The Bidirectional Associations Between Psychotic Experiences and DSM-IV Mental Disorders
Abstract
Objective:
Method:
Results:
Conclusions:
Method
Samples
Procedures
Data Collection and Data Items
Psychotic experiences.
DSM-IV mental disorders.
Statistical Analysis
Results
Lifetime Prevalence of Mental Disorders Among Respondents With and Without Psychotic Experiences
| Total Sample (N=31,261) | Respondents With Lifetime Psychotic Experiences (N=2,385) | Respondents Without Lifetime Psychotic Experiences (N=28,876) | Odds Ratio Between Lifetime Psychotic Experiences and Lifetime Mental Disorder | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mental Disorder | Na | %b | SE | Na | %b | SE | Na | %b | SE | Odds Ratioc | 95% CI |
| Mood disorders | |||||||||||
| Major depressive disorder with hierarchy | 6,824 | 11.8 | 0.2 | 897 | 25.4 | 1.2 | 5,927 | 10.9 | 0.2 | 2.3* | 2.0–2.6 |
| Bipolar disorder (broad) | 1,212 | 2.3 | 0.1 | 196 | 6.5 | 0.6 | 1,016 | 2.1 | 0.1 | 2.8* | 2.2–3.5 |
| Anxiety disorders | |||||||||||
| Panic disorder | 1,019 | 1.8 | 0.1 | 181 | 4.8 | 0.5 | 838 | 1.6 | 0.1 | 2.7* | 2.2–3.4 |
| Generalized anxiety disorder with hierarchy | 1,832 | 3.4 | 0.1 | 276 | 8.0 | 0.6 | 1,556 | 3.1 | 0.1 | 2.4* | 2.0–3.0 |
| Social phobia | 2,495 | 4.7 | 0.1 | 382 | 12.1 | 0.8 | 2,113 | 4.3 | 0.1 | 2.4* | 2.0–2.8 |
| Specific phobia | 4,108 | 8.4 | 0.2 | 630 | 20.5 | 1.1 | 3,478 | 7.6 | 0.2 | 2.6* | 2.3–3.0 |
| Agoraphobia without panic | 557 | 1.0 | 0.1 | 102 | 3.1 | 0.4 | 455 | 0.9 | 0.1 | 2.8* | 2.0–3.9 |
| Posttraumatic stress disorder | 1,811 | 3.7 | 0.1 | 328 | 10.2 | 0.7 | 1,483 | 3.3 | 0.1 | 3.0* | 2.5–3.6 |
| Separation anxiety disorder (child) | 449 | 2.2 | 0.1 | 90 | 5.7 | 0.8 | 359 | 2.0 | 0.1 | 2.3* | 1.6–3.1 |
| Separation anxiety disorder (adult) | 877 | 3.7 | 0.2 | 186 | 11.1 | 1.0 | 691 | 3.2 | 0.2 | 3.1* | 2.4–4.0 |
| Impulse control disorders | |||||||||||
| Intermittent explosive disorder with hierarchy | 1,023 | 3.3 | 0.1 | 153 | 8.4 | 0.7 | 870 | 3.0 | 0.1 | 2.1* | 1.7–2.6 |
| Attention deficit hyperactivity disorder | 368 | 1.5 | 0.1 | 79 | 5.1 | 0.8 | 289 | 1.3 | 0.1 | 2.6* | 1.8–3.9 |
| Oppositional defiant disorder with hierarchy | 311 | 2.2 | 0.2 | 68 | 5.8 | 0.9 | 243 | 1.9 | 0.2 | 2.7* | 1.8–4.1 |
| Conduct disorder | 329 | 2.1 | 0.2 | 64 | 5.4 | 0.8 | 265 | 1.8 | 0.2 | 2.3* | 1.6–3.4 |
| Eating disorders | |||||||||||
| Anorexia nervosa | 69 | 0.4 | 0.1 | 13 | 0.7 | 0.3 | 56 | 0.3 | 0.1 | 1.8 | 0.7–4.4 |
| Binge eating disorder with hierarchy | 563 | 2.1 | 0.1 | 128 | 5.0 | 0.5 | 435 | 1.9 | 0.1 | 2.0* | 1.5–2.6 |
| Bulimia nervosa with hierarchy | 364 | 1.1 | 0.1 | 89 | 3.8 | 0.5 | 275 | 0.9 | 0.1 | 3.6* | 2.6–5.0 |
| Substance use disorders | |||||||||||
| Alcohol abuse with hierarchy | 1,908 | 5.1 | 0.2 | 232 | 9.8 | 0.9 | 1,676 | 4.8 | 0.2 | 1.7* | 1.4–2.0 |
| Alcohol dependence | 1,170 | 2.4 | 0.1 | 205 | 6.3 | 0.6 | 965 | 2.1 | 0.1 | 2.3* | 1.8–2.8 |
| Drug abuse with hierarchy | 644 | 1.8 | 0.1 | 83 | 3.6 | 0.5 | 561 | 1.7 | 0.1 | 1.6* | 1.2–2.1 |
| Drug dependence | 481 | 1.2 | 0.1 | 104 | 3.8 | 0.5 | 377 | 1.0 | 0.1 | 2.7* | 1.9–3.6 |
Temporal Priorities Between Onset Ages for Psychotic Experiences and Mental Disorders
| Mental Disorder | Respondents With Psychotic Experience and Mental Disorder | Respondents With Both Lifetime Mental Disorder of Interest and Lifetime Psychotic Experiences | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Psychotic Experience Onset Prior to Disorder Onset | Psychotic Experience Onset and Disorder Onset in the Same Year | Psychotic Experience Onset After Disorder Onset | Goodness-of-Fit Test for Equal Proportiona | ||||||
| N | %b | SE | %b | SE | %b | SE | χ2 | p | |
| Mood disorders | |||||||||
| Major depressive disorder with hierarchy | 897 | 44.5 | 2.0 | 10.2 | 1.2 | 45.4 | 2.2 | 0.1 | 0.767 |
| Bipolar disorder (broad) | 196 | 53.7 | 5.0 | 7.2 | 2.5 | 39.1 | 5.0 | 6.0 | 0.024 |
| Anxiety disorders | |||||||||
| Panic disorder | 181 | 42.2 | 5.3 | 10.9 | 3.9 | 46.9 | 5.3 | 1.0 | 0.343 |
| Generalized anxiety disorder with hierarchy | 276 | 46.1 | 4.2 | 6.8 | 1.9 | 47.1 | 4.3 | 0.0 | 0.839 |
| Social phobia | 382 | 22.6 | 2.8 | 6.7 | 2.2 | 70.7 | 3.3 | 113.0 | <0.001 |
| Specific phobia | 630 | 6.7 | 1.2 | 4.5 | 0.9 | 88.9 | 1.5 | 549.8 | <0.001 |
| Agoraphobia without panic | 102 | 28.4 | 5.8 | 3.7 | 1.9 | 68.0 | 5.9 | 38.2 | <0.001 |
| Posttraumatic stress disorder | 328 | 40.0 | 3.9 | 11.2 | 2.3 | 48.8 | 3.6 | 4.2 | 0.047 |
| Separation anxiety disorder (child) | 90 | 9.1 | 2.8 | 3.8 | 2.0 | 87.1 | 3.4 | 163.5 | <0.001 |
| Separation anxiety disorder (adult) | 186 | 46.7 | 5.0 | 7.5 | 1.9 | 45.8 | 5.0 | 0.0 | 0.893 |
| Impulse control disorders | |||||||||
| Intermittent explosive disorder with hierarchy | 153 | 25.4 | 3.3 | 5.3 | 2.3 | 69.4 | 3.9 | 105.0 | <0.001 |
| Attention deficit hyperactivity disorder | 79 | 9.4 | 4.9 | 2.9 | 2.7 | 87.6 | 6.1 | 3,145.0 | <0.001 |
| Oppositional defiant disorder with hierarchy | 68 | 17.6 | 5.8 | 1.1 | 1.1 | 81.3 | 5.9 | 401.3 | <0.001 |
| Conduct disorder | 64 | 17.7 | 5.9 | 4.9 | 3.4 | 77.5 | 7.2 | 54.0 | <0.001 |
| Eating disorders | |||||||||
| Anorexia nervosa | 13 | 23.6 | 13.6 | — | — | 76.4 | 13.6 | —c | — |
| Binge eating disorder with hierarchy | 128 | 44.7 | 5.9 | 6.9 | 2.9 | 48.3 | 5.9 | 0.2 | 0.656 |
| Bulimia nervosa with hierarchy | 89 | 49.8 | 6.3 | 8.4 | 4.0 | 41.8 | 6.4 | 1.4 | 0.266 |
| Substance use disorders | |||||||||
| Alcohol abuse with hierarchy | 232 | 50.1 | 4.6 | 2.6 | 1.2 | 47.3 | 4.6 | 0.5 | 0.494 |
| Alcohol dependence | 205 | 43.3 | 4.4 | 6.3 | 2.6 | 50.4 | 4.8 | 2.8 | 0.109 |
| Drug abuse with hierarchy | 83 | 55.0 | 6.9 | 3.2 | 2.0 | 41.8 | 6.8 | 36.6 | 0.026 |
| Drug dependence | 104 | 48.2 | 6.3 | 7.6 | 3.8 | 44.2 | 6.2 | 2.5 | 0.192 |
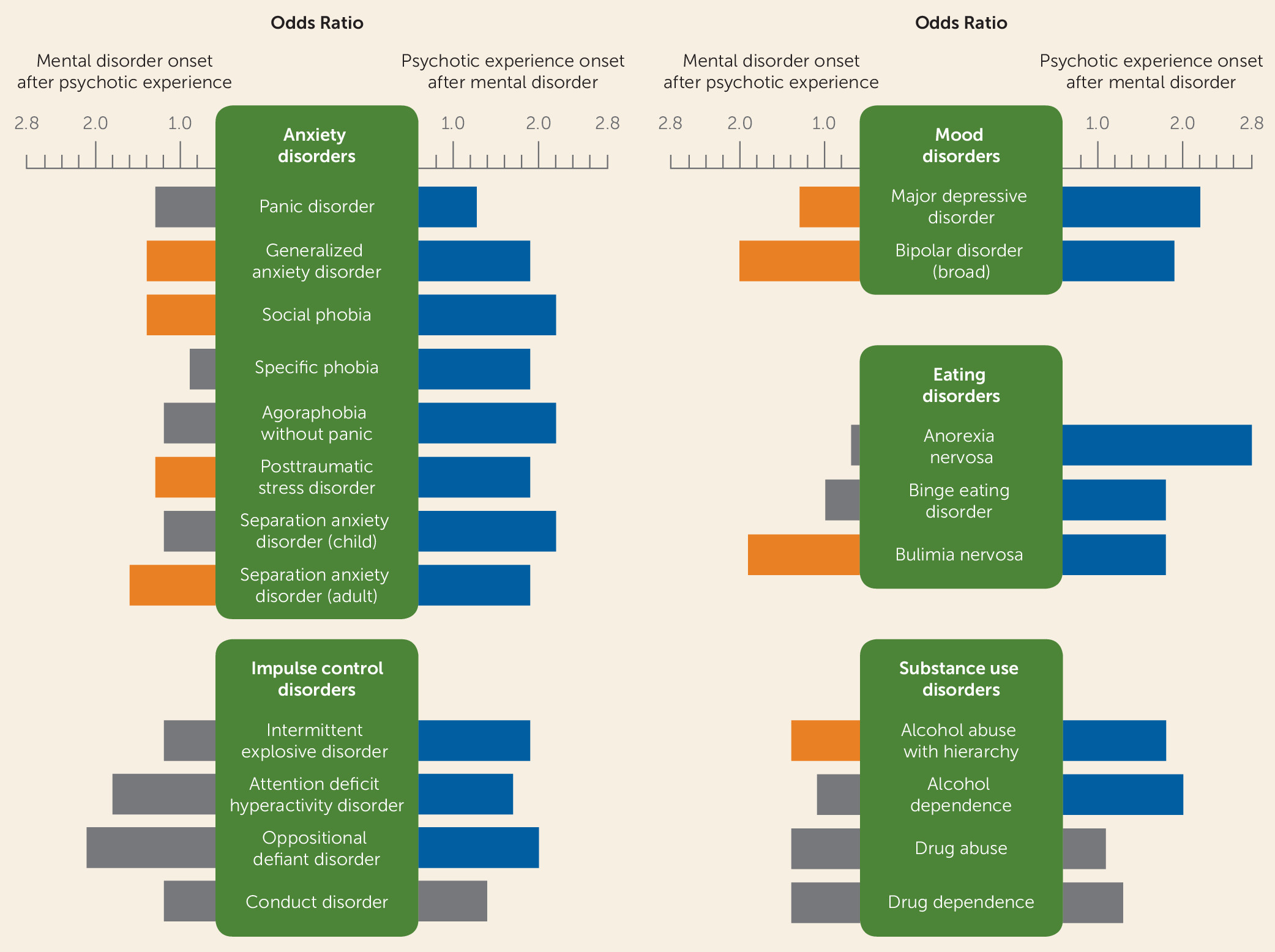
Time-Lagged Associations Between Lifetime Psychotic Experiences and Subsequent Onset of Mental Disorders
| Bivariate Modelsa | Multivariate Modelsb | |||
|---|---|---|---|---|
| Mental Disorder | Odds Ratio | 95% CI | Odds Ratio | 95% CI |
| Mood disorders | ||||
| Major depressive disorder with hierarchy | 1.6* | 1.4–1.9 | 1.3* | 1.2–1.5 |
| Bipolar disorder (broad) | 2.7* | 2.0–3.5 | 2.0* | 1.5–2.6 |
| Anxiety disorders | ||||
| Panic disorder | 2.0* | 1.5–2.8 | 1.3 | 0.9–1.8 |
| Generalized anxiety disorder with hierarchy | 1.9* | 1.5–2.4 | 1.4* | 1.1–1.8 |
| Social phobia | 2.0* | 1.5–2.7 | 1.4* | 1.0–1.8 |
| Specific phobia | 1.0 | 0.7–1.5 | 0.9 | 0.6–1.3 |
| Agoraphobia without panic | 2.0* | 1.2–3.4 | 1.2 | 0.7–2.1 |
| Posttraumatic stress disorder | 2.0* | 1.6–2.6 | 1.3* | 1.1–1.7 |
| Separation anxiety disorder (child) | 1.7 | 0.9–3.2 | 1.2 | 0.6–2.3 |
| Separation anxiety disorder (adult) | 2.7* | 1.9–3.6 | 1.6* | 1.2–2.2 |
| Impulse control disorders | ||||
| Intermittent explosive disorder with hierarchy | 1.5* | 1.1–2.1 | 1.2 | 0.9–1.6 |
| Attention deficit hyperactivity disorder | 2.5 | 0.8–7.4 | 1.8 | 0.6–5.6 |
| Oppositional defiant disorder with hierarchy | 2.6* | 1.2–5.7 | 2.1 | 0.9–5.0 |
| Conduct disorder | 1.9 | 0.9–4.1 | 1.2 | 0.5–3.0 |
| Eating disorders | ||||
| Anorexia nervosa | 0.9 | 0.3–2.8 | 0.7 | 0.2–2.0 |
| Binge eating disorder with hierarchy | 1.7* | 1.1–2.5 | 1.0 | 0.7–1.6 |
| Bulimia nervosa with hierarchy | 3.2* | 2.2–4.8 | 1.9* | 1.2–3.1 |
| Substance use disorders | ||||
| Alcohol abuse with hierarchy | 1.7* | 1.3–2.3 | 1.4* | 1.1–1.9 |
| Alcohol dependence | 1.9* | 1.4–2.7 | 1.1 | 0.8–1.7 |
| Drug abuse with hierarchy | 1.9* | 1.2–2.8 | 1.4 | 0.9–2.1 |
| Drug dependence | 2.3* | 1.5–3.4 | 1.4 | 0.9–2.0 |
Time-Lagged Associations Between Lifetime Mental Disorders and Subsequent Onset of Psychotic Experiences
| Mental Disorder | Bivariate Modelsa | Multivariate Modelb | ||
|---|---|---|---|---|
| Odds Ratio | 95% CI | Odds Ratio | 95% CI | |
| Mood disorders | ||||
| Major depressive disorder with hierarchy | 2.5* | 2.1–3.0 | 2.2* | 1.8–2.7 |
| Bipolar disorder (broad) | 2.6* | 1.9–3.7 | 1.9* | 1.3–2.9 |
| Anxiety disorders | ||||
| Panic disorder | 2.5* | 1.8–3.4 | 1.6* | 1.2–2.3 |
| Generalized anxiety disorder with hierarchy | 2.4* | 1.8–3.1 | 1.7* | 1.2–2.3 |
| Social phobia | 2.2* | 1.8–2.6 | 1.5* | 1.2–2.0 |
| Specific phobia | 2.6* | 2.2–2.9 | 2.2* | 1.8–2.7 |
| Agoraphobia without panic | 2.5* | 1.8–3.6 | 1.9* | 1.3–2.7 |
| Posttraumatic stress disorder | 2.5* | 1.9–3.2 | 1.8* | 1.3–2.4 |
| Separation anxiety disorder (child) | 2.1* | 1.5–3.0 | 1.5* | 1.0–2.1 |
| Separation anxiety disorder (adult) | 2.8* | 2.1–3.9 | 1.9* | 1.3–2.8 |
| Impulse control disorders | ||||
| Intermittent explosive disorder with hierarchy | 2.4* | 1.9–3.0 | 1.9* | 1.5–2.5 |
| Attention deficit hyperactivity disorder | 2.7* | 2.0–3.8 | 1.7* | 1.2–2.4 |
| Oppositional defiant disorder with hierarchy | 3.0* | 2.1–4.3 | 2.0* | 1.3–3.1 |
| Conduct disorder | 2.5* | 1.7–3.7 | 1.4 | 0.9–2.3 |
| Eating disorders | ||||
| Anorexia nervosa | 2.9* | 1.1–8.1 | 2.8* | 1.0–7.8 |
| Binge eating disorder with hierarchy | 2.2* | 1.6–3.2 | 1.8* | 1.2–2.6 |
| Bulimia nervosa with hierarchy | 2.7* | 1.8–4.2 | 1.8* | 1.2–3.0 |
| Substance use disorders | ||||
| Alcohol abuse with hierarchy | 1.8* | 1.4–2.5 | 1.8* | 1.3–2.5 |
| Alcohol dependence | 2.4* | 1.8–3.3 | 2.0* | 1.3–2.9 |
| Drug abuse with hierarchy | 1.5 | 1.0–2.3 | 1.1 | 0.7–1.8 |
| Drug dependence | 2.6* | 1.7–3.9 | 1.3 | 0.8–2.3 |
| χ2 | p | |||
| Joint effect of all types of disorders (df=21) | 130.4 | <0.001 | ||
| Difference between types of disorders (df=20) | 27.9 | 0.111 | ||
| Odds Ratio | 95% CI | |||
| Number of disorders | ||||
| 2 disorders | 1.0 | 0.7–1.3 | ||
| 3 disorders | 0.5* | 0.4–0.8 | ||
| 4 disorders | 0.4* | 0.2–0.8 | ||
| 5+ disorders | 0.2* | 0.1–0.4 | ||
| χ2 | p | |||
| Joint effect of all number of disorders (df=4) | 31.1 | <0.001 | ||
Discussion
Future Directions
Conclusions
Acknowledgments
Footnotes
Supplementary Material
- View/Download
- 677.01 KB
References
Information & Authors
Information
Published In
History
Authors
Competing Interests
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).