Changes in Prevalence of Depression and Anxiety Following Smoking Cessation: Results From an International Cohort Study (ATTEMPT)
Abstract
Background:
Method:
Results:
Conclusions:
Introduction
Methods
Study Population and Design
| Smoking status at 12-month follow-up | ||||||
|---|---|---|---|---|---|---|
| Total sample (n = 3645) | Lost to follow-up (n = 2005) | Followed up (n = 1640) | Ex-smoker ≥ 3 months (n = 123) | Ex-smoker <3 months (n = 159) | Current smoker (n = 1358) | |
| Sociodemographic characteristics | ||||||
| Mean age, years (s.d.) | 45.8 (7.3) | 45.4 (7.1) | 46.3 (7.5)*** | 47.1 (7.9) | 46.7 (7.8) | 46.2 (7.4) |
| Women, % (n) | 48.0 (1750) | 50.3 (1009) | 45.2 (741)** | 45.5 (56) | 40.9 (65) | 45.7 (620) |
| Married, % (n) | 47.4 (1729) | 44.4 (890) | 51.2 (839)*** | 50.4 (62) | 47.8 (76) | 51.6 (701) |
| Employed, % (n)a | 72.2 (2632) | 71.4 (1427) | 73.6 (1205) | 77.2 (95) | 76.6 (121) | 72.9 (989) |
| White, % (n) | 93.3 (3400) | 93.7 (1879) | 92.7 (1521) | 95.1 (117) | 95.0 (151) | 92.3 (1253) |
| Education, % (n)b | ||||||
| No high school | 4.5 (163) | 5.5 (109) | 3.3 (54)* | 4.9 (6) | 4.4 (7) | 3.0 (41) |
| Some high school | 5.9 (215) | 6.5 (129) | 5.3 (86) | 1.6 (2) | 5.0 (8) | 5.6 (76) |
| High school | 31.6 (1150) | 33.6 (672) | 29.2 (478)* | 30.1 (37) | 28.3 (45) | 29.2 (396) |
| Some college | 27.8 (1014) | 25.7 (514) | 30.5 (500)** | 30.1 (37) | 28.9 (46) | 30.8 (417) |
| College | 8.9 (324) | 8.8 (176) | 9.0 (148) | 11.4 (14) | 10.7 (17) | 8.6 (117) |
| Graduate school | 21.2 (771) | 20.0 (399) | 22.7 (372) | 22.0 (27) | 22.6 (36) | 22.8 (309) |
| Country, % (n) | ||||||
| USA | 19.9 (725) | 14.4 (288) | 26.6 (437)*** | 22.8 (28) | 21.4 (34) | 27.6 (375) |
| Canada | 2.8 (102) | 2.2 (45) | 3.5 (57) | 4.1 (5) | 2.5 (4) | 3.5 (48) |
| UK | 33.0 (1203) | 38.3 (767) | 26.6 (436)*** | 38.2 (47) | 30.8 (49) | 25.0 (340) |
| France | 33.2 (1209) | 35.0 (702) | 30.9 (507)* | 22.8 (28) | 34.0 (54) | 31.3 (425) |
| Spain | 11.1 (406) | 10.1 (203) | 12.4 (203) | 12.2 (15) | 11.3 (18) | 12.5 (170) |
| Cigarette smoking characteristics | ||||||
| Mean length of time of smoking, years (s.d.) | 28.5 (9.4) | 28.2 (9.3) | 29.0 (9.4)** | 29.8 (9.4) | 29.8 (9.0) | 28.8 (9.5) |
| Mean nicotine dependence score (s.d.)c | 4.7 (2.4) | 4.7 (2.4) | 4.7 (2.4) | 4.4 (2.6)x,y | 3.9 (2.5)x | 4.8 (2.4)y |
| Mean motivation to quit (s.d.) | 6.8 (1.9) | 6.8 (1.9) | 6.9 (1.8) | 7.0 (1.7) | 7.1 (1.8) | 6.9 (1.9) |
| Quit attempt in past 3 months, % (n)d | 29.1 (983) | 30.9 (572) | 27.0 (411)* | 20.5 (23)x | 40.1 (61)y | 26.0 (327)x |
| Use of cessation medication in past 3 months, % (n) | 25.7 (937) | 27.9 (559) | 23.0 (378)** | 15.4 (19) | 25.2 (40) | 23.5 (319) |
| Physical and mental health characteristics | ||||||
| Mean body mass index, kg/m2 (s.d.) | 26.8 (5.5) | 26.5 (5.5) | 27.1 (5.4)*** | 27.8 (4.9) | 27.9 (5.6) | 27.0 (5.5) |
| Mean EQ-5D score (s.d.)e | 0.76 (0.26) | 0.75 (0.27) | 0.76 (0.26) | 0.82 (0.22)x | 0.78 (0.23)x,y | 0.76 (0.27)y |
| Lifetime diagnosis, % (n) | ||||||
| Any | 39.5 (1439) | 41.1 (824) | 37.5 (615)* | 35.8 (44) | 39.6 (63) | 37.4 (508) |
| Depressionf | 24.0 (870) | 25.4 (506) | 22.3 (364)* | 16.3 (20) | 20.3 (32) | 23.1 (312) |
| Anxietyf | 28.0 (1016) | 28.5 (569) | 27.4 (447) | 25.2 (31) | 28.5 (45) | 27.5 (371) |
| Prescription in past 2 weeks, % (n) | ||||||
| Any | 15.4 (561) | 15.3 (306) | 15.5 (255) | 9.8 (12) | 15.7 (25) | 16.1 (218) |
| Depression | 10.1 (369) | 10.5 (210) | 9.7 (159) | 4.9 (6) | 9.4 (15) | 10.2 (138) |
| Anxiety | 9.4 (341) | 9.0 (180) | 9.8 (161) | 5.7 (7) | 8.8 (159) | 10.3 (140) |
| Symptom in past 3 months, % (n) | ||||||
| Any | 29.5 (1075) | 30.1 (604) | 28.7 (471) | 26.8 (33) | 30.2 (48) | 28.7 (390) |
| Depressiong | 16.0 (581) | 16.5 (330) | 15.3 (251) | 10.6 (13) | 13.2 (21) | 16.0 (217) |
| Anxietyg | 21.5 (781) | 21.8 (437) | 21.0 (344) | 18.7 (23) | 24.5 (39) | 20.8 (282) |
Measures
Analysis
Results
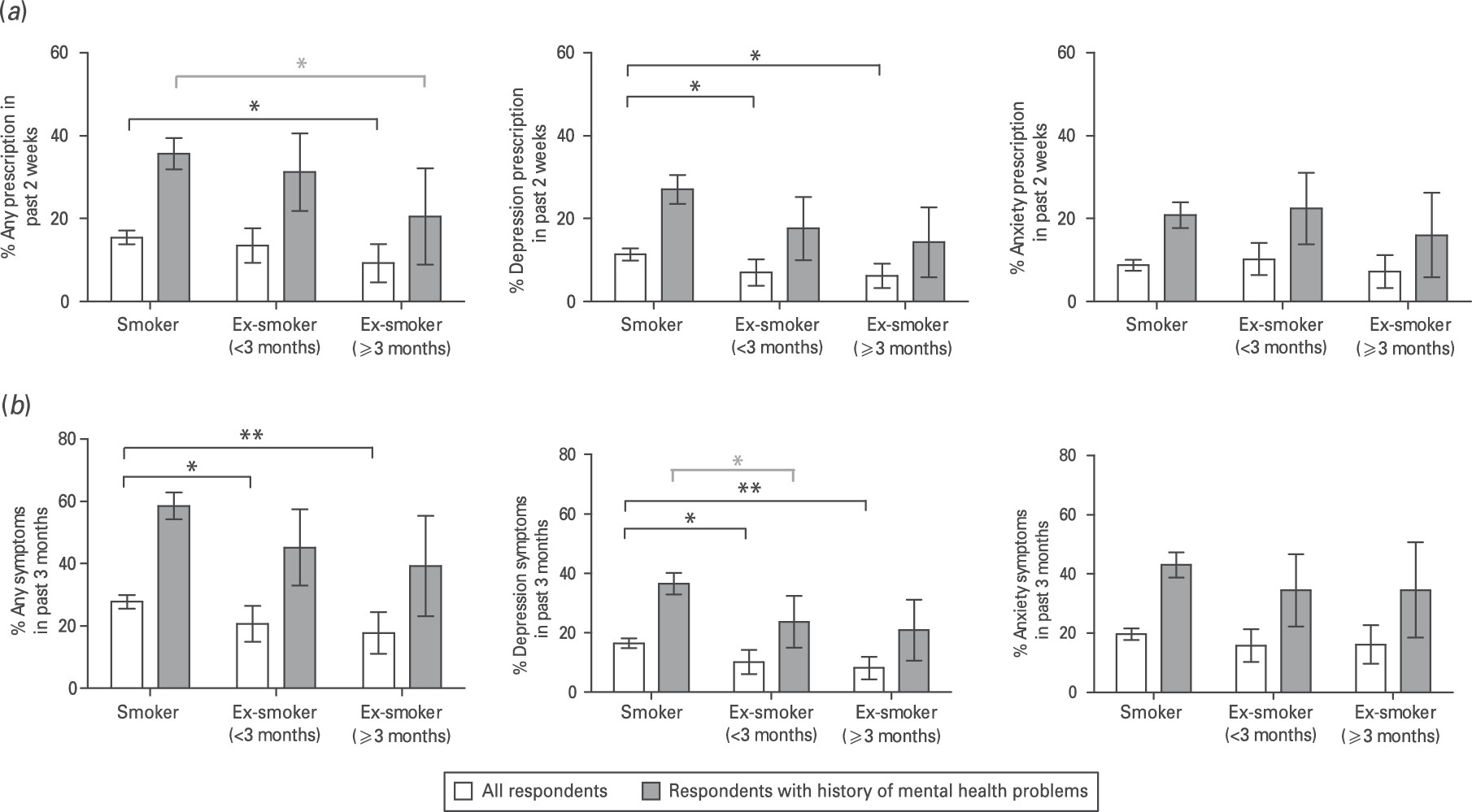
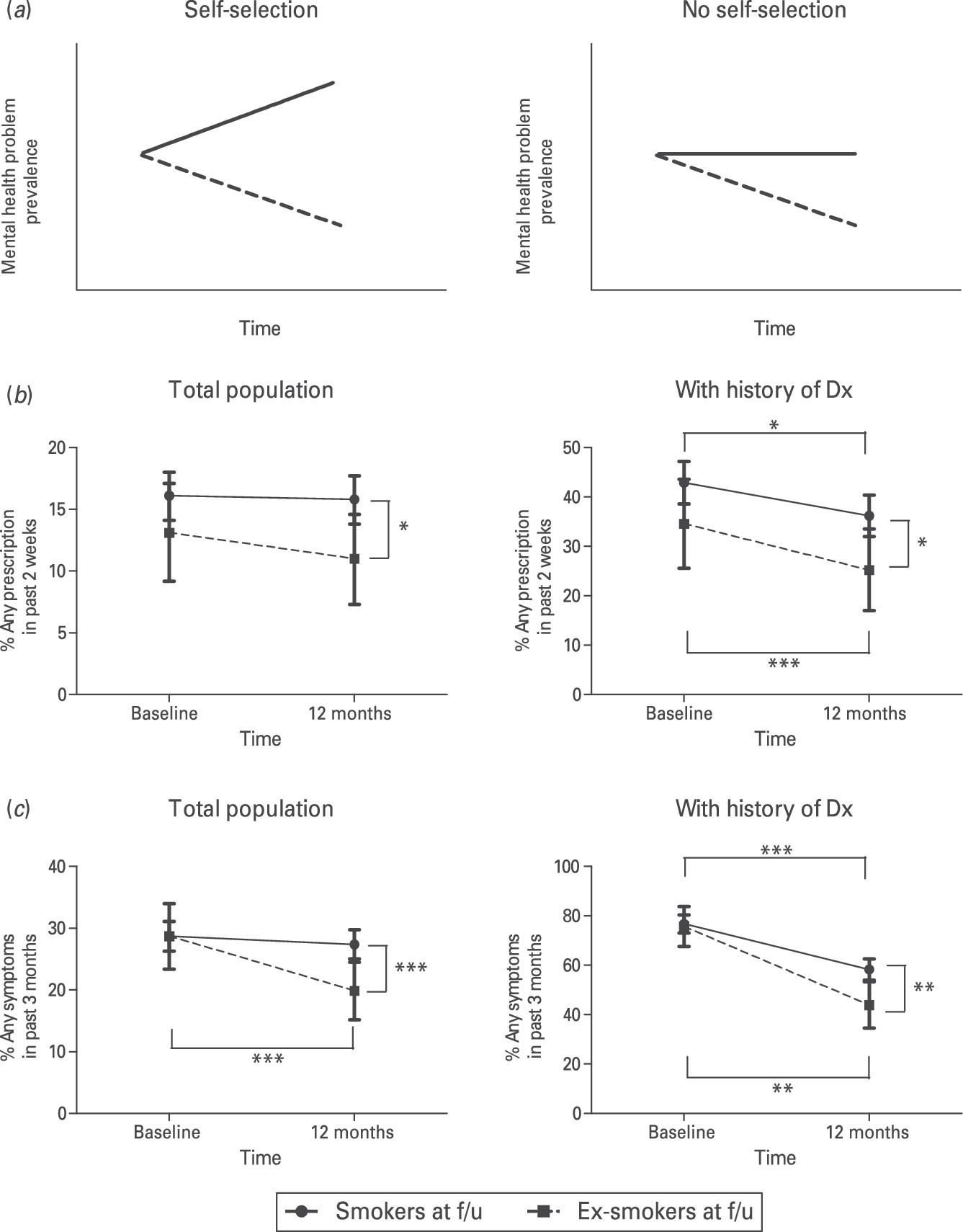
Impact of Short- and Longer-Term Smoking Cessation on Depression and Anxiety Prevalence in the General Population
| Total follow-up | Current smoker (1) | Ex-smoker <3 months (2) | Ex-smoker ≥ 3 months (3) | 2 v. 1: OR (95% CI) | 3 v. 1: OR (95% CI) | |
|---|---|---|---|---|---|---|
| General population | ||||||
| Subjects, n | 1640 | 1358 | 159 | 123 | ||
| Prescription in past 2 weeks, % (n) | ||||||
| Any | 14.9 (245) | 15.8 (214) | 13.8 (22) | 7.3 (9) | 0.86 (0.54–1.38) | 0.42 (0.21–0.85)* |
| Depression | 10.4 (171) | 11.5 (156) | 6.9 (11) | 3.3 (4) | 0.57 (0.30–1.08) | 0.26 (0.09–0.71)** |
| Anxiety | 9.0 (147) | 9.2 (125) | 9.4 (15) | 5.7 (7) | 1.03 (0.59–1.80) | 0.60 (0.27–1.31) |
| Symptom in last 3 months, % (n) | ||||||
| Any | 26.1 (428) | 27.4 (372) | 22.0 (35) | 17.1 (21) | 0.75 (0.51–1.11) | 0.55 (0.34–0.89)* |
| Depressiona | 15.0 (245) | 16.5 (223) | 9.5 (15) | 5.7 (7) | 0.53 (0.31–0.92)* | 0.31 (0.14–0.67)** |
| Anxietya | 19.1 (313) | 19.7 (267) | 17.1 (27) | 15.6 (19) | 0.84 (0.54–1.30) | 0.75 (0.45–1.25) |
| Population with mental health historyb | ||||||
| Subjects, n | 615 | 508 | 63 | 44 | ||
| Prescription in past 2 weeks, % (n) | ||||||
| Any | 34.3 (211) | 36.2 (184) | 31.7 (20) | 15.9 (7) | 0.82 (0.47–1.44) | 0.33 (0.15–0.76)** |
| Depression | 24.9 (153) | 27.2 (138) | 17.5 (11) | 9.1 (4) | 0.57 (0.29–1.12) | 0.27 (0.09–0.76)* |
| Anxiety | 21.1 (130) | 22.0 (112) | 20.6 (13) | 11.4 (5) | 0.92 (0.48–1.75) | 0.45 (0.18–1.18) |
| Symptom in past 3 months, % (n) | ||||||
| Any | 55.8 (343) | 58.3 (296) | 47.6 (30) | 38.6 (17) | 0.65 (0.39–1.10) | 0.45 (0.24–0.85)* |
| Depression | 33.7 (207) | 36.6 (186) | 22.2 (14) | 15.9 (7) | 0.50 (0.27–0.92)* | 0.33 (0.14–0.75)** |
| Anxiety | 42.1 (259) | 43.5 (221) | 36.5 (23) | 34.1 (15) | 0.75 (0.43–1.28) | 0.67 (0.35–1.28) |
| Prescription for condition in past 2 weeks: OR (95% CI) | Symptom in past 3 months: OR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Any (n = 1423) | Depression (n = 1423) | Anxiety (n = 1423) | Any (n = 1423) | Depression (n = 1417) | Anxiety (n = 1417) | |
| Age | 1.03 (1.00–1.05)* | 1.01 (0.99–1.04) | 1.02 (0.98–1.05) | 1.02 (1.00–1.04) | 1.01 (0.99–1.04) | 1.00 (0.98–1.02) |
| Gendera | 1.44 (0.98–2.12) | 1.03 (0.66–1.61) | 2.34 (1.42–3.86)** | 1.72 (1.28–2.33)*** | 1.05 (0.71–1.57) | 1.93 (1.39–2.68)*** |
| Marriage statusb | 0.75 (0.51–1.09) | 0.53 (0.34–0.82)** | 1.06 (0.66–1.72) | 1.02 (0.76–1.37) | 0.54 (0.37–0.80)** | 1.04 (0.76–1.43) |
| Employment statusc | 0.51 (0.34–0.75)*** | 0.47 (0.30–0.73)** | 0.49 (0.30–0.82)** | 0.64 (0.46–0.88)** | 0.44 (0.29–0.66)*** | 0.65 (0.46–0.92)* |
| Ethnicityd | 0.53 (0.27–1.03) | 0.53 (0.25–1.13) | 0.46 (0.20–1.06) | 0.67 (0.39–1.16) | 0.81 (0.40–1.66) | 0.73 (0.40–1.33) |
| Education | ||||||
| No high school | 1 | 1 | 1 | 1 | 1 | 1 |
| Some high school | 0.77 (0.22–2.74) | 2.52 (0.50–12.6) | 0.10 (0.02–0.55)** | 0.54 (0.19–1.54) | 1.41 (0.32–6.20) | 0.30 (0.10–0.91)* |
| High school | 1.04 (0.38–2.87) | 2.75 (0.70–10.8) | 0.42 (0.13–1.33) | 1.00 (0.43–2.36) | 2.14 (0.62–7.35) | 0.75 (0.32–1.79) |
| Some college | 1.07 (0.38–3.02) | 2.06 (0.50–8.41) | 0.56 (0.17–1.80) | 0.85 (0.36–2.03) | 1.60 (0.45–5.66) | 0.74 (0.31–1.79) |
| College | 1.48 (0.48–4.63) | 3.04 (0.67–13.8) | 0.44 (0.12–1.67) | 1.19 (0.46–3.05) | 2.40 (0.62–9.25) | 0.83 (0.32–2.19) |
| Graduate school | 0.99 (0.35–2.83) | 1.86 (0.45–7.76) | 0.36 (0.11–1.17) | 0.86 (0.36–2.07) | 1.54 (0.43–5.51) | 0.72 (0.30–1.74) |
| Country | ||||||
| USA | 1 | 1 | 1 | 1 | 1 | 1 |
| Canada | 0.63 (0.23–1.76) | 0.79 (0.24–2.57) | 0.50 (0.13–1.87) | 0.90 (0.41–2.00) | 0.83 (0.30–2.27) | 1.02 (0.41–2.55) |
| UK | 0.84 (0.49–1.45) | 0.67 (0.37–1.22) | 0.69 (0.31–1.51) | 0.95 (0.62–1.46) | 0.65 (0.38–1.10) | 1.01 (0.62–1.65) |
| France | 0.73 (0.44–1.21) | 0.47 (0.26–0.85)* | 1.15 (0.60–2.21) | 1.10 (0.73–1.64) | 0.42 (0.24–0.72)** | 1.55 (1.00–2.42) |
| Spain | 0.85 (0.41–1.77) | 0.38 (0.14–0.99)* | 1.63 (0.70–3.80) | 0.82 (0.47–1.44) | 0.38 (0.17–0.86)* | 1.15 (0.63–2.10) |
| Nicotine dependence score | 1.08 (1.00–1.18) | 1.04 (0.95–1.15) | 1.14 (1.03–1.27)* | 1.08 (1.01–1.15)* | 1.01 (0.93–1.10) | 1.10 (1.03–1.18)** |
| Motivation to quit | 1.07 (0.97–1.19) | 0.99 (0.88–1.11) | 1.21 (1.06–1.38)** | 1.04 (0.96–1.12) | 0.94 (0.85–1.05) | 1.06 (0.98–1.16) |
| Quit attempt in past 3 months | 1.27 (0.82–1.96) | 1.05 (0.63–1.76) | 2.02 (1.19–3.42)** | 1.43 (1.03–2.00)* | 1.33 (0.84–2.09) | 1.26 (0.88–1.81) |
| Cessation medication used in past 3 monthse | 1.06 (0.67–1.69) | 0.89 (0.51–1.55) | 1.05 (0.59–1.89) | 1.35 (0.94–1.93) | 1.15 (0.71–1.85) | 1.30 (0.87–1.89) |
| Change in body mass indexf | 1.03 (0.95–1.12) | 0.99 (0.91–1.09) | 1.02 (0.92–1.13) | 1.04 (0.97–1.12) | 1.06 (0.98–1.15) | 0.99 (0.92–1.07) |
| Change in health scoref | 0.36 (0.16–0.80)* | 0.24 (0.09–0.60)** | 0.47 (0.17–1.26) | 0.20 (0.10–0.40)*** | 0.16 (0.07–0.36)*** | 0.36 (0.18–0.74)** |
| Baseline equivalent to dependent variable | 26.8 (17.9–40.1)*** | 35.9 (21.8–59.2)*** | 46.1 (27.0–78.8)*** | 14.1 (10.3–19.1)*** | 33.1 (21.6–50.8)*** | 13.2 (9.5–18.5)*** |
| Smoking status | ||||||
| Smoker | 1 | 1 | 1 | 1 | 1 | 1 |
| Ex-smoker (< 3 months) | 0.74 (0.37–1.46) | 0.37 (0.14–0.96)* | 1.38 (0.63–3.04) | 0.52 (0.31–0.88)* | 0.34 (0.15–0.78)* | 0.67 (0.38–1.17) |
| Ex-smoker (≥ 3 months) | 0.28 (0.10–0.78)* | 0.25 (0.06–0.94)* | 0.57 (0.18–1.76) | 0.38 (0.20–0.73)** | 0.24 (0.09–0.67)** | 0.67 (0.34–1.31) |
Impact of Short- and Longer-Term Smoking Cessation on Depression and Anxiety Prevalence Among Those with a History of Mental Health Problems
| Prescription for condition in past 2 weeks: OR (95% CI) | Symptom in past 3 months: OR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Any (n = 536) | Depression (n = 536) | Anxiety (n = 536) | Any (n = 536) | Depression (n = 536) | Anxiety (n = 536) | |
| Age | 1.05 (1.02–1.08)** | 1.03 (1.00–1.07) | 1.02 (0.98–1.06) | 1.04 (1.01–1.07) | 1.03 (0.99–1.06) | 1.00 (0.97–1.03) |
| Genderb | 1.16 (0.73–1.84) | 0.82 (0.49–1.38) | 1.88 (1.07–3.32)* | 1.48 (1.00–2.18) | 0.96 (0.59–1.57) | 1.50 (1.01–2.23)* |
| Marriage statusc | 0.72 (0.46–1.12) | 0.47 (0.28–0.79)** | 1.04 (0.60–1.78) | 0.92 (0.63–1.34) | 0.42 (0.26–0.69)** | 0.93 (0.63–1.36) |
| Employment statusd | 0.54 (0.34–0.87)* | 0.47 (0.28–0.79)** | 0.60 (0.33–1.07) | 0.64 (0.42–0.98) | 0.37 (0.22–0.62)*** | 0.75 (0.49–1.14) |
| Ethnicitye | 0.54 (0.23–1.27) | 0.73 (0.29–1.86) | 0.42 (0.16–1.12) | 0.64 (0.30–1.38) | 0.98 (0.40–2.42) | 0.76 (0.36–1.58) |
| Education | ||||||
| No high school | 1 | 1 | 1 | 1 | 1 | 1 |
| Some high school | 0.64 (0.15–2.79) | 1.16 (0.19–6.98) | 0.16 (0.03–1.06) | 0.31 (0.08–1.18) | 0.77 (0.14–4.07) | 0.23 (0.06–0.88)* |
| High school | 1.48 (0.46–4.72) | 2.71 (0.64–11.4) | 0.65 (0.17–2.55) | 0.85 (0.28–2.57) | 1.77 (0.47–6.69) | 0.72 (0.24–2.10) |
| Some college | 1.36 (0.42–4.48) | 1.96 (0.45–8.57) | 0.72 (0.18–2.90) | 0.74 (0.24–2.27) | 1.43 (0.37–5.55) | 0.67 (0.22–2.00) |
| College | 2.45 (0.65–9.17) | 3.44 (0.69–17.2) | 0.58 (0.12–2.80) | 0.80 (0.24–2.71) | 1.50 (0.33–6.83) | 0.63 (0.19–2.10) |
| Graduate school | 1.07 (0.32–3.57) | 1.44 (0.32–6.53) | 0.37 (0.09–1.54) | 0.72 (0.23–2.24) | 1.13 (0.29–4.50) | 0.66 (0.22–2.00) |
| Country | ||||||
| USA | 1 | 1 | 1 | 1 | 1 | 1 |
| Canada | 0.42 (0.11–1.57) | 0.92 (0.19–4.37) | 0.17 (0.03–0.88)* | 0.46 (0.14–1.48) | 0.38 (0.09–1.63) | 0.71 (0.20–2.49) |
| UK | 0.71 (0.37–1.38) | 0.55 (0.27–1.11) | 0.64 (0.27–1.55) | 0.69 (0.39–1.22) | 0.45 (0.23–0.87)* | 0.70 (0.39–1.27) |
| France | 0.46 (0.25–0.84)* | 0.33 (0.17–0.65)** | 0.74 (0.35–1.53) | 0.62 (0.37–1.05) | 0.26 (0.13–0.49)*** | 0.92 (0.54–1.57) |
| Spain | 0.61 (0.25–1.46) | 0.34 (0.12–0.99)* | 1.17 (0.44–3.15) | 0.53 (0.26–1.10) | 0.29 (0.11–0.75)* | 0.83 (0.40–1.73) |
| Nicotine dependence score | 1.06 (0.96–1.17) | 1.01 (0.91–1.13) | 1.11 (0.99–1.25) | 1.07 (0.99–1.16) | 1.00 (0.90–1.11) | 1.07 (0.98–1.16) |
| Motivation to quit | 1.07 (0.94–1.21) | 1.02 (0.89–1.17) | 1.19 (1.02–1.38)* | 1.02 (0.92–1.13) | 0.97 (0.85–1.10) | 1.04 (0.93–1.15) |
| Quit attempt in past 3 months | 1.04 (0.61–1.77) | 0.78 (0.42–1.45) | 2.03 (1.10–3.74)* | 1.56 (1.00–2.43) | 1.12 (0.62–2.00) | 1.31 (0.85–2.04) |
| Cessation medication used in past 3 monthsf | 0.93 (0.53–1.64) | 0.82 (0.43–1.57) | 0.84 (0.43–1.65) | 1.21 (0.75–1.93) | 0.95 (0.52–1.73) | 1.26 (0.79–2.03) |
| Change in body mass indexg | 1.00 (0.90–1.10) | 0.95 (0.85–1.06) | 1.01 (0.90–1.13) | 1.05 (0.96–1.15) | 1.05 (0.94–1.17) | 1.00 (0.91–1.09) |
| Change in health scoreg | 0.56 (0.23–1.36) | 0.36 (0.13–1.00)* | 0.64 (0.23–1.83) | 0.39 (0.18–0.85) | 0.28 (0.11–0.74)* | 0.50 (0.23–1.09) |
| Baseline equivalent to dependent variable | 11.5 (7.13–18.5)* | 13.6 (7.92–23.4)*** | 23.9 (13.0–44.0)*** | 3.94 (2.47–6.27) | 12.6 (7.63–21.0)*** | 5.24 (3.41–8.06)* |
| Smoking status | ||||||
| Smoker | 1 | 1 | 1 | 1 | 1 | 1 |
| Ex-smoker (<3 months) | 0.76 (0.35–1.65) | 0.40 (0.15–1.09) | 1.28 (0.52–3.18) | 0.53 (0.28–0.98) | 0.36 (0.14–0.92)* | 0.66 (0.34–1.25) |
| Ex-smoker (≥3 months) | 0.24 (0.07–0.77)* | 0.26 (0.06–1.05) | 0.48 (0.13–1.80) | 0.39 (0.18–0.85) | 0.33 (0.11–1.02) | 0.65 (0.29–1.43) |
Discussion
References
Information & Authors
Information
Published In
History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).