VA/DOD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder: Clinician Summary
Abstract
Introduction
| # | Recommendation | Strength | Category |
|---|---|---|---|
| A. General Clinical Management | |||
| 1 | We recommend engaging patients in shared decision making (SDM), which includes educating patients about effective treatment options. | Strong For | Not Reviewed, Amended |
| 2 | For patients with posttraumatic stress disorder (PTSD) who are treated in primary care, we suggest collaborative care interventions that facilitate active engagement in evidence-based treatments. | Weak For | Reviewed, New-replaced |
| B. Diagnosis and Assessment of PTSD | |||
| 3 | We suggest periodic screening for PTSD using validated measures such as the Primary Care PTSD Screen (PC-PTSD) or the PTSD Checklist (PCL). | Weak For | Not Reviewed, Amended |
| 4 | For patients with suspected PTSD, we recommend an appropriate diagnostic evaluation that includes determination of DSM criteria, acute risk of harm to self or others, functional status, medical history, past treatment history, and relevant family history. A structured diagnostic interview may be considered. | Strong For | Not Reviewed, Amended |
| 5 | For patients with a diagnosis of PTSD, we suggest using a quantitative self-report measure of PTSD severity, such as the PTSD Checklist for DSM-5 (PCL-5), in the initial treatment planning and to monitor treatment progress. | Weak For | Not Reviewed, Amended |
| C. Prevention of PTSD | |||
| a. Selective Prevention of PTSD | |||
| 6 | For the selective prevention of PTSD, there is insufficient evidence to recommend the use of trauma-focused psychotherapy or pharmacotherapy in the immediate post-trauma period. | N/A | Reviewed, New-replaced |
| b. Indicated Prevention of PTSD and Treatment of ASD | |||
| 7 | For the indicated prevention of PTSD in patients with acute stress disorder (ASD), we recommend an individual trauma-focused psychotherapy that includes a primary component of exposure and/or cognitive restructuring. | Strong For | Reviewed, New-replaced |
| 8 | For the indicated prevention of PTSD in patients with ASD, there is insufficient evidence to recommend the use of pharmacotherapy. | N/A | Reviewed, New-replaced |
| D. Treatment of PTSD | |||
| a. Treatment Selection | |||
| 9 | We recommend individual, manualized trauma-focused psychotherapy (see Recommendation 11) over other pharmacologic and non-pharmacologic interventions for the primary treatment of PTSD. | Strong For | Reviewed, New-added |
| 10 | When individual trauma-focused psychotherapy is not readily available or not preferred, we recommend pharmacotherapy (see Recommendation 17) or individual non-trauma-focused psychotherapy (see Recommendation 12). With respect to pharmacotherapy and non-trauma-focused psychotherapy, there is insufficient evidence to recommend one over the other. | Strong For | Reviewed, New-added |
| b. Psychotherapy | |||
| 11 | For patients with PTSD, we recommend individual, manualized trauma-focused psychotherapies that have a primary component of exposure and/or cognitive restructuring to include Prolonged Exposure (PE), Cognitive Processing Therapy (CPT), Eye Movement Desensitization and Reprocessing (EMDR), specific cognitive behavioral therapies for PTSD, Brief Eclectic Psychotherapy (BEP), Narrative Exposure Therapy (NET), and written narrative exposure. | Strong For | Reviewed, New-replaced |
| 12 | We suggest the following individual, manualized non-trauma-focused therapies for patients diagnosed with PTSD: Stress Inoculation Training (SIT), Present-Centered Therapy (PCT), and Interpersonal Psychotherapy (IPT). | Weak For | Reviewed, New-replaced |
| 13 | There is insufficient evidence to recommend for or against psychotherapies that are not specified in other recommendations, such as Dialectical Behavior Therapy (DBT), Skills Training in Affect and Interpersonal Regulation (STAIR), Acceptance and Commitment Therapy (ACT), Seeking Safety, and supportive counseling. | N/A | Reviewed, New-replaced |
| 14 | There is insufficient evidence to recommend using individual components of manualized psychotherapy protocols over or in addition to the full therapy protocol. | N/A | Reviewed, New-added |
| 15 | We suggest manualized group therapy over no treatment. There is insufficient evidence to recommend using one type of group therapy over any other. | Weak For | Reviewed, New-replaced |
| 16 | There is insufficient evidence to recommend for or against trauma-focused or non-trauma-focused couples therapy for the primary treatment of PTSD. | N/A | Reviewed, Amended |
| c. Pharmacotherapy | |||
| 17 | We recommend sertraline, paroxetine, fluoxetine, or venlafaxine as monotherapy for PTSD for patients diagnosed with PTSD who choose not to engage in or are unable to access trauma-focused psychotherapy. | Strong For | Reviewed, New-replaced |
| 18 | We suggest nefazodone, imipramine, or phenelzine as monotherapy for the treatment of PTSD if recommended pharmacotherapy (see Recommendation 17), trauma-focused psychotherapy (see Recommendation 11), or non-trauma-focused psychotherapy (see Recommendation 12) are ineffective, unavailable, or not in accordance with patient preference and tolerance. (NOTE: Nefazodone and phenelzine have potentially serious toxicities and should be managed carefully.) | Weak For | Reviewed, New-replaced |
| 19 | We suggest against treatment of PTSD with quetiapine, olanzapine, and other atypical antipsychotics (except for risperidone, which is a Strong Against, see Recommendation 20), citalopram, amitriptyline, lamotrigine, or topiramate as monotherapy due to the lack of strong evidence for their efficacy and/or known adverse effect profiles and associated risks. | Weak Against | Reviewed, New-replaced |
| 20 | We recommend against treating PTSD with divalproex, tiagabine, guanfacine, risperidone, benzodiazepines, ketamine, hydrocortisone, or D-cycloserine, as monotherapy due to the lack of strong evidence for their efficacy and/or known adverse effect profiles and associated risks. | Strong Against | Reviewed, New-replaced |
| 21 | We recommend against treating PTSD with cannabis or cannabis derivatives due to the lack of evidence for their efficacy, known adverse effects, and associated risks. | Strong Against | Reviewed, New-added |
| 22 | There is insufficient evidence to recommend for or against monotherapy or augmentation therapy for the treatment of PTSD with eszopiclone, escitalopram, bupropion, desipramine, doxepin, D-serine, duloxetine, desvenlafaxine, fluvoxamine, levomilnacipran, mirtazapine, nortriptyline, trazodone, vilazodone, vortioxetine, buspirone, hydroxyzine, cyproheptadine, zaleplon, and zolpidem. | N/A | Reviewed, New-replaced |
| d. Augmentation Therapy | |||
| 23 | We suggest against the use of topiramate, baclofen, or pregabalin as augmentation treatment of PTSD due to insufficient data and/or known adverse effect profiles and associated risks. | Weak Against | Reviewed, New-replaced |
| 24 | We suggest against combining exposure therapy with D-cycloserine in the treatment of PTSD outside of the research setting. | Weak Against | Reviewed, New-added |
| 25 | We recommend against using atypical antipsychotics, benzodiazepines, and divalproex as augmentation therapy for the treatment of PTSD due to low quality evidence or the absence of studies and their association with known adverse effects. | Strong Against | Reviewed, New-replaced |
| 26 | There is insufficient evidence to recommend the combination of exposure therapy with hydrocortisone outside of the research setting. | N/A | Reviewed, New-added |
| 27 | There is insufficient evidence to recommend for or against the use of mirtazapine in combination with sertraline for the treatment of PTSD. | N/A | Reviewed, New-replaced |
| e. Prazosin | |||
| 28a | For global symptoms of PTSD, we suggest against the use of prazosin as mono- or augmentation therapy. | Weak Against | Reviewed, New-replaced |
| 28b | For nightmares associated with PTSD, there is insufficient evidence to recommend for or against the use of prazosin as mono- or augmentation therapy. | N/A | Reviewed, New-replaced |
| f. Combination Therapy | |||
| 29 | In partial- or non-responders to psychotherapy, there is insufficient evidence to recommend for or against augmentation with pharmacotherapy. | N/A | Reviewed, New-replaced |
| 30 | In partial- or non-responders to pharmacotherapy, there is insufficient evidence to recommend for or against augmentation with psychotherapy. | N/A | Reviewed, New-replaced |
| 31 | There is insufficient evidence to recommend for or against starting patients with PTSD on combination pharmacotherapy and psychotherapy. | N/A | Reviewed, New-added |
| g. Non-pharmacologic Biological Treatments | |||
| 32 | There is insufficient evidence to recommend for or against the following somatic therapies: repetitive transcranial magnetic stimulation (rTMS), electroconvulsive therapy (ECT), hyperbaric oxygen therapy (HBOT), stellate ganglion block (SGB), or vagal nerve stimulation (VNS). | N/A | Reviewed, New-replaced |
| h. Complementary and Integrative Treatments | |||
| 33 | There is insufficient evidence to recommend acupuncture as a primary treatment for PTSD. | N/A | Reviewed, New-replaced |
| 34 | There is insufficient evidence to recommend any complementary and integrative health (CIH) practice, such as meditation (including mindfulness), yoga, and mantram meditation, as a primary treatment for PTSD. | N/A | Reviewed, New-replaced |
| i. Technology-based Treatment Modalities | |||
| 35 | We suggest internet-based cognitive behavioral therapy (iCBT) with feedback provided by a qualified facilitator as an alternative to no treatment. | Weak For | Reviewed, New-replaced |
| 36 | We recommend using trauma-focused psychotherapies that have demonstrated efficacy using secure video teleconferencing (VTC) modality when PTSD treatment is delivered via VTC. | Strong For | Reviewed, Amended |
| E. Treatment of PTSD with Co-occurring Conditions | |||
| 37 | We recommend that the presence of co-occurring disorder(s) not prevent patients from receiving other VA/DoD guideline-recommended treatments for PTSD. | Strong For | Reviewed, New-added |
| 38 | We recommend VA/DoD guideline-recommended treatments for PTSD in the presence of co-occurring substance use disorder (SUD). | Strong For | Reviewed, New-replaced |
| 39 | We recommend an independent assessment of co-occurring sleep disturbances in patients with PTSD, particularly when sleep problems pre-date PTSD onset or remain following successful completion of a course of treatment. | Strong For | Reviewed, New-replaced |
| 40 | We recommend Cognitive Behavioral Therapy for Insomnia (CBT-I) for insomnia in patients with PTSD unless an underlying medical or environmental etiology is identified or severe sleep deprivation warrants the immediate use of medication to prevent harm. | Strong For | Reviewed, Amended |
How to Use the Clinical Practice Guideline
Grading Recommendations
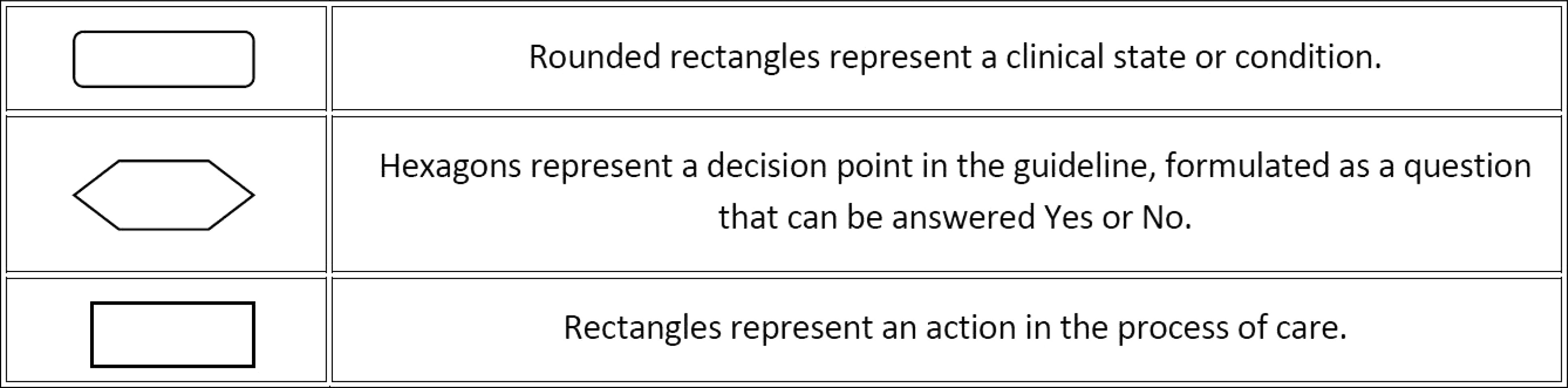
Algorithm
Scope of the Clinical Practice Guideline
Recommendation Discussion
General Clinical Management
Patient-centered Care.

| Sidebar 4. Diagnostic Criteria for Acute Stress Disorder based on DSM-5 | |
|---|---|
| Criterion A | Exposure to actual or threatened death, serious injury or sexual violation in one (or more) of the following way(s): |
| required | 1. Direct exposure |
| 2. Witnessing the event | |
| 3. Learning that a close family member or close friend was exposed to a trauma | |
| 4. Indirect exposure to aversive details of the trauma, usually in the course of professional duties (e.g., first responders, medics) | |
| Criterion B | Presence of nine (or more) of the following symptoms from any of the five categories of intrusion, negative mood, dissociation, avoidance, and arousal, beginning or worsening after the traumatic event(s) occurred: |
| 9 required | The traumatic event is persistently re-experienced, in the following way(s): |
| 1. Intrusive thoughts | |
| 2. Nightmares | |
| 3. Flashbacks | |
| 4. Emotional distress or physical reactivity after exposure to traumatic reminders | |
| Negative mood | |
| 5. Difficulty experiencing positive affect | |
| Dissociative symptoms | |
| 6. Altered sense of reality | |
| 7. Inability to recall key aspects of the trauma | |
| Avoidance of trauma-related stimuli after the trauma, in the following way(s): | |
| 8. Trauma-related thoughts or feelings | |
| 9. Trauma-related reminders | |
| Arousal symptoms | |
| 10. Difficulty sleeping | |
| 11. Irritability or aggression | |
| 12. Hypervigilance | |
| 13. Difficulty concentrating | |
| 14. Heightened startle reaction | |
| Criterion C | Symptoms last three days to one month after trauma exposure |
| Criterion D | Symptoms cause significant distress or functional impairment |
| Criterion E | Symptoms are not due to medication, substance use, or other illness |
Shared Decision Making.
Collaborative Care.

| Sidebar 6. Diagnostic Criteria for Posttraumatic Stress Disorder based on DSM-5 | |
|---|---|
| Criterion A | The person was exposed to: death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence, in the following way(s): |
| required | 1. Direct exposure |
| 2. Witnessing the trauma | |
| 3. Learning that a relative or close friend was exposed to a trauma | |
| 4. Indirect exposure to aversive details of the trauma, usually in the course of professional duties (e.g., first responders, medics) | |
| Criterion B | The traumatic event is persistently re-experienced, in the following way(s): |
| 1 required | 1. Intrusive thoughts |
| 2. Nightmares | |
| 3. Flashbacks | |
| 4. Emotional distress after exposure to traumatic reminders | |
| 5. Physical reactivity after exposure to traumatic reminders | |
| Criterion C | Avoidance of trauma-related stimuli after the trauma, in the following way(s): |
| 1 required | 1. Trauma-related thoughts or feelings |
| 2. Trauma-related reminders | |
| Criterion D | Negative thoughts or feelings that began or worsened after the trauma, in the following way(s): |
| 2 required | 1. Inability to recall key features of the trauma |
| 2. Overly negative thoughts and assumptions about oneself or the world | |
| 3. Exaggerated blame of self or others for causing the trauma | |
| 4. Negative affect | |
| 5. Decreased interest in activities | |
| 6. Feeling isolated | |
| 7. Difficulty experiencing positive affect | |
| Criterion E | Trauma-related arousal and reactivity that began or worsened after the trauma, in the following way(s): |
| 2 required | 1. Irritability or aggression |
| 2. Risky or destructive behavior | |
| 3. Hypervigilance | |
| 4. Heightened startle reaction | |
| 5. Difficulty concentrating | |
| 6. Difficulty sleeping | |
| Criterion F required | Symptoms last for more than one month |
| Criterion G required | Symptoms cause significant distress or functional impairment |
| Criterion H required | Symptoms are not due to medication, substance use, or other illness |
Diagnosis and Assessment of Posttraumatic Stress Disorder

| Guideline Work Group | |
|---|---|
| Department of Veterans Affairs | Department of Defense |
| Nancy C. Bernardy, PhD (Champion) | Charles W. Hoge, MD (Champion) |
| Matthew J. Friedman, MD, PhD (Champion) | David S. Riggs, PhD (Champion) |
| Paula P. Schnurr, PhD (Champion) | Megan J. Ehret, PharmD, MS, BCPP |
| Kathleen M. Chard, PhD | Maj Joel T. Foster, PhD |
| Lori Davis, MD | COL Shawn F. Kane, MD, FAAFP, FACSM |
| Bradford Felker, MD | Kate McGraw, PhD |
| Jessica L. Hamblen, PhD | CDR Jeffrey Millegan, MD, MPH, FAPA |
| Matthew Jeffreys, MD | Elaine P. Stuffel, BSN, MHA, RN |
| Sonya Norman, PhD | COL Lisa A. Teegarden, PsyD |
| Mary Jo Pugh, RN, PhD, FACMPH | CDR Meena Vythilingam, MD |
| Sheila A.M. Rauch, PhD, ABPP | COL Wendi M. Waits, MD |
| Todd P. Semla, MS, PharmD, BCPS, FCCP, AGSF | Jonathan Wolf, MD |
| Office of Quality, Safety and Value Veterans Health Administration | Office of Evidence Based Practice U.S. Army Medical Command |
| Eric Rodgers, PhD, FNP, BC | Corinne K. B. Devlin, MSN, RN, FNP-BC |
| James Sall, PhD, FNP-BC | Elaine P. Stuffel, BSN, MHA, RN |
| Rene Sutton, BS, HCA | |
| Guideline Work Group | |
| Lewin Group | ECRI Institute |
| Clifford Goodman, PhD | James Reston, MPH, PhD |
| Christine Jones, MS, MPH, PMP | Amy Tsou, MD, MSc |
| Erin Gardner, BS | Rebecca Rishar, MLIS |
| Anjali Jain, MD | Jeff Oristaglio, PhD |
| Savvas Pavlides, PhD | |
| Sigma Health Consulting, LLC | DutyFirst Consulting |
| Frances Murphy, MD, MPH | Anita Ramanathan, BA |
| Megan McGovern, BA | |
Prevention of Posttraumatic Stress Disorder
Selective Prevention of Posttraumatic Stress Disorder.
Indicated Prevention of Posttraumatic Stress Disorder and Treatment of Acute Stress Disorder.
Treatment of Posttraumatic Stress Disorder
Treatment Selection.
Psychotherapy.
Pharmacotherapy.
| Quality of Evidence* | Recommend For | Suggest For | Suggest Against | Recommend Against | No Recommendation For or Against |
|---|---|---|---|---|---|
| Moderate | Sertraline^ | Prazosin (excluding the treatment of PTSD associated nightmares) | Prazosin for the treatment of PTSD associated nightmares | ||
| Paroxetine^ | |||||
| Fluoxetine | |||||
| Venlafaxine | |||||
| Low | Nefazodone ± | Quetiapine | Divalproex | Eszopiclone | |
| Olanzapine | Tiagabine | ||||
| Citalopram | Guanfacine | ||||
| Amitriptyline | |||||
| Very Low | Imipramine | Lamotrigine | Risperidone | Bupropion | |
| Phenelzine± | Topiramate | Benzodiazepines | Desipramine | ||
| D-cycloserine | D-serine | ||||
| Hydrocortisone | Escitalopram | ||||
| Ketamine | Mirtazapine | ||||
| No Data† | Antidepressants | ||||
| Doxepin | |||||
| Duloxetine‡ | |||||
| Desvenlafaxine | |||||
| Fluvoxamine‡ | |||||
| Levomilnacipran | |||||
| Nortriptyline | |||||
| Trazodone | |||||
| Vilazodone | |||||
| Vortioxetine | |||||
| Anxiolytic/Hypnotics | |||||
| Buspirone‡ | |||||
| Cyproheptadine | |||||
| Hydroxyzine | |||||
| Zaleplon | |||||
| Zolpidem |
| Quality of Evidence± | Recommend For | Suggest For | Suggest Against | Recommend Against | No Recommendation For or Against |
|---|---|---|---|---|---|
| Moderate | Prazosin (excluding the treatment of PTSD associated nightmares) | Risperidone | Prazosin for the treatment of PTSD associated nightmares | ||
| Low | Topiramate | Divalproex Olanzapine | Hydrocortisone | ||
| Very Low | Baclofen | Mirtazapine and Sertraline^ | |||
| Pregabalin | |||||
| D-cycloserine† | |||||
| No data‡ | Other atypical antipsychotics | Any drug not listed |
Augmentation Therapy
Prazosin
Global Posttraumatic Stress Disorder Symptoms
Nightmares and Sleep Quality
Combination Therapy.
Non-pharmacologic Biological Treatments.
Complementary and Integrative Treatments.
Technology-based Treatment Modalities.
Treatment of Posttraumatic Stress Disorder with Co-occurring Conditions
Background on Co-occurring Conditions with Posttraumatic Stress Disorder.
Appendix
| Therapeutic Category | Initial Dose | Dose Range | Clinical Considerations: Comorbidities and Safety |
|---|---|---|---|
| Antidepressants | ■ Avoid abrupt discontinuation; withdrawal symptoms with sudden discontinuation of SSRIs and SNRIs, paroxetine and venlafaxine in particular | ||
| Monotherapy | |||
| ■ Fluoxetine* | 10-20 mg daily | 20-80 mg daily | |
| ■ Paroxetine* | 10-20 mg daily | 20-50 mg daily | ■ Paroxetine and sertraline have FDA label indications for treating PTSD |
| ■ Sertraline* | 25-60 mg daily | 50-200 mg daily | ■ Common adverse effects of the SSRIs and SNRIs include nausea, headache, diarrhea, anxiety, nervousness, sexual dysfunction, agitation, dizziness, hyponatremia or SIADH, and serotonin syndrome |
| ■ Venlafaxine* | IR: 25 mg 2 or 3 times a day | 75-375 mg in 2-3 divided doses | ■ Venlafaxine can elevate blood pressure; caution advised with patients with hypertension |
| XR: 37.5 mg once daily | 75-225 mg once daily | ||
| ■ Nefazodone± | 25-100 mg 2 times daily | 150-600 mg in 2 divided doses | ■ Nefazodone is associated with life-threatening hepatic failure; monitor for signs and symptoms including LFTs; avoid if active liver disease; do not re-challenge |
| ■ Nefazodone is subject to many drug interactions, particularly those involving CYP3A4 and glycoprotein | |||
| ■ Imipramine± | 25-75 mg daily | 100-300 mg in 1 or 2 divided doses | ■ Avoid TCAs within three months of an acute MI |
| ■ TCAs are relatively contraindicated in patients with coronary artery disease or prostatic enlargement | |||
| ■ TCAs side effects include dry mouth, dry eyes, constipation, orthostatic hypotension, tachycardia, ventricular arrhythmias, weight gain, and drowsiness Photosensitivity may occur | |||
| ■ Phenelzine± | 15 mg 3 times daily | 15 mg daily; 90 mg in divided doses | ■ Phenelzine considerations include drug-drug and drug-food interactions, risk of hypertensive crisis, hypotension, and anticholinergic effects |
References
Information & Authors
Information
Published In
History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).