of court-based implementation of two-generation psychiatric care to ascertain precisely the magnitude and cost-efficacy of improvement in outcome over care as usual conferred by this supplemental program. Such trials, however, are extremely difficult to conduct feasibly in the setting of the immediate aftermath of placement of a young child in protective custody. Approaching young parents who have lost custody of their children to engage in research in which they would be randomized to mental health support could be construed as ethically inappropriate, and the randomization of children in protective custody would require consent from the state (their legal guardian) to enroll them in randomized controlled trials. This inherent difficulty with more rigorous study designs strongly motivates our reporting of this promising open trial in an effort to contribute to an evidentiary base for more appropriate allocation of U.S. government resources, in favor of targeted intervention for the mental health support of children and families indexed (by the event of placement in protective custody) for extreme high risk for one of the most deleterious known environmental causes of child psychopathology, which is recurrent child maltreatment.
Acknowledgments
The authors acknowledge financial support for the intervention program provided by the St. Louis County Children’s Service Fund and a philanthropic gift from an anonymous donor to the Washington University School of Medicine. They also acknowledge the extraordinary efforts of the clinical team who collaborated with the authors in implementing the program, including Ann McAndrew, L.P.C., Molly McGrath, M.S.W., Jennifer Holzhauer, M.S.W., Megan Panther, M.B.A., Caroline Wheatley, M.S.W., Lara Oakley, Sandy Polanc, Laura Pons, M.S.W., Angela Klocke, R.N., and a succession of resident physicians-in-training who assisted the authors in delivering the clinical interventions. The authors also acknowledge their dedicated colleagues in the St. Louis County Family Court, including Carol Bader, J.D., Kip Seely, and Michael Burton, J.D., as well as their colleagues in the Missouri Department of Social Services, whose partnership made the program possible. Finally, the authors acknowledge those parents and caregivers of children in the program, including birth parents, foster parents, and small villages of devoted family members, who rose to the occasion of the crises involving the young children enrolled, faithfully (usually very patiently) engaged in the intervention process, and inspired the members of the intervention team.