The Effect of Concomitant Treatment With SSRIs and Statins: A Population-Based Study
Publication: American Journal of Psychiatry
Abstract
Objective:
Both preclinical studies and clinical trials have indicated that the combination of a selective serotonin reuptake inhibitor (SSRI) and a statin may have superior antidepressant effects compared with SSRI treatment alone. The authors sought to assess whether this beneficial effect can be generalized to a more heterogeneous population of SSRI users.
Method:
In a nationwide cohort study that included all incident SSRI users in Denmark between 1997 and 2012, the authors compared people who had periods of concomitant use of SSRIs and statins with people who had periods of SSRI treatment alone. Outcomes included the rates of psychiatric hospital contacts (any cause), psychiatric hospital contacts due to depression, suicidal behavior, and all-cause mortality. Using Cox regression and competing risk analysis, the authors calculated crude and adjusted hazard ratios for these outcomes.
Results:
The authors identified 872,216 incident SSRI users, of whom 113,108 (13.0%) used a statin concomitantly. Compared with SSRI treatment alone, the combined use of an SSRI and a statin was associated with a significantly lower risk for both psychiatric hospital contacts (adjusted hazard ratio=0.75 (95% CI=0.69, 0.82) and psychiatric hospital contacts due to depression (adjusted hazard ratio=0.64, 95% CI=0.55, 0.75). Compared with SSRI treatment alone, the concomitant use of SSRIs and statins was not associated with significant increases in all-cause mortality (adjusted hazard ratio=1.04, 95% CI=0.96, 1.12) or suicidal behavior (adjusted hazard ratio=0.85, 95% CI=0.61, 1.18).
Conclusions:
In a large naturalistic cohort, concomitant treatment with SSRIs and statins resulted in robust advantages compared with SSRIs alone.
Remission rates for patients with depression are modest despite treatment with antidepressants at adequate dosages for sufficient duration (1). Even after switching to other antidepressants, augmenting with additional antidepressants, or undergoing adjunctive psychotherapy, a large proportion of patients experience only partial response or no response at all (2). Therefore, alternative strategies to relieve depression have been investigated intensively in recent decades (3).
One such strategy, which has shown some promise, is treatment with anti-inflammatory agents. The “inflammatory hypothesis” for depression has been revived in recent years (4) in the wake of large studies linking inflammatory processes with the emergence of depression (5, 6). Also, a series of clinical trials indicated that anti-inflammatory drugs such as selective cyclooxygenase-2 (COX-2) inhibitors (7) and aspirin (8) may have antidepressant effects (9).
Despite being used primarily for their lipid-lowering properties, statins have direct anti-inflammatory effects that are not mediated by their hypocholesterolemic activity (10). Therefore, the potential impact of statins on depression has also been investigated. Some studies have pointed to either depressogenic (11) or neutral effects (12), and others have suggested that statins have antidepressant properties (13, 14) independent of their cholesterol-lowering effect (15). These observations have inspired researchers to test the antidepressant effect of statins in combination with typical first-line antidepressants, namely, the selective serotonin reuptake inhibitors (SSRIs). Indeed, results from studies in both animals (16) and humans (17) indicate that the combination of an SSRI and a statin has superior antidepressant effect compared with treatment with an SSRI alone. However, it remains unknown whether the effect observed in these initial studies can be generalized to more heterogeneous populations of SSRI users. The aim of this study was to test the comparative effectiveness and safety of SSRI treatment with or without concomitant use of statins, based on a large population-based cohort of unselected SSRI users.
Method
This was a register-based nationwide cohort study based on the entire Danish population (approximately 5.5 million inhabitants). Data were obtained by register linkage via the unique personal registration numbers that are assigned to all Danish residents at the time of birth or with the achievement of residency (18). The study included data from several nationwide registers, which are described below. The use of the data was approved by the Danish Data Protection Agency, the Danish National Board of Health, and Statistics Denmark.
Study Population
The study population was defined as all incident SSRI (Anatomical Therapeutic Chemical [ATC] code N06AB) users in Denmark between Jan. 1, 1997, and Dec. 31, 2012 (with no use between Jan. 1, 1996, and Dec. 31, 1996). SSRI use was defined as redemption of at least one prescription for an SSRI identified through the Danish National Prescription Registry (19), which contains information on all prescribed drugs picked up at pharmacies throughout Denmark. For each transaction, the ATC code is registered along with the number and dose of pills and the date of the transaction.
Assessment of Statin Use
The use of statins among SSRI users was also assessed through the Danish National Prescription Registry based on redemptions of prescriptions for the following drugs: simvastatin (ATC codes C10AA01 and C10BA02), lovastatin (C10AA02), pravastatin (C10AA03), fluvastatin (C10AA04), atorvastatin (C10AA05), and rosuvastatin (C10AA07). Only incident statin users (no use of statins in the year preceding the day of redemption of the first SSRI prescription) were included in the study population.
Dose and Duration of Treatment
For both the SSRIs and the statins, the treatment duration was estimated on the basis of the prescribed number and dose of pills and the Defined Daily Dose (DDD) (http://www.whocc.no/ddd). The estimated treatment duration for each prescription was calculated as follows: treatment duration (days) = ([number of packages × number of pills per package × dose of pills] / DDD) × 1.15 + 7. The multiplication factor of 1.15 and the addition of 7 days were included because these extensions of the treatment period are in closer agreement with actual drug consumption in clinical practice (20).
Time at Risk and Follow-Up
For the analysis of the effect of concomitant SSRI and statin use, follow-up started on the day of redemption of the first SSRI prescription (the index date). Individuals who redeemed a prescription for a statin during follow-up shifted to contribute “time at risk” to the SSRI-plus-statin group from the date of this redemption. Individuals shifted back to contribute time at risk to the SSRI-only group if the SSRI treatment lasted longer than the statin treatment. Censoring occurred due to discontinuation of SSRI treatment, switching between different statins, emigration, completion of 3 years of follow-up, or end of the study period (Dec. 31, 2013), whichever came first. Individuals were only included once in the study.
Definition of Outcomes
Four outcomes, two related to psychiatric hospital contacts and two related to adverse events, were considered in order to evaluate the effect of concomitant treatment with SSRIs and statins compared with SSRI treatment alone:
Psychiatric hospital contacts (any cause) were defined as the assignment of a diagnosis of a mental disorder (as defined in chapter V in ICD-10) after an inpatient, outpatient, or emergency department contact with a psychiatric hospital in Denmark. The diagnoses used to define this variable were extracted from the Danish Psychiatric Central Research Register, which contains complete electronic records of all psychiatric diagnoses assigned at psychiatric hospitals in Denmark since 1969 (21, 22).
Psychiatric hospital contacts specifically due to depression were defined as the assignment of a main diagnosis of depression (ICD-10 codes F32 or F33) after an inpatient, outpatient, or emergency department contact with a psychiatric hospital in Denmark. This variable was also based on diagnoses extracted from the Danish Psychiatric Central Research Register.
Using diagnoses of mental illness assigned in relation to hospital contacts as a proxy for the development or worsening of existing mental illness is a well-established practice in register-based research (5, 21–23).
Suicidal behavior was defined as either a suicide or a suicide attempt. Cases of suicide were identified in the Cause of Death Register (24), and suicide attempts were identified through the Danish National Patient Register (25) and the Danish Psychiatric Central Research Register (22). Both suicide and suicide attempts were defined by ICD-10 codes X60–X84 (26).
All-cause mortality was assessed through the Danish Civil Registration System (18).
Assessment of Covariates
The sociodemographic covariates were sex, age, and education level. Education level was divided into six levels: primary school, secondary school, vocational education, short higher education, medium higher education, and university degree (27).
Diagnoses of mental disorders prior to the index date (data from 1969 onward) were also included as covariates (based on information from the Danish Central Psychiatric Research Register [22]). Similarly, hospital diagnoses of medical diseases prior to the index date (data from 1977 onward) were included as covariates based on diagnoses recorded in the Danish National Patient Register (25). For both registers, ICD-8 was used as the diagnostic reference until Jan. 1, 1994, when it was replaced by ICD-10 (ICD-9 was not implemented in Denmark). The mental disorder covariates were defined as follows, based on both main and auxiliary diagnoses: mental and behavioral disorders due to psychoactive substance abuse (ICD-8 codes 291.x9, 294.39, 303.x9, 303.20, 303.28, 303.90, 304.x9; ICD-10 codes F10–F19), schizophrenia and related disorders (ICD-8 codes 295.x9, 296.89, 297.x9, 298.29–298.99, 299.04, 299.05, 299.09, 301.83; ICD-10 codes F20–F29), bipolar disorder (ICD-8 codes 296.19, 296.39, 298.19; ICD-10 codes F30–F31), single and recurrent depressive disorder (ICD-8 codes 296.09, 296.29, 298.09, 300.49; ICD-10 codes F32–F33), neurotic, stress-related, and somatoform disorders (ICD-8 codes 300.x9 [excluding 300.49], 305.x9, 305.68, 307.99; ICD-10 codes F40–F48), and other mental disorders (all diagnoses other than those mentioned above). The covariates regarding medical diseases were defined in accordance with the Charlson comorbidity index (28) modified for use with the ICD-10 (29). The 19 medical diseases considered in the Charlson comorbidity index (myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, connective tissue disease, ulcer disease, mild liver disease, diabetes, hemiplegia, moderate to severe renal disease, diabetes with end organ damage, any tumor, leukemia, lymphoma, moderate to severe liver disease, metastatic solid tumor, AIDS) were included as individual covariates (based on main diagnoses only).
Since the potential antidepressant effect of statins may be mediated through the anti-inflammatory properties of this class of drugs, the following anti-inflammatory medications, used within the year preceding the index date, were included as covariates: corticosteroids (ATC codes H02A and H02B), anti-inflammatory/antirheumatic agents (M01B and M01C), and nonsteroidal anti-inflammatory drugs (NSAIDs) (M01A and N02BA). Despite not having anti-inflammatory properties, low-dose aspirin (B01AC06) was included in the group of NSAIDs because it has been suggested to have an antidepressant effect as well (23). To adjust for potential confounding effects of other medications prescribed for medical conditions related to statin use, the following classes of drugs, used within the year preceding the index date, were included as covariates: antihypertensives (ATC code C02), diuretics (C03), peripheral vasodilators (C04), vasoprotective agents (C05), beta-blockers (C07), calcium channel blockers (C08), agents acting on the renin-angiotensin system (C09), and lipid-modifying agents other than statins (C10 excluding C10AA and C10BA02). Furthermore, to adjust for use of other psychopharmaceuticals, the following classes of drugs, used within the year preceding the index date, were included as covariates: antidepressants other than SSRIs (ATC code N06A excluding N06AB), antipsychotics (N05A excluding N05AN), lithium (N05AN), other mood stabilizers (oxcarbazepine, carbamazepine, lamotrigine, valproate; N03AF02, N03AF01, N03AX09, N03AG01), anxiolytics (N05BA, N05CD02, N05CD05, N05CD06, N03AX16), and benzodiazepine-like hypnotics (N05CF01, N05CF02).
Statistical Analysis
Main analyses.
Cox proportional hazard regression analyses were performed to calculate hazard ratios for the four outcomes: psychiatric hospital contact, psychiatric hospital contact due to depression, suicidal behavior, and all-cause mortality. The time since first SSRI prescription (index date) was used as underlying time scale. The crude analyses were adjusted for age (with linear splines to ensure proportional hazards) and sex. The fully adjusted analyses were adjusted for the following covariates: age (with linear splines), sex, education level, previous diagnoses of mental disorders or medical diseases, previous suicide attempts (defined as described under the definition of outcomes), start year of SSRI treatment, and use of the following drugs in the year prior to the index date (dichotomously defined: yes/no): corticosteroids, anti-inflammatory/antirheumatic agents, NSAIDs, antihypertensives, diuretics, peripheral vasodilators, vasoprotective agents, beta-blockers, calcium channel blockers, agents acting on the renin-angiotensin system, lipid-modifying agents other than statins, antidepressants other than SSRIs, antipsychotics, lithium, other mood stabilizers, anxiolytics, and benzodiazepine-like hypnotics. For all Cox analyses, the proportional hazards assumption was tested based on Schoenfeld’s residuals. The assumption was met in all analyses.
In the primary analyses, SSRI-only users were compared with users of SSRIs who were concomitantly taking statins. Furthermore, since citalopram is the most commonly prescribed SSRI and simvastatin the most commonly prescribed statin in Denmark, we tested the effect of concomitant citalopram-simvastatin use compared with citalopram treatment alone. We also tested the effect of concomitant treatment with any SSRI and simvastatin, and any SSRI with any statin other than simvastatin, respectively, to treatment with any SSRI alone. In these specific analyses, censoring also occurred if there was a switch in treatment from one statin to another. Finally, to illustrate the cumulative hazard over time, we graphed cumulative events (i.e., psychiatric hospital contacts in general and those specifically due to depression), based on competing risk analyses using the Fine and Gray model (30) with death as the competing risk.
Propensity-score matched analyses.
To verify that the results of the main analyses were not accounted for by potential confounding by indication associated with the nonexperimental design of the study, we carried out propensity-score matched analyses analog to the main analyses. These analyses are described in detail in the data supplement that accompanies the online edition of this article.
Sensitivity analyses.
A number of sensitivity analyses (of the Cox proportional hazard regression analyses) were carried out to test the robustness of the associations. The first consisted of repeating the main analyses, but with the treatment duration defined without the multiplication factor of 1.15 and the addition of 7 days. The analyses were also repeated within the age groups 10–49 years, 50–69 years, and 70–109 years, stratified by sex. Since prior contacts at psychiatric hospitals could increase the risk for subsequent contacts, we also reran the main analyses excluding SSRI users with a history of such contacts. Finally, we repeated the main analyses after excluding individuals diagnosed with any of the medical diseases included in the Charlson comorbidity index.
All statistical analyses were performed with Stata, release 13 (Stata Corp, College Station, Tex.) at Statistics Denmark via remote access.
Results
For the period from 1997 through 2012, we identified 872,216 incident SSRI users. The most frequently used SSRIs were citalopram (57.2%), sertraline (17.1%), and escitalopram (11.4%). The total follow-up time—that is, the treatment period for the SSRIs—was 642,058 person-years. Among the 872,216 SSRI users, 113,108 (13.0%) used a statin concomitantly (simvastatin, 12.0%; atorvastatin, 0.6%; pravastatin, 0.2%; rosuvastatin, 0.1%; fluvastatin, 0.04%; and lovastatin, 0.02%), resulting in a follow-up time of SSRI plus statin use of 73,142 person-years. See Figure 1 for an overview of the study design.
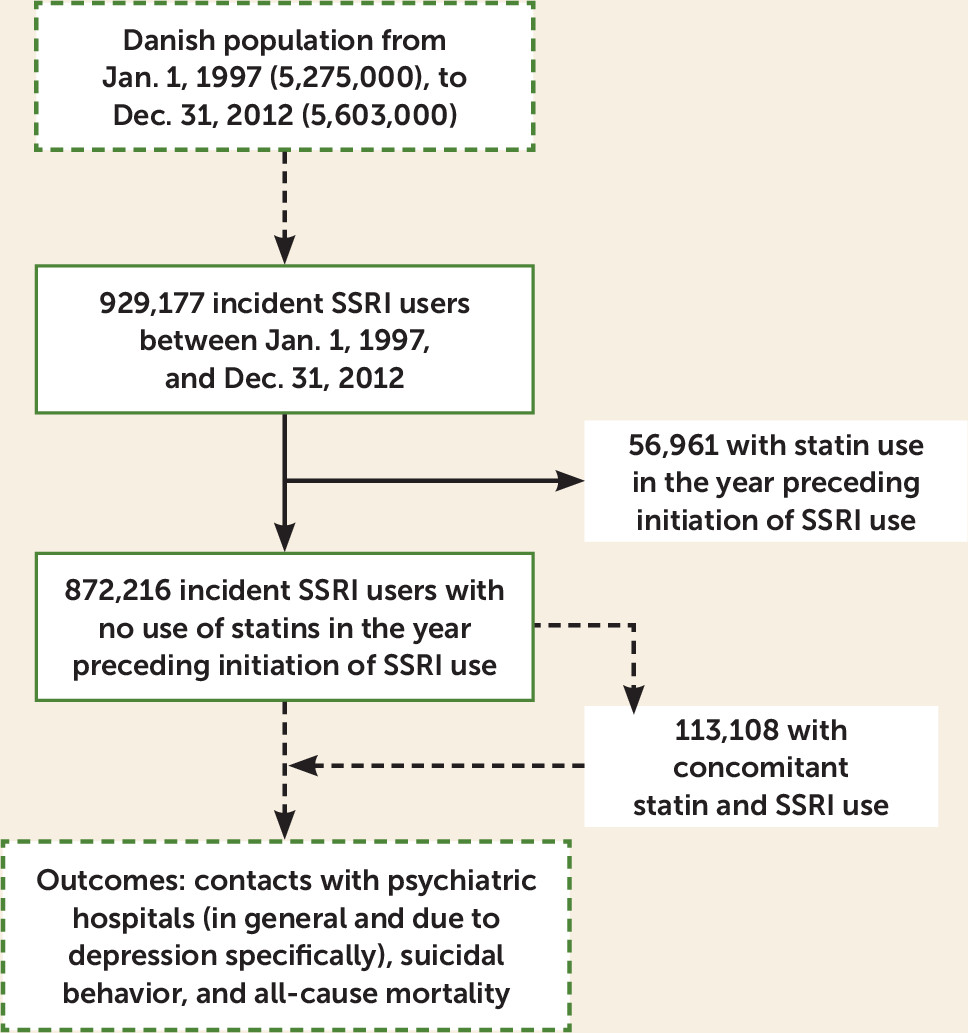
FIGURE 1. Flowchart Illustrating the Design of a Study of the Effect of Concomitant Treatment With SSRIs and Statinsa
a Source: Statistics Denmark. SSRIs=selective serotonin reuptake inhibitors.
Table 1 summarizes the clinical and sociodemographic characteristics of the overall sample and of individuals using an SSRI alone and those using an SSRI and a statin. On average, statin users were older and had less psychiatric morbidity, more use of psychopharmaceuticals, more medical morbidity, and more use of medication for cardiovascular disease.
| Characteristic | All SSRI Users (N=872,216) | Users of SSRIs Only (N=759,108) | Concomitant Users of SSRIs and Statins (N=113,108) | |||
|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Median | IQR | |
| Age (years) | 48.0 | 33.4, 67.8 | 45.7 | 31.6, 68.2 | 56.2 | 47.2, 66.5 |
| N | % | N | % | N | % | |
| Female | 536,019 | 61.6 | 469,623 | 62.0 | 66,396 | 58.7 |
| Age groups (years) | ||||||
| 10–29 | 170,862 | 19.6 | 168,443 | 22.2 | 2,419 | 2.1 |
| 30–49 | 291,312 | 33.5 | 257,649 | 34.0 | 33,663 | 29.8 |
| 50–69 | 210,151 | 24.1 | 153,881 | 20.3 | 56,270 | 49.8 |
| 70–89 | 181,265 | 20.8 | 160,757 | 21.2 | 20,508 | 18.1 |
| ≥90 | 17,311 | 2.0 | 17,080 | 2.3 | 231 | 0.2 |
| Education | ||||||
| Primary school | 366,930 | 42.1 | 314,756 | 41.5 | 52,174 | 46.1 |
| Secondary school | 33,570 | 3.9 | 31,871 | 4.2 | 1,699 | 1.5 |
| Vocational | 1,722 | 0.2 | 1,578 | 0.2 | 144 | 0.1 |
| Short higher | 204,268 | 23.5 | 171,519 | 22.6 | 32,749 | 29.0 |
| Medium higher | 130,016 | 14.9 | 113,110 | 14.9 | 16,906 | 15.0 |
| University | 134,395 | 15.4 | 124,976 | 16.5 | 9,419 | 8.2 |
| Index year | ||||||
| 1997 | 64,521 | 7.4 | 51,747 | 6.8 | 12,774 | 11.3 |
| 1998 | 58,104 | 6.7 | 47,117 | 6.2 | 10,987 | 9.7 |
| 1999 | 51,369 | 5.9 | 41,793 | 5.5 | 9,576 | 8.5 |
| 2000 | 53,083 | 6.1 | 43,675 | 5.8 | 9,408 | 8.3 |
| 2001 | 60,366 | 6.9 | 49,705 | 6.6 | 10,661 | 9.4 |
| 2002 | 57,744 | 6.6 | 47,756 | 6.3 | 9,988 | 8.8 |
| 2003 | 63,743 | 7.3 | 53,479 | 7.0 | 10,264 | 9.1 |
| 2004 | 52,327 | 6.0 | 44,530 | 5.9 | 7,797 | 6.9 |
| 2005 | 56,112 | 6.4 | 48,651 | 6.4 | 7,461 | 6.6 |
| 2006 | 56,209 | 6.4 | 49,664 | 6.5 | 6,545 | 5.8 |
| 2007 | 54,772 | 6.3 | 49,145 | 6.5 | 5,627 | 5.0 |
| 2008 | 51,094 | 5.9 | 47,107 | 6.2 | 3,987 | 3.5 |
| 2009 | 54,348 | 6.2 | 51,018 | 6.7 | 3,330 | 2.9 |
| 2010 | 55,061 | 6.3 | 52,537 | 6.9 | 2,524 | 2.2 |
| 2011 | 43,324 | 5.0 | 41,887 | 5.5 | 1,437 | 1.3 |
| 2012 | 40,039 | 4.6 | 39,297 | 5.2 | 742 | 0.7 |
| Previous mental disorders | ||||||
| Any contact | 169,436 | 19.4 | 151,918 | 20.0 | 17,518 | 15.5 |
| Depression | 45,746 | 5.3 | 40,806 | 5.4 | 4,940 | 4.4 |
| Schizophrenia spectrum | 22,870 | 2.6 | 20,450 | 2.7 | 2,420 | 2.1 |
| Bipolar disorder | 5,828 | 0.7 | 5,204 | 0.7 | 624 | 0.6 |
| Anxiety | 24,188 | 2.8 | 21,563 | 2.9 | 2,625 | 2.3 |
| Substance abuse | 35,239 | 4.1 | 30,636 | 4.0 | 4,603 | 4.1 |
| Other mental disorders | 68,939 | 7.9 | 62,799 | 8.3 | 6,140 | 5.4 |
| Previous medical diseases | ||||||
| Any disorder | 210,968 | 24.2 | 180,206 | 23.8 | 30,762 | 27.2 |
| Myocardial infarction | 20,724 | 2.4 | 17,119 | 2.3 | 3,605 | 3.2 |
| Congestive heart failure | 13,732 | 1.6 | 12,409 | 1.6 | 1,323 | 1.2 |
| Peripheral vascular disease | 19,669 | 2.3 | 16,292 | 2.2 | 3,377 | 3.0 |
| Cerebrovascular disease | 21,850 | 2.5 | 18,194 | 2.4 | 3,656 | 3.2 |
| Dementia | 9,870 | 1.1 | 9,433 | 1.2 | 437 | 0.4 |
| Chronic pulmonary disease | 53,420 | 6.1 | 46,860 | 6.2 | 6,560 | 5.8 |
| Connective tissue disease | 19,191 | 2.2 | 16,592 | 2.2 | 2,699 | 2.4 |
| Ulcer disease | 28,143 | 3.2 | 23,818 | 3.1 | 4,325 | 3.8 |
| Mild liver disease | 7,672 | 0.9 | 6,755 | 0.9 | 917 | 0.8 |
| Diabetes | 16,492 | 1.9 | 12,048 | 1.6 | 4,444 | 3.9 |
| Hemiplegia | 1,499 | 0.2 | 1,338 | 0.2 | 161 | 0.1 |
| Moderate to severe renal disease | 7,643 | 0.9 | 6,625 | 0.9 | 1,018 | 0.9 |
| Diabetes with end organ damage | 8,775 | 1.0 | 6,406 | 0.9 | 2,369 | 2.1 |
| Any tumor | 63,169 | 7.3 | 56,441 | 7.5 | 6,728 | 6.0 |
| Leukemia | 1,677 | 0.2 | 1,543 | 0.2 | 134 | 0.1 |
| Lymphoma | 3,661 | 0.4 | 3,316 | 0.4 | 345 | 0.3 |
| Liver disease | 722 | 0.1 | 647 | 0.1 | 75 | 0.1 |
| Metastatic solid tumor | 6,977 | 0.8 | 6,685 | 0.9 | 292 | 0.3 |
| AIDS | 897 | 0.1 | 784 | 0.1 | 113 | 0.1 |
| Previous cardiovascular drug use | ||||||
| Any use | 263,535 | 30.2 | 217,183 | 28.6 | 46,352 | 41.0 |
| Diuretics | 150,993 | 17.9 | 126,743 | 17.4 | 24,250 | 21.5 |
| Renin-angiotensin system drugs | 85,517 | 10.1 | 67,389 | 9.2 | 18,128 | 16.1 |
| Beta-blockers | 78,850 | 9.4 | 63,108 | 8.6 | 15,742 | 14.0 |
| Calcium channel blockers | 65,827 | 7.8 | 52,610 | 7.2 | 13,217 | 11.7 |
| Vasoprotective agents | 40,773 | 4.8 | 35,102 | 4.8 | 5,671 | 5.0 |
| Antihypertensives | 4,524 | 0.5 | 3,610 | 0.5 | 914 | 0.8 |
| Other lipid-modifying agents | 1,807 | 0.2 | 1,434 | 0.2 | 373 | 0.3 |
| Peripheral vasodilators | 263 | <0.1 | 214 | <0.1 | 49 | 0.04 |
| Previous anti-inflammatory drug use | ||||||
| Any use | 749,141 | 85.9 | 643,769 | 84.8 | 105,372 | 93.2 |
| Corticosteroids | 265,885 | 31.5 | 219,032 | 30.0 | 46,853 | 41.5 |
| Antirheumatics | 259 | <0.1 | 211 | <0.1 | 48 | 0.04 |
| NSAIDs | 708,611 | 84.1 | 607,206 | 83.2 | 101,405 | 89.9 |
| Low-dose aspirin | 92,814 | 11.0 | 78,529 | 10.8 | 14,285 | 12.7 |
| Previous psychopharmaceutical use | ||||||
| Any use | 591,443 | 67.8 | 502,086 | 66.1 | 89,357 | 79.0 |
| Antidepressants other than SSRIs | 80,583 | 9.6 | 68,686 | 9.4 | 11,897 | 10.5 |
| Antipsychotics | 67,238 | 8.0 | 59,069 | 8.1 | 8,169 | 7.2 |
| Lithium | 2,853 | 0.3 | 2,512 | 0.3 | 341 | 0.3 |
| Other mood stabilizers | 64,471 | 7.7 | 54,225 | 7.4 | 10,246 | 9.1 |
| Anxiolytics | 466,321 | 55.3 | 391,949 | 53.7 | 74,372 | 65.9 |
| Benzodiazepine-like hypnotics | 297,208 | 35.3 | 249,463 | 34.2 | 47,745 | 42.3 |
a
IQR=interquartile range; NSAIDs=nonsteroidal anti-inflammatory agents; SSRI=selective serotonin reuptake inhibitor.
Effects on Psychiatric Hospital Contacts
Concomitant use of an SSRI and a statin was associated with a decreased risk for both psychiatric hospital contacts in general (adjusted hazard ratio=0.75, 95% CI=0.69, 0.82) and for psychiatric hospital contacts due to depression specifically (adjusted hazard ratio=0.64, 95% CI=0.55, 0.75) compared with the use of an SSRI alone. Simvastatin was, by far, the most commonly used statin. The risk for both psychiatric hospital contacts in general and contacts due to depression were reduced significantly when SSRIs were used in combination with either simvastatin or any of the statins in the composite group of “other statins” (see Table 2). The same was the case for the citalopram-simvastatin combination compared with citalopram alone.
| Outcome and Medication Group | Nb (events) | Person-Years | Crude Hazard Ratioc | 95% CI | Adjusted Hazard Ratiod | 95% CI |
|---|---|---|---|---|---|---|
| Contacts with psychiatric hospitals (any cause) | ||||||
| SSRI alone | 78,023 | 514,810 | 1.0 | Ref. | 1.0 | Ref. |
| SSRI plus a statin | 11,883 | 73,142 | 0.65 | 0.60, 0.71 | 0.75 | 0.69, 0.82 |
| Simvastatin | 11,228 | 67,371 | 0.65 | 0.60, 0.72 | 0.76 | 0.70, 0.83 |
| Other statinse | 655 | 5,771 | 0.61 | 0.45, 0.83 | 0.66 | 0.49, 0.89 |
| Citalopram only | 40,202 | 268,368 | 1.0 | Ref. | 1.0 | Ref. |
| Citalopram plus simvastatin | 5,677 | 32,856 | 0.60 | 0.53, 0.67 | 0.72 | 0.64, 0.81 |
| Contacts with psychiatric hospitals due to depression | ||||||
| SSRI alone | 29,231 | 521,998 | 1.0 | Ref. | 1.0 | Ref. |
| SSRI plus a statin | 3,937 | 74,226 | 0.59 | 0.50, 0.68 | 0.64 | 0.55, 0.75 |
| Simvastatin | 3,720 | 69,044 | 0.60 | 0.51, 0.70 | 0.66 | 0.56, 0.77 |
| Other statinse | 217 | 5,182 | 0.49 | 0.28, 0.86 | 0.54 | 0.30, 0.94 |
| Citalopram only | 15,178 | 290,674 | 1.0 | Ref. | 1.0 | Ref. |
| Citalopram plus simvastatin | 2,028 | 33,154 | 0.58 | 0.48, 0.71 | 0.66 | 0.54, 0.80 |
| All-cause mortality | ||||||
| SSRI alone | 36,035 | 520,380 | 1.0 | Ref. | 1.0 | Ref. |
| SSRI plus a statin | 4,040 | 73,467 | 1.00 | 0.93, 1.08 | 1.04 | 0.96, 1.12 |
| Simvastatin | 3,833 | 68,818 | 1.00 | 0.92, 1.07 | 1.02 | 0.95, 1.10 |
| Other statinse | 207 | 4,649 | 0.99 | 0.89, 1.51 | 1.24 | 0.95, 1.62 |
| Citalopram only | 25,911 | 303,712 | 1.0 | Ref. | 1.0 | Ref. |
| Citalopram plus simvastatin | 2,065 | 30,981 | 0.98 | 0.90, 1.06 | 1.02 | 0.94, 1.11 |
| Suicidal behavior | ||||||
| SSRI alone | 6,746 | 528,374 | 1.0 | Ref. | 1.0 | Ref. |
| SSRI plus a statin | 469 | 74,189 | 0.79 | 0.56, 1.10 | 0.85 | 0.61, 1.18 |
| Simvastatin | 426 | 68,395 | 0.79 | 0.56, 1.12 | 0.85 | 0.60, 1.20 |
| Other statinse | 43 | 5,794 | 0.74 | 0.24, 2.31 | 0.81 | 0.26, 2.52 |
| Citalopram only | 3,350 | 226,355 | 1.0 | Ref. | 1.0 | Ref. |
| Citalopram plus simvastatin | 321 | 30,251 | 0.62 | 0.39, 0.99 | 0.65 | 0.41, 1.04 |
a
Numbers in boldface represent statistically significant results. SSRI=selective serotonin reuptake inhibitor.
b
The crude analyses were based on the number of events listed here, and the adjusted analyses were based on slightly fewer events: contacts with psychiatric hospitals, 286 less for any SSRI and 156 less for citalopram; contacts with psychiatric hospitals due to depression, 89 less for any SSRI and 50 less for citalopram; all-cause mortality, 51 less for any SSRI and 28 less for citalopram; suicidal behavior, 44 less for any SSRI and 22 less for citalopram.
c
Adjusted for age and sex.
d
Adjusted for age, sex, education level, SSRI index year, previous contacts for mental disorders and medical diseases, and use of other anti-inflammatory medications, cardiovascular protective medications, and psychopharmaceuticals within the year preceding the SSRI index date.
e
The other statins were lovastatin, pravastatin, fluvastatin, atorvastatin, and rosuvastatin.
Figure 2 illustrates the effect of concomitant use of an SSRI and a statin compared with use of SSRI alone on the cumulative risk of psychiatric hospital contacts in general and contacts due to depression during follow-up.
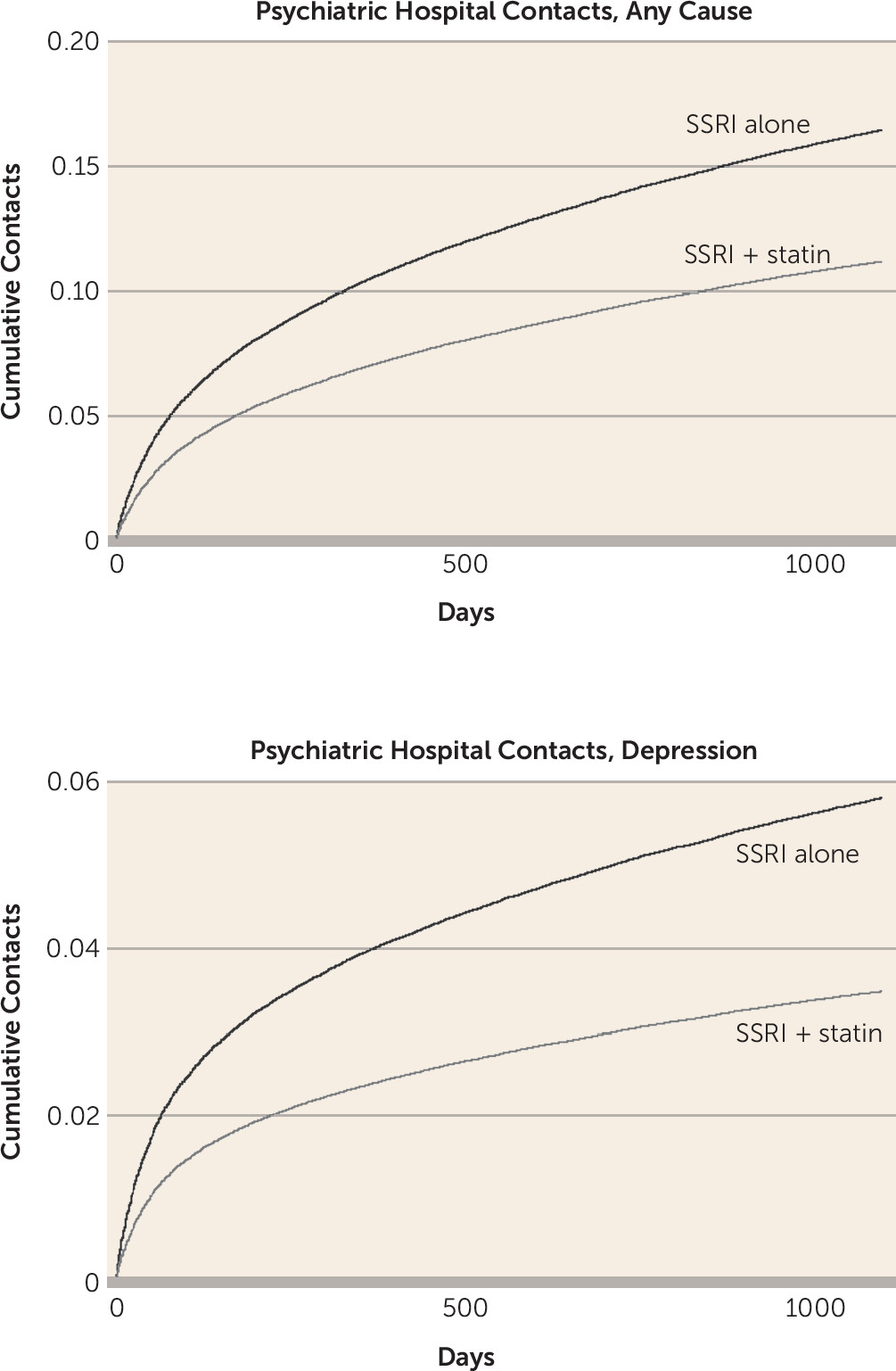
FIGURE 2. Cumulative Psychiatric Hospital Contacts for Any Reason or Due to Depression Specifically Among Individuals Using an SSRI and a Statin Concomitantly, Compared With Individuals Using an SSRI Alonea
a Adjusted for age, sex, education level, SSRI index year, previous contacts for mental disorders and medical diseases, and use of other anti-inflammatory medications, cardiovascular protective medications, and psychopharmaceuticals during the year preceding the SSRI index date. SSRI=selective serotonin reuptake inhibitor.
Adverse Events
Compared with SSRI treatment alone, the concomitant use of SSRIs and statins was not associated with significant increases in all-cause mortality (crude hazard ratio=1.00, 95% CI=0.93, 1.08; adjusted hazard ratio=1.04, 95% CI=0.96, 1.12) or suicidal behavior (crude hazard ratio=0.79, 95% CI=0.56, 1.10; adjusted hazard ratio=0.85, 95% CI=0.61, 1.18). Results were similar for the SSRI plus simvastatin, SSRI plus other statins, and citalopram plus simvastatin combinations (see Table 2).
Propensity-Score Matched Analyses
The results of the propensity-score matched analyses confirmed the results of the main analyses, regarding effects both on psychiatric hospital contacts and on adverse events. The results are available in the online data supplement .
Sensitivity Analyses
All sensitivity analyses supported the results of the main analyses: the direction of the hazard ratios was consistent across sex and age groups, for individuals without prior contacts with psychiatric hospitals, for individuals without prior diagnoses of medical diseases included in the Charlson comorbidity index, and when using the unadjusted equation for defining treatment duration of SSRIs and statins (results not shown).
Discussion
This study was based on a nationwide sample of 872,216 incident SSRI users, of whom 113,108 (13.0%) used a statin concomitantly during a total follow-up of 642,058 person-years. The analyses of this longitudinal data set showed that the combined use of an SSRI and a statin, compared with use of an SSRI alone, was associated with lower risks both for contacts with psychiatric hospitals in general and for contacts with psychiatric hospitals due to depression specifically. These results are consistent with the findings of the only placebo-controlled randomized trial of these two treatment regimens (17). In that trial, the severity of depression, as measured by the Hamilton Depression Rating Scale (HAM-D), decreased significantly more among the participants allocated to fluoxetine (up to 40 mg/day) plus lovastatin (30 mg/day) compared with those receiving fluoxetine plus placebo (reductions of 12.8 and 8.2 points, respectively, on the HAM-D) (17). Since the use of fluoxetine and lovastatin is relatively uncommon in Denmark, our study was not powered to test the effect of this particular combination. The only specific SSRI-statin combination that we were able to investigate in our study was citalopram plus simvastatin compared with citalopram alone, where the combination was associated with lower risk both for contacts with psychiatric hospitals in general and for contacts with psychiatric hospitals due to depression specifically.
A well-known adverse effect of statins is dose-dependent myopathy, which in rare cases may progress to life-threatening rhabdomyolysis (31). Since a subset of the SSRIs (primarily fluvoxamine) inhibit the cytochrome P450 enzymes 3A4 and 2C9, which metabolize simvastatin, lovastatin, atorvastatin, and fluvastatin, the blood levels of these statins may increase during SSRI treatment (32), thereby potentially increasing the risk for rhabdomyolysis (33). In the present study, the use of fluvoxamine was rare (0.12% of the SSRI users were enrolled in the cohort with use of fluvoxamine) and the overall concomitant use of an SSRI (of any type) and a statin (of any type) was not associated with increased mortality when compared with the use of SSRIs alone. This is in accordance with a recent expert review (32) that concluded that “escitalopram, citalopram, and paroxetine are almost certain to be safe in co-therapy with all statins, and rosuvastatin, pitavastatin, and pravastatin are almost certain to be safe in co-therapy with all SSRIs. Other combinations may theoretically be associated with risks, but the magnitude of interaction is likely to be below clinical thresholds.” Our study was underpowered to investigate individual SSRI-statin combinations other than the combined use of citalopram and simvastatin, which is not considered to be associated with clinically relevant drug-drug interactions through the cytochrome P450 system (32), and, accordingly, was not associated with increased mortality in our study. An exploratory analysis of our data showed that the combination of any SSRI and lovastatin was associated with increased mortality (crude hazard ratio=3.21, 95% CI=1.04, 9.96; adjusted hazard ratio=3.58, 95% CI=1.15, 11.10). However, this was based on only four cases of death among the individuals treated with the combination of lovastatin and any SSRI. The SSRIs used in combination with lovastatin by the four deceased individuals could not be investigated because of protection of anonymity.
It has been suggested that lowering cholesterol levels, for instance by means of treatment with statins, may increase the risk for suicidal ideation (34). This would suggest that for a group of individuals who are already at relatively increased risk of suicide, such as those treated with SSRIs due to depression or related psychiatric morbidity, using statins could be hazardous. However, we found no association between concomitant use of SSRIs and statins and increased suicidal behavior. If anything, the results were suggestive of a potential protective effect of the citalopram-simvastatin combination compared with citalopram alone (crude hazard ratio=0.62, 95% CI=0.39, 0.99; adjusted hazard ratio=0.65, 95% CI=0.41, 1.04).
The main strength of this study is the very large nationwide sample, the longitudinal nature of the data, and the high validity of the registers from which we obtained the data used to define the sample (SSRI prescription) (19), the exposure (statin prescription) (19), and the outcomes (psychiatric hospital contacts, suicidal behavior, and mortality) (18, 22, 24, 35, 36). An important limitation of the study is the observational design, which limits the possibilities for causal inference. In that regard, it is important to acknowledge that the statins were not prescribed for their potential antidepressant effect in the present study, but for their anticholesterol properties. Thus, while the psychiatric morbidity of the subjects of the study is unlikely to confound the indication for prescribing statins, the cholesterol profile of the subjects will inherently lead to confounding by indication. However, our analyses were adjusted for a large number of potential confounders, and all sensitivity analyses supported the primary results. Furthermore, the results of the propensity-score matched analyses were consistent with those of the main analyses. However, this does not preclude the existence of residual confounding or bias, so the findings must be interpreted with caution.
Finally, since the psychiatric outcomes in this study were defined based on contacts with psychiatric hospitals, our results are mainly valid for rather severe psychopathology, and less so for milder psychopathology, which may go untreated or may be treated by general practitioners or private practicing psychiatrists.
In conclusion, the results from this large naturalistic cohort study are in accordance with those from prior studies, including a small randomized controlled trial (17), and indicate that the antidepressant potential of the SSRI-statin combination should be subjected to further testing in larger randomized controlled trials. Since the most prevalent SSRI-statin combination in this study was citalopram-simvastatin, which therefore represents the main driving force behind the positive results, we believe that this specific combination would be a good candidate for a head-to-head test against a citalopram-placebo combination in a randomized controlled trial. Finally, although based on very limited numbers, it appears that lovastatin should be used with caution in combination with SSRIs due to potentially increased mortality.
Supplementary Material
File (appi.ajp.2016.15040463.ds001.pdf)
- View/Download
- 517.12 KB
References
1.
Trivedi MH, Rush AJ, Wisniewski SR, et al: Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40
2.
Gaynes BN, Warden D, Trivedi MH, et al: What did STAR*D teach us? Results from a large-scale, practical, clinical trial for patients with depression. Psychiatr Serv 2009; 60:1439–1445
3.
Nierenberg AA: Strategies for achieving full remission when first-line antidepressants are not enough. J Clin Psychiatry 2013; 74:e26
4.
Müller N: Immunology of major depression. Neuroimmunomodulation 2014; 21:123–130
5.
Benros ME, Waltoft BL, Nordentoft M, et al: Autoimmune diseases and severe infections as risk factors for mood disorders: a nationwide study. JAMA Psychiatry 2013; 70:812–820
6.
Wium-Andersen MK, Ørsted DD, Nielsen SF, et al: Elevated C-reactive protein levels, psychological distress, and depression in 73,131 individuals. JAMA Psychiatry 2013; 70:176–184
7.
Abbasi SH, Hosseini F, Modabbernia A, et al: Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: randomized double-blind placebo-controlled study. J Affect Disord 2012; 141:308–314
8.
Almeida OP, Flicker L, Yeap BB, et al: Aspirin decreases the risk of depression in older men with high plasma homocysteine. Transl Psychiatry 2012; 2:e151
9.
Köhler O, Benros ME, Nordentoft M, et al: Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry 2014; 71:1381–1391
10.
Weitz-Schmidt G: Statins as anti-inflammatory agents. Trends Pharmacol Sci 2002; 23:482–486
11.
Zhang X, Norris SL, Gregg EW, et al: Depressive symptoms and mortality among persons with and without diabetes. Am J Epidemiol 2005; 161:652–660
12.
Mansi I, Frei CR, Pugh MJ, et al: Psychologic disorders and statin use: a propensity score-matched analysis. Pharmacotherapy 2013; 33:615–626
13.
Parsaik AK, Singh B, Hassan Murad M, et al: Statins use and risk of depression: a systematic review and meta-analysis. J Affect Disord 2014; 160:62–67
14.
Otte C, Zhao S, Whooley MA: Statin use and risk of depression in patients with coronary heart disease: longitudinal data from the Heart and Soul Study. J Clin Psychiatry 2012; 73:610–615
15.
Young-Xu Y, Chan KA, Liao JK, et al: Long-term statin use and psychological well-being. J Am Coll Cardiol 2003; 42:690–697
16.
Santos T, Baungratz MM, Haskel SP, et al: Behavioral interactions of simvastatin and fluoxetine in tests of anxiety and depression. Neuropsychiatr Dis Treat 2012; 8:413–422
17.
Ghanizadeh A, Hedayati A: Augmentation of fluoxetine with lovastatin for treating major depressive disorder, a randomized double-blind placebo controlled-clinical trial. Depress Anxiety 2013; 30:1084–1088
18.
Pedersen CB, Gøtzsche H, Møller JO, et al: The Danish Civil Registration System: a cohort of eight million persons. Dan Med Bull 2006; 53:441–449
19.
Kildemoes HW, Sørensen HT, Hallas J: The Danish National Prescription Registry. Scand J Public Health 2011; 39(suppl):38–41
20.
Gardarsdottir H, Heerdink ER, Egberts AC: Potential bias in pharmacoepidemiological studies due to the length of the drug free period: a study on antidepressant drug use in adults in the Netherlands. Pharmacoepidemiol Drug Saf 2006; 15:338–343
21.
Munk-Jørgensen P, Østergaard SD: Register-based studies of mental disorders. Scand J Public Health 2011; 39(suppl):170–174
22.
Mors O, Perto GP, Mortensen PB: The Danish Psychiatric Central Research Register. Scand J Public Health 2011; 39(suppl):54–57
23.
Köhler O, Petersen L, Mors O, et al: Inflammation and depression: combined use of selective serotonin reuptake inhibitors and NSAIDs or paracetamol and psychiatric outcomes. Brain Behav 2015; 5:e00338
24.
Helweg-Larsen K: The Danish Register of Causes of Death. Scand J Public Health 2011; 39(suppl):26–29
25.
Lynge E, Sandegaard JL, Rebolj M: The Danish National Patient Register. Scand J Public Health 2011; 39(suppl):30–33
26.
Mortensen PB, Agerbo E, Erikson T, et al: Psychiatric illness and risk factors for suicide in Denmark. Lancet 2000; 355:9–12
27.
Jensen VM, Rasmussen AW: Danish education registers. Scand J Public Health 2011; 39(suppl):91–94
28.
Charlson ME, Pompei P, Ales KL, et al: A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40:373–383
29.
Nuttall M, van der Meulen J, Emberton M: Charlson scores based on ICD-10 administrative data were valid in assessing comorbidity in patients undergoing urological cancer surgery. J Clin Epidemiol 2006; 59:265–273
30.
Fine JP, Gray RJ: A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 1999; 94:496–509
31.
Antons KA, Williams CD, Baker SK, et al: Clinical perspectives of statin-induced rhabdomyolysis. Am J Med 2006; 119:400–409
32.
Andrade C: Selective serotonin reuptake inhibitor drug interactions in patients receiving statins. J Clin Psychiatry 2014; 75:e95–e99
33.
Bellosta S, Corsini A: Statin drug interactions and related adverse reactions. Expert Opin Drug Saf 2012; 11:933–946
34.
De Berardis D, Marini S, Piersanti M, et al: The relationships between cholesterol and suicide: an update. ISRN Psychiatry 2012; vol 2012, article ID 387901
35.
Bock C, Bukh JD, Vinberg M, et al: Validity of the diagnosis of a single depressive episode in a case register. Clin Pract Epidemol Ment Health 2009; 5:4
36.
Uggerby P, Østergaard SD, Røge R, et al: The validity of the schizophrenia diagnosis in the Danish Psychiatric Central Research Register is good. Dan Med J 2013; 60:A4578
Information & Authors
Information
Published In
History
Received: 13 April 2015
Revision received: 27 January 2016
Revision received: 4 March 2016
Accepted: 21 March 2016
Published online: 3 May 2016
Published in print: August 01, 2016
Authors
Competing Interests
Dr. Gasse has received unrestricted research grants from Eli Lilly and Lundbeck, funding through research collaboration with LASER Analytica, funding from the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement 279227, and support from the Innovative Medicines Initiative Joint Undertaking resources, which were composed of financial contributions from the European Union Seventh Framework Programme and in-kind contributions from members of the European Federation of Pharmaceutical Industries and Associations. Dr. Nierenberg has served as a consultant for Abbott Laboratories, the American Psychiatric Association, Appliance Computing, Inc. (Mindsite), Basilea, Brain Cells, Brandeis University, Bristol-Myers Squibb, Clintara, Corcept, Dey Pharmaceuticals, Dainippon Sumitomo (now Sunovion), Eli Lilly, EpiQ, L.P./Mylan, Forest, Genaissance, Genentech, GlaxoSmithKline, Healthcare Global Village, Hoffman–LaRoche, Infomedic, Lundbeck, Janssen, Jazz Pharmaceuticals, MedAvante, Merck, Methylation Sciences, Naurex, Novartis, Pamlab, Parexel, Pfizer, PGx Health, Otsuka, Ridge Diagnostics, Shire, Schering-Plough, Somerset, Sunovion, Takeda, Targacept, and Teva; he has also served as a consultant through the MGH Clinical Trials Network and Institute for AstraZeneca, Brain Cells, Dainippon Sumitomo/Sepracor, Johnson & Johnson, Labopharm, Merck, Methylation Sciences, Novartis, PGx Health, Shire, Schering-Plough, Targacept, and Takeda/Lundbeck; he has received grants or research support from the American Foundation for Suicide Prevention, the Agency for Healthcare Research and Quality, the Brain and Behavior Research Foundation, Bristol-Myers Squibb, Cederroth, Cephalon, Cyberonics, Elan, Eli Lilly, Forest, GlaxoSmithKline, Janssen, Lichtwer Pharma, the Marriott Foundation, Mylan, NIMH, Pamlab, the Patient-Centered Outcomes Research Institute, Pfizer, Shire, the Stanley Foundation, Takeda, and Wyeth-Ayerst; he has received honoraria from Belvoir Publishing, University of Texas Southwestern Dallas, Brandeis University, Bristol-Myers Squibb, Hillside Hospital, American Drug Utilization Review, the American Society for Clinical Psychopharmacology, Baystate Medical Center, Columbia University, CRICO, Dartmouth Medical School, Health New England, the Harold Grinspoon Charitable Foundation, IMEDEX, the International Society for Bipolar Disorder, the Israel Society for Biological Psychiatry, Johns Hopkins University, MJ Consulting, New York State, Medscape, MBL Publishing, MGH Psychiatry Academy, the National Association of Continuing Education, Physicians Postgraduate Press, SUNY Buffalo, University of Pisa, University of Michigan, University of Miami, University of Wisconsin at Madison, the American Professional Society of ADHD and Related Disorders, the International Society for Bipolar Disorders, SciMed, Slack Publishing, Wolters Kluwer Publishing, the American Society of Clinical Psychopharmacology, the New Clinical Drug Evaluation Unit, Rush Medical College, Yale University School of Medicine, the National Network of Depression Centers, Nova Southeastern University, NAMI, the Institute of Medicine, CME Institute, the International Society for CNS Clinical Trials and Methodology, the World Congress on Brain Behavior and Emotion, the Congress of the Hellenic Society for Basic and Clinical Pharmacology, and the Anxiety and Depression Association of America; he owns stock in Appliance Computing, Inc. (MindSite), Brain Cells, and MedAvante; and he holds copyrights for the Clinical Positive Affect Scale and the MGH Structured Clinical Interview for the Montgomery-Åsberg Depression Rating Scale, exclusively licensed to the MGH Clinical Trials Network and Institute. The other authors report no financial relationships with commercial interests.
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBFigures
FIGURE 1. Flowchart Illustrating the Design of a Study of the Effect of Concomitant Treatment With SSRIs and Statinsa
a Source: Statistics Denmark. SSRIs=selective serotonin reuptake inhibitors.
FIGURE 2. Cumulative Psychiatric Hospital Contacts for Any Reason or Due to Depression Specifically Among Individuals Using an SSRI and a Statin Concomitantly, Compared With Individuals Using an SSRI Alonea
a Adjusted for age, sex, education level, SSRI index year, previous contacts for mental disorders and medical diseases, and use of other anti-inflammatory medications, cardiovascular protective medications, and psychopharmaceuticals during the year preceding the SSRI index date. SSRI=selective serotonin reuptake inhibitor.
Tables
Media
References
References
1.
Trivedi MH, Rush AJ, Wisniewski SR, et al: Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry 2006; 163:28–40
2.
Gaynes BN, Warden D, Trivedi MH, et al: What did STAR*D teach us? Results from a large-scale, practical, clinical trial for patients with depression. Psychiatr Serv 2009; 60:1439–1445
3.
Nierenberg AA: Strategies for achieving full remission when first-line antidepressants are not enough. J Clin Psychiatry 2013; 74:e26
4.
Müller N: Immunology of major depression. Neuroimmunomodulation 2014; 21:123–130
5.
Benros ME, Waltoft BL, Nordentoft M, et al: Autoimmune diseases and severe infections as risk factors for mood disorders: a nationwide study. JAMA Psychiatry 2013; 70:812–820
6.
Wium-Andersen MK, Ørsted DD, Nielsen SF, et al: Elevated C-reactive protein levels, psychological distress, and depression in 73,131 individuals. JAMA Psychiatry 2013; 70:176–184
7.
Abbasi SH, Hosseini F, Modabbernia A, et al: Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: randomized double-blind placebo-controlled study. J Affect Disord 2012; 141:308–314
8.
Almeida OP, Flicker L, Yeap BB, et al: Aspirin decreases the risk of depression in older men with high plasma homocysteine. Transl Psychiatry 2012; 2:e151
9.
Köhler O, Benros ME, Nordentoft M, et al: Effect of anti-inflammatory treatment on depression, depressive symptoms, and adverse effects: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry 2014; 71:1381–1391
10.
Weitz-Schmidt G: Statins as anti-inflammatory agents. Trends Pharmacol Sci 2002; 23:482–486
11.
Zhang X, Norris SL, Gregg EW, et al: Depressive symptoms and mortality among persons with and without diabetes. Am J Epidemiol 2005; 161:652–660
12.
Mansi I, Frei CR, Pugh MJ, et al: Psychologic disorders and statin use: a propensity score-matched analysis. Pharmacotherapy 2013; 33:615–626
13.
Parsaik AK, Singh B, Hassan Murad M, et al: Statins use and risk of depression: a systematic review and meta-analysis. J Affect Disord 2014; 160:62–67
14.
Otte C, Zhao S, Whooley MA: Statin use and risk of depression in patients with coronary heart disease: longitudinal data from the Heart and Soul Study. J Clin Psychiatry 2012; 73:610–615
15.
Young-Xu Y, Chan KA, Liao JK, et al: Long-term statin use and psychological well-being. J Am Coll Cardiol 2003; 42:690–697
16.
Santos T, Baungratz MM, Haskel SP, et al: Behavioral interactions of simvastatin and fluoxetine in tests of anxiety and depression. Neuropsychiatr Dis Treat 2012; 8:413–422
17.
Ghanizadeh A, Hedayati A: Augmentation of fluoxetine with lovastatin for treating major depressive disorder, a randomized double-blind placebo controlled-clinical trial. Depress Anxiety 2013; 30:1084–1088
18.
Pedersen CB, Gøtzsche H, Møller JO, et al: The Danish Civil Registration System: a cohort of eight million persons. Dan Med Bull 2006; 53:441–449
19.
Kildemoes HW, Sørensen HT, Hallas J: The Danish National Prescription Registry. Scand J Public Health 2011; 39(suppl):38–41
20.
Gardarsdottir H, Heerdink ER, Egberts AC: Potential bias in pharmacoepidemiological studies due to the length of the drug free period: a study on antidepressant drug use in adults in the Netherlands. Pharmacoepidemiol Drug Saf 2006; 15:338–343
21.
Munk-Jørgensen P, Østergaard SD: Register-based studies of mental disorders. Scand J Public Health 2011; 39(suppl):170–174
22.
Mors O, Perto GP, Mortensen PB: The Danish Psychiatric Central Research Register. Scand J Public Health 2011; 39(suppl):54–57
23.
Köhler O, Petersen L, Mors O, et al: Inflammation and depression: combined use of selective serotonin reuptake inhibitors and NSAIDs or paracetamol and psychiatric outcomes. Brain Behav 2015; 5:e00338
24.
Helweg-Larsen K: The Danish Register of Causes of Death. Scand J Public Health 2011; 39(suppl):26–29
25.
Lynge E, Sandegaard JL, Rebolj M: The Danish National Patient Register. Scand J Public Health 2011; 39(suppl):30–33
26.
Mortensen PB, Agerbo E, Erikson T, et al: Psychiatric illness and risk factors for suicide in Denmark. Lancet 2000; 355:9–12
27.
Jensen VM, Rasmussen AW: Danish education registers. Scand J Public Health 2011; 39(suppl):91–94
28.
Charlson ME, Pompei P, Ales KL, et al: A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40:373–383
29.
Nuttall M, van der Meulen J, Emberton M: Charlson scores based on ICD-10 administrative data were valid in assessing comorbidity in patients undergoing urological cancer surgery. J Clin Epidemiol 2006; 59:265–273
30.
Fine JP, Gray RJ: A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 1999; 94:496–509
31.
Antons KA, Williams CD, Baker SK, et al: Clinical perspectives of statin-induced rhabdomyolysis. Am J Med 2006; 119:400–409
32.
Andrade C: Selective serotonin reuptake inhibitor drug interactions in patients receiving statins. J Clin Psychiatry 2014; 75:e95–e99
33.
Bellosta S, Corsini A: Statin drug interactions and related adverse reactions. Expert Opin Drug Saf 2012; 11:933–946
34.
De Berardis D, Marini S, Piersanti M, et al: The relationships between cholesterol and suicide: an update. ISRN Psychiatry 2012; vol 2012, article ID 387901
35.
Bock C, Bukh JD, Vinberg M, et al: Validity of the diagnosis of a single depressive episode in a case register. Clin Pract Epidemol Ment Health 2009; 5:4
36.
Uggerby P, Østergaard SD, Røge R, et al: The validity of the schizophrenia diagnosis in the Danish Psychiatric Central Research Register is good. Dan Med J 2013; 60:A4578