Physical Assault in the Psychiatry Emergency Room
Abstract
Previous studies of physical assaults in hospitals focused primarily on inpatient psychiatric units, leaving unanswered questions about the extent to which findings generalize to psychiatric emergency rooms. Assault incident reports and electronic medical records from one psychiatric emergency room and two inpatient psychiatric units were reviewed. Qualitative methods were used to identify precipitants. Quantitative methods were used to describe characteristics of each event, as well as demographic and symptom profiles associated with incidents. During the five-year study period, there were 60 incidents in the psychiatric emergency room and 124 incidents on the inpatient units. Precipitating factors, incident severity, means of assault, and interventions were similar in both settings. Among patients in the psychiatric emergency room, a diagnosis of schizophrenia, schizoaffective disorder, or bipolar disorder with manic symptoms (Adjusted Odds Ratio (AOR) 27.86) and presenting with thoughts to harm others (AOR 10.94) were associated with an increased likelihood of having an assault incident report. Similarities between assaults in the psychiatric emergency room and inpatient psychiatric units suggest that the broader literature from inpatient psychiatry can be generalized to the psychiatric emergency room setting, although some differences exist.
Reprinted from J Am Acad Psychiatry Law 2020; 48:484–495, with permission from The American Academy of Psychiatry and the Law. Copyright © 2020
Physical assaults (i.e., nonaccidental physical contact that intimidates or harms another person) are a persistent problem in hospital psychiatry, disrupting the milieu and causing physical injuries, psychological distress, missed workdays, and increased costs.1–9 Estimates of the proportion of patients who commit physical assaults range from 5 to 15 percent of the inpatient population.10,11 Risk factors that may be associated with increased risk of assaultive behavior include younger age, male gender, involuntary admission, history of substance use, history of violence, and certain diagnoses (e.g., schizophrenia).4,10,12 A diverse array of antecedents can precipitate assaultive behaviors, with research suggesting staff–patient interactions (e.g., imposing restrictions on a patient’s behavior or disputes over medication) precede nearly 40 percent of assaults.6 Assaults may not have a clear underlying narrative.6 Importantly, the majority of prior studies examined assaults on inpatient psychiatry units,1–4,6,10,11,13–23 with a smaller literature addressing medical emergency rooms18,24,25 and community settings.3,26–28 Data describing assaults in the psychiatric emergency room are scarce, raising questions about the degree to which lessons learned from inpatient settings are applicable in the psychiatric emergency room.
Differences exist between inpatient units and psychiatric emergency rooms. The psychiatric emergency room is often a small space, where patients are in close proximity, patients are admitted and discharged 24 hours per day, intoxication and withdrawal symptoms may be especially acute, therapeutic programing may be limited, and patients are typically uncertain about their likely disposition. None of these factors is unique to the psychiatric emergency room, but the combination and relative intensities of these factors can make the psychiatric emergency room a unique clinical space. Moreover, psychiatric emergency rooms can vary in their size, location, staffing, and primary population served, raising additional questions about the generalizability of inpatient data to psychiatric emergency room settings.
Of the few studies examining assaults in the psychiatric emergency room, even fewer have described events in detail and assessed risk factors. Dawson et al.29 compared violent and nonviolent patients on 72-hour psychiatric holds in a medical emergency room, but the sample size was small (n=22 violent patients), the definition of violence included verbal altercations, and the analysis did not include multivariate models or adjustments for multiple comparisons. Lynch and Noel30 tested a Risk of Violence Assessment scale in a psychiatric emergency room, attempting to predict future violence in both the psychiatric emergency room and inpatient unit, but their sample was also small (n=32 violent patients) and was limited to a Veterans Affairs hospital with a 95 percent male population. McNiel et al.31 used violence in the two weeks prior to presentation, as well as violence in the psychiatric emergency room, as a predictor of hospitalization rather than an outcome variable, and included fear-inducing behavior (e.g., verbal attacks, threats, attacks on objects) in the definition of violence. Similarly, Way et al.32 studied assaultive behavior in the psychiatric emergency room as a predictor of psychiatric hospitalization rather than an outcome. Terrell et al.,33 examining a related question, reported the frequency of seclusion and restraint in a psychiatric emergency room, but statistical tests were limited to a t test for age.33
Aims of the Study
To address the gaps in this literature, this study uses qualitative and quantitative methods to examine several questions about assaults in an urban psychiatric emergency room. What types of assaultive behaviors occur in the psychiatric emergency room? When do they happen, what are the means of assault, and what are the associated demographic and clinical symptoms? What events and experiences precipitate these behaviors? How do assaults in the psychiatric emergency room compare with assaults on inpatient psychiatric units? Are demographic and clinical predictors the same in both? Ultimately, are the behaviors and circumstances sufficiently similar that literature from inpatient units can be directly applied to a psychiatric emergency room setting, or are there important differences that should be kept in mind?
Methods
Setting
Data were collected at one adult psychiatric emergency room and two adult inpatient psychiatric units at a large, integrated, multi-campus, urban hospital system. The psychiatric emergency room is a locked, 24-bed unit, which operates 24 hours per day and is adjacent to a medical emergency room. The clinical team consists of psychiatrists, nurses, nurse practitioners, social workers, and occupational therapists who evaluate more than 500 patients per month. Regulations allow patients to be kept up to 24 hours for an evaluation or up to 72 hours in an extended observation room. The two inpatient units have 24 and 30 beds. Both have an average length of stay of approximately two weeks, and both are embedded in general medical hospitals. One unit has additional staffing for electroconvulsive therapy, and the other has additional staffing for substance use disorders.
Incidents
Whereas the underlying data source material called each event an assault, this article refers to events as incidents or incident reports to avoid overstating what is known about the events. In particular, the assault label implies culpability and can overlook significant ambiguities about what constitutes intentional versus accidental physical contact, who is perceived as the aggressor and who is engaging in self-defense, and whether the underlying motives are discernable.
Incident reports collected by the department of psychiatry were the primary source for identifying incidents in the psychiatric emergency room. This method is similar to previous studies on inpatient psychiatric units.1,2,18,21,22,34 Hospital staff are trained to complete incident reports for all assaults via an online form, regardless of severity. Any staff member can enter an incident report, and reports can be entered anonymously. Reports include a brief description of what happened, when and where it happened, and who was involved. Incident reports were included in this study if the incident occurred in the psychiatric emergency room between January 2014 and December 2018 and had the classifications General Event Type: Safety/Security, and Specific Event Type: Assault.
The electronic medical record was reviewed for each patient identified in these incident reports to obtain additional narrative descriptions for each incident. Data collected from these narratives were event time (i.e., weekday, hour), location, who was involved in the incident, means of assault (e.g., punch), and interventions following the incident. Incident severity was assessed using the physical aggression subscale on the Modified Overt Aggression Scale (MOAS).35 Initially, two authors (R.E.L. and S.A.R.) assigned MOAS scores to each incident, but after comparing MOAS scores for the first 31 incidents, there was near-perfect agreement (Cohen’s kappa 0.8524, standard error 0.101, 95% CI 0.6548–1), so one author (R.E.L.) assigned MOAS scores for all remaining incidents. This method was also utilized for incident reports originating from the two inpatient psychiatric units during the same time period.
Incident narratives, derived from incident reports and patients’ electronic medical records, were analyzed qualitatively to identify antecedent events and themes that precipitated the incident. A grounded theory approach was used, where themes were allowed to emerge from each narrative. Two authors (R.E.L. and S.A.R.), both psychiatrists with experience in qualitative research, first reviewed the incident narratives. R.E.L. generated a preliminary codebook, which was reviewed by S.A.R., who provided critical review and offered suggestions for clarity and parsimony. R.E.L. and S.A.R. coded each narrative independently and discussed the results. Discrepancies were discussed until consensus was reached. Revisions to the codebook were allowed throughout the coding process, which resulted in some minor modifications, clarifications, and consolidations, but no major changes were made; 90 percent of themes were present in the first 20 narratives, and 100 percent were present in the first 96 narratives, suggesting that theme saturation was achieved. In organizing the resulting list of antecedent events and themes, we generally tried to preserve the focus and specificity of the themes used in the codebook rather than aggregating themes into broad categories, so that the categories would not become vague, overly abstract, or too common to be useful to clinical staff.
Demographic and Clinical Factors
Demographic and clinical characteristics were collected from the electronic medical record for all patients who were mentioned in an incident report. If a patient’s first incident report originated from the psychiatric emergency room, the patient was described as a “psychiatric emergency room patient with an incident report.” If the first incident report originated on an inpatient unit, the patient was described as an “inpatient with an incident report.” Individuals were included only once even if they were involved in more than one incident; five psychiatric emergency room patients had two or more incident reports while in the psychiatric emergency room, two psychiatric emergency room patients had one incident report in the psychiatric emergency room and one incident report on the inpatient unit, and 20 inpatients had two or more incident reports on the inpatient units.
Demographic and clinical characteristics were selected based on previous literature studying agitation, aggression, and assault. Demographic characteristics were gender,1,15,16 age,1,2,15,16 homelessness,14 unemployment,10,14 and legal history.2,15 Historical clinical characteristics were number of prior hospitalizations, prior hospitalization in a state facility, and history of violence.1,2,15,16 Current clinical characteristics were enrollment in assertive community treatment, assisted outpatient treatment,36 and presenting with thoughts to harm self or others.1,2,15 Recent substance use was defined as any self-reported use within two weeks of presentation or positive urine toxicology.1,14–16 Diagnostic categories were schizophrenia, schizoaffective, or bipolar disorder2,14–16; unipolar depression (sometimes associated with decreased assault risk)2,14,16; posttraumatic stress disorder; dementia16; intellectual disability (associated with violence in a forensic setting)37; traumatic brain injury15,16; borderline personality disorder or traits2,10,14; antisocial personality disorder or traits2,10,14,15; and unspecified personality disorder or traits.2,10,14
Although some previous studies treated substance use as a binary category,1,3,4,10,11,15,16 we examined substances individually. Schizophrenia, schizoaffective disorder, and bipolar disorder were combined because their presentations in a psychiatric emergency room can be indistinguishable. Patients with these diagnoses were separated into those with manic symptoms and those without manic symptoms because McNiel et al.13 reported significant bivariate association between diagnosis (i.e., schizophrenia, mania, other) and “physical attacks” in the two weeks prior to involuntary civil commitment (with higher rates for schizophrenia and mania) and in the first 72 hours of commitment (with higher rates for mania).
The control group consisted of individuals seen in the psychiatric emergency room who did not appear in any incident reports. The control group was described as psychiatric emergency room patients with no incident reports. The control group was created by reviewing an administrative list of all patients seen in the psychiatric emergency room, organized by time of arrival. The individual arriving immediately before and immediately after the psychiatric emergency room patient with an incident report was chosen for the control group; if the selected individual was already in the data set, the next person on the list was selected. The reason for matching by time of arrival was to help control for milieu factors (e.g., staffing, waiting time, noise level, census). When reviewing the electronic medical record for each person in the control group, three electronic medical records contained reports of assaultive behavior while in the psychiatric emergency room, but there was no corresponding official incident report. These three individuals were added to the group of psychiatric emergency room patients with incident reports, and additional individuals were selected as controls using the criteria described above.
Data Analysis
Quantitative data were analyzed using Excel 2013 and Stata 15.1 (StataCorp LLC, College Station, Texas). The first analysis used incidents as the unit of analysis, with simple counts and chi-square tests to compare incidents in the psychiatric emergency room with incidents on inpatient psychiatric units. The second analysis was an assessment of demographic and clinical characteristics, which necessitated using individual patient records as the unit of analysis; we acknowledge that in most cases assaultive behavior is better conceptualized as a temporary feature of the illness rather than a permanent feature of the individual. This analysis was a three-way comparison of psychiatric emergency room patients with incident reports versus inpatients with incident reports versus psychiatric emergency room patients with no incident reports. This analysis used chi-square tests for categorical variables and analysis of variance for continuous variables. Post hoc analysis without adjustment was used to detect between-group differences and included t tests for continuous variables and chi-square tests for categorical variables. Variables with statistically significant associations were entered into a conditional logistic regression model comparing demographic and clinical characteristics of psychiatric emergency room patients with incident reports versus psychiatric emergency room patients with no incident reports, which accounted for case–control matching by time of arrival. Statistical significance was defined as P < .05.
This study was approved by the Institutional Review Board at the New York State Psychiatric Institute. Additional details of the methodology can be found in the supplemental materials available in the online version of the article (under Figures & Data).
Results
Incident Characteristics
During the 60-month study period, 184 unique incidents were reported, with 60 incidents in the psychiatric emergency room and 124 incidents on the inpatient psychiatric units. Bivariate comparisons between incidents in the psychiatric emergency room and the inpatient psychiatric units are shown in the supplemental materials. Incidents between a patient and staff were the largest category in both the psychiatric emergency room (n=43, 71.67%) and the inpatient units (n=79, 63.51%). Incidents between patients made up most of the rest of the incidents in the psychiatric emergency room (n=17, 28.34%) and inpatient units (n=44, 35.49%); incidents between a patient and a visitor were rare (n=3 total).
The most common staff victim in the psychiatric emergency room was a security officer (Fig. 1). Incidents in the psychiatric emergency room were more likely to have a security officer victim than incidents on the inpatient units (45% versus 21.8%, chi-square=10.5195, degrees of freedom (df)=1, P <.001). The most common staff victim on the inpatient units was a mental health worker. Incidents on the inpatient units were more likely to have a mental health worker victim than incidents in the psychiatric emergency room (26.6% versus 5%, chi-square=12.0020, df=1, P < .001).
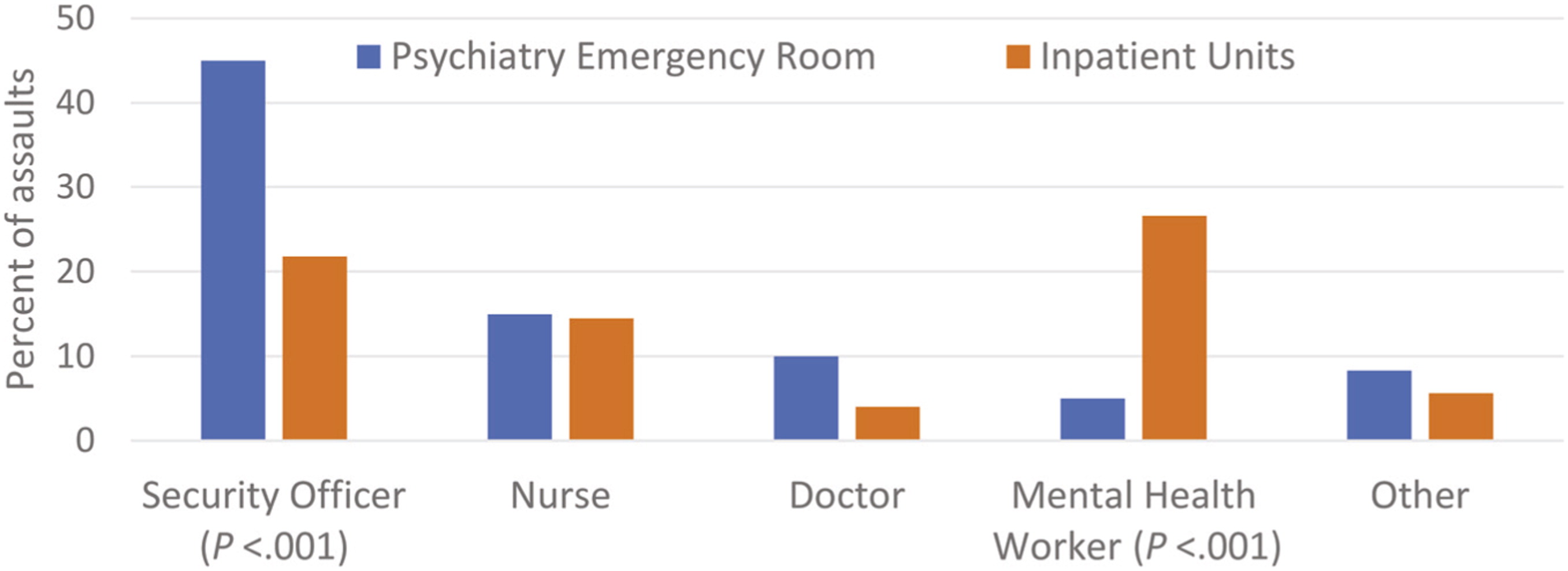
FIGURE 1. Staff victims by role and location. Percent of assault incident reports where staff members were identified as victims in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults). No medical students, nurse practitioners, or physician assistants were assaulted in the study time period.a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
Incident severity was dichotomized between incidents causing no injury (MOAS 0–2) versus incidents causing any injury (MOAS 3–4). Incident severity did not differ between the psychiatric emergency room and inpatient units (chi-square=1.0684, df=1, P=.301). Overall there were three menacing gestures (MOAS=1), 117 incidents without injury (MOAS=2), and 64 incidents with mild injuries (MOAS=3).
Inpatient incidents showed significant variation by time of day and were least common between 12 midnight and 6 a.m. (chi-square 13.7354, df=3, P=.003; null hypothesis was that incidents were evenly distributed throughout 24 hours). Incidents in the psychiatric emergency room did not vary significantly by time of day (P=.41) (Fig. 2). Incidents did not vary by day of week for either the psychiatric emergency room or inpatient units.

FIGURE 2. Incidents by location and time of day. Percent of assault incident reports occurring in each time period in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults).a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
In both locations, punches were the most common means of assault. Means of assault in the psychiatric emergency room were not significantly different from means on the inpatient units (Fig. 3).

FIGURE 3. Means of assault by location. Percent of incidents for each means of assault in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults).a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
The most common intervention after an incident was administration of an intramuscular antipsychotic medication. In the psychiatric emergency room, a higher percentage of incidents involved a manual hold compared with the inpatient units (44.1% versus 25%, chi-square=6.7777, df=1, P=.009). Mechanical restraint or seclusion were used occasionally (Fig. 4).

FIGURE 4. Interventions by location. Percent of incidents where each intervention was utilized in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults). IM, intramuscular.a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
Qualitative Analysis of Precipitating Themes
Twenty antecedent themes were identified as precipitating factors. These were organized into four major categories: psychosis (e.g., disorganization); conflict with peers (e.g., taunting); conflicts with staff (e.g., admission or discharge dispute); and other themes (e.g., family involvement). The most common category in both the psychiatric emergency room and the inpatient units involved themes related to psychosis, especially disorganization and paranoia. Conflicts with peers and conflicts with staff were also common. Precipitating events and their frequencies are described in Table 1.
| Themec | Paradigmatic Examples | Psychiatric Emergency Room, n (%) | Inpatient Units, n (%) |
|---|---|---|---|
| Psychosis | 36 (60) | 71 (57) | |
| Disorganization | Incident is unprovoked and accompanied by other nonsensical behavior | 25 (42) | 56 (45) |
| Paranoia | Patient complains that a person is talking about him or her, then strikes that person | 13 (22) | 20 (16) |
| Perceptual disturbance | Patient has command auditory hallucinations to hurt others | 4 (7) | 10 (8) |
| Conflicts with peers | 8 (13) | 34 (27) | |
| Taunting | One patient calls another patient a derogatory name | 3 (5) | 17 (14) |
| Dispute over limited resource | Two patients want to use the same computer at the same time | 0 (0) | 7 (6) |
| Annoyed by behavior on the unit | A patient is talking loudly and constantly, which is bothering many on the floor and ultimately triggers an incident | 1 (2) | 7 (6) |
| Dispute over personal space or property | A patient enters the wrong room, or roommates disagree on whether the door should be open or closed | 1 (2) | 4 (3) |
| Direct challenge to fight | One patient challenges another patient to fight | 2 (3) | 2 (2) |
| Retaliation | Incident is a response to an argument that started the previous day | 0 (0) | 7 (6) |
| Defending others | Patient thinks someone else is about to be attacked | 1 (2) | 3 (2) |
| Phenomenological escalation | Patients are shadow boxing, then start real boxing | 0 (0) | 2 (2) |
| Conflicts with staff | 20 (33) | 32 (26) | |
| Objection to unit rules or structure | Patient is asked not to stand next to the door | 4 (7) | 18 (15) |
| Admission or discharge dispute | The patient wants immediate discharge | 12 (20) | 12 (10) |
| Perceived needs are not being met | Patient demands opioids for pain | 4 (7) | 4 (3) |
| Other themes | 16 (27) | 37 (30) | |
| Accidental assault | Person is flailing arms without targeting anyone in particular, or a staff member gets pushed while keeping two patients apart | 1 (2) | 3 (2) |
| Dispute involving food | Staff threw away food a patient was intending to eat | 0 (0) | 6 (5) |
| Themes related to sexuality | Patient feels a romantic connection with a staff member and touches the staff member inappropriately, or targets a perceived rival, or feels insulted on the basis of sexuality | 3 (5) | 11 (9) |
| Family involvement | Incident happens after a family visit | 6 (10) | 13 (10) |
| Bodily integrity | Patient thinks he or she is about to be attacked | 2 (3) | 4 (3) |
| No identifiable narrative | Patient is not described as disorganized, but no clear narrative is mentioned | 4 (7) | 1 (1) |
a
The full code book, with definitions for each code or theme, is available in the supplemental materials.
b
There were n=60 total incidents in the psychiatric emergency room and n=124 incidents on the inpatient units.
c
Category counts (e.g., psychosis) may differ from theme count sums (e.g., disorganization, paranoia, perceptual disturbance) because some incidents involved multiple themes within a category.
Demographic and Clinical Characteristics
Psychiatric emergency room patients with incident reports differed from inpatients with incident reports only with respect to antisocial personality disorder or traits, with higher rates reported among psychiatric emergency room patients with incident reports (12.7%) than among inpatients with incident reports (3.0%), but this analysis was limited by low counts in those categories (Table 2).
| Psychiatric Emergency Room Patients with Incident Reports | Inpatients with Incident Reports | Psychiatric Emergency Room Patients with No Incident Reports | Test Statistic (df) | P | Psychiatric Emergency Room Patients with Incident Reports versus Inpatients with Incident Reports | Psychiatric Emergency Room Patients with Incident Reports versus Psychiatric Emergency Room Patients with No Incident Reports | |||
|---|---|---|---|---|---|---|---|---|---|
| Test Statistic (df) | P | Test Statistic (df) | P | ||||||
| Age, y | 37.5 ± 14.3 | 33.2 ± 12.5 | 41.4 ± 15.1 | F(2,262)=6.38a | .0020 | t(153)=1.88b | .062 | t(163)=3.51b | .0006 |
| Categorical variablesc | |||||||||
| Employed | 9 (17.0) | 12 (12.0) | 30 (28.9) | χ2(2)=9.44 | .009 | χ2(1)=0.73 | 0.39 | χ2(1)=2.65 | .104 |
| Prior arrests | 31 (58.5) | 59 (60.2) | 46 (43.0) | χ2(2)=6.97 | .031 | χ2(1)=0.042 | .84 | χ2(1)=3.41 | .065 |
| Current AOT | 6 (11.1) | 5 (5.1) | 2 (1.8) | χ2(2)=6.59 | .037 | χ2(1)=1.92 | .17 | χ2(1)=6.66 | .010 |
| History of violence | 38 (70.4) | 63 (65.6) | 41 (39.8) | χ2(2)=19.11 | <.001 | χ2(1)=0.35 | .56 | χ2(1)=13.24 | <.001 |
| Presented with thoughts to harm others | 27 (49.1) | 50 (50.5) | 14 (12.7) | χ2(2)=39.50 | <.001 | χ2(1)=0.028 | .87 | χ2(1)=25.96 | <.001 |
| Recent cannabinoid use | 25 (45.5) | 39 (39.0) | 29 (26.4) | χ2(2)=6.94 | .031 | χ2(2)=0.61 | .44 | χ2(2)=6.07 | .014 |
| Recent cocaine use | 14 (25.5) | 14 (14.0) | 33 (30.0) | χ2(2)=7.80 | .020 | χ2(2)=3.15 | .076 | χ2(2)=0.37 | .54 |
| Schizophrenia, schizoaffective, or bipolar disorder | χ2(4)=38.09 | <.00 | χ2(2)=1.50 | .47 | χ2(2)=31.62 | <.001 | |||
| None | 6 (10.9) | 14 (14.0) | 37 (33.6) | ||||||
| Yes, without manic symptoms | 22 (40.0) | 47 (47.0) | 61 (55.5) | ||||||
| Yes, with manic symptoms | 27 (49.1) | 39 (39.0) | 12 (10.9) | ||||||
| Unipolar depression | 1 (1.8) | 6 (6.0) | 17 (15.5) | χ2(2)=10.10 | .006 | χ2(2)=1.44 | .23 | χ2(2)=7.02 | .008 |
| Intellectual disability | 5 (9.1) | 11 (11.0) | 1 (0.9) | χ2(2)=9.71 | .008 | χ2(2)=0.14 | .71 | χ2(2)=7.00 | .008 |
| Antisocial personality disorder or traits | 7 (12.7) | 3 (3.0) | 5 (4.6) | χ2(2)=6.73 | .035 | χ2(2)=5.56 | .018 | χ2(2)=3.64 | .056 |
Psychiatric emergency room patients with incident reports: n=55; inpatients with incident reports: n=100; psychiatric emergency room patients with no incident reports: n=110. Data are presented as mean ± SD or n (%). The full analysis with all demographic and clinical variables is available in the supplemental materials.
a
Analysis of variance for parametric continuous variables.
b
Post hoc analyses without adjustment.
c
χ2 test for categorical variables.
df, degrees of freedom; AOT, assisted outpatient treatment.
In bivariate analyses, psychiatric emergency room patients with incident reports were more likely than psychiatric emergency room patients with no incident reports to be younger; to be enrolled in assisted outpatient treatment; to have a reported history of violent behavior; to present with thoughts of harming others; to report recent use of cannabinoids (natural or synthetic); and to have a diagnosis of schizophrenia, schizoaffective disorder, or bipolar disorder with manic symptoms or a diagnosis of intellectual disability. Unipolar depression was less common among psychiatric emergency room patients with incident reports than among psychiatric emergency room patients with no incident reports (Table 2).
Psychiatric emergency room patients with incident reports were compared with psychiatric emergency room patients with no incident reports using a conditional logistic regression model that included all variables associated with incident reports (Table 2). In this model, a diagnosis of schizophrenia, schizoaffective disorder, or bipolar disorder with manic symptoms (adjusted odds ratio (AOR) 27.86, 95% CI 1.18–656.85, P=.039) and presenting with thoughts of harming others (AOR 10.94, 95% CI 1.01–118.94, P=.049) were associated with increased likelihood of having an incident report. Older age was associated with lower likelihood of having an incident report (AOR 0.93, 95% CI 0.86–0.999, P=.048) (Table 3).
| Crude Odds Ratio (95% CI) | P | Adjusted Odds Ratio (95% CI) | P | |
|---|---|---|---|---|
| Age | 0.96 (0.94–0.99) | .002 | 0.93 (0.86–0.999) | .048 |
| Gender | ||||
| Male | 1.00a | 1.00a | ||
| Female | 0.73 (0.35–1.51) | .397 | 0.15 (0.007–2.68) | .194 |
| Employment | ||||
| Employed | 1.00a | 1.00a | ||
| Unemployed | 2.04 (0.88–4.67) | .094 | 2.35 (0.38–14.41) | .356 |
| Prior arrest | ||||
| No | 1.00a | 1.00a | ||
| Yes | 1.88 (0.94–3.79) | .075 | 0.53 (0.075–3.74) | .525 |
| Current AOT | ||||
| No | 1.00a | 1.00a | ||
| Yes | 12.96 (1.44–99.67) | .021 | 0 (0–infinity) | .995 |
| History of violence | ||||
| No | 1.00a | 1.00a | ||
| Yes | 3.69 (1.71–7.97) | .001 | 4.08 (0.48–35.01) | .200 |
| Presented with thoughts to harm others | ||||
| No | 1.00a | 1.00a | ||
| Yes | 7.13 (2.91–17.50) | <.001 | 10.94 (1.01–118.94) | .049 |
| Recent cannabinoid useb | ||||
| No | 1.00a | 1.00a | ||
| Yes | 2.29 (1.15–4.54) | .018 | 0.33 (0.028–3.75) | .370 |
| Schizophrenia, schizoaffective, or bipolar disorder | ||||
| None | 1.00a | 1.00a | ||
| Yes, without mania | 2.30 (0.79–6.69) | .128 | 1.10 (0.11–11.14) | .939 |
| Yes, with mania | 19.39 (5.05–74.52) | < .001 | 27.86 (1.18–656.85) | .039 |
| Unipolar depression | ||||
| No | 1.00a | 1.00a | ||
| Yes | 0.12 (0.02–0.88) | .038 | 0.56 (0.02–12.57) | .712 |
| Intellectual disability | ||||
| No | 1.00a | 1.00a | ||
| Yes | 10.00 (1.17–85.59) | .036 | 0 (0–infinity) | .994 |
| Antisocial personality disorder | ||||
| No | 1.00a | 1.00a | ||
| Yes | 2.80 (0.89–8.82) | .079 | 1.61 (0.11–23.34) | .729 |
a
Reference value.
b
Including synthetic cannabinoids. AOT, assisted outpatient treatment.
Discussion
In this qualitative and quantitative analysis of assault incident reports from the psychiatric emergency room and inpatient psychiatry units, there were similarities across sites in the types of incidents that occurred, as well as in their severity. Our results echo previous literature on risk factors for inpatient assault, including younger age, history of violence, and presenting with thoughts of harming others.1,2,15,16 Previous studies have also reported reduced risk of assaultive behavior among depressed patients2,14,16 and have pointed toward some relationship between psychotic disorders and assault risk.3,4,17 These similarities suggest much of the literature generated on inpatient psychiatry units is applicable to a psychiatric emergency room setting.
Our results also suggest some differences between the two settings regarding which staff members are at highest risk, the use of manual holds, associations with time of day, and the possible role of antisocial personality disorder. Awareness of these differences could inform staff training and preparation, especially for mental health workers and security officers.
Although identifying risk factors associated with assaultive behavior is valuable, it is also true that assaultive behavior is notoriously difficult to predict. If patients are confused, intoxicated, impulsive, intellectually disabled, or motivated by an internal logic known only to the patient, staff might have difficulty knowing what the patient is thinking, feeling, or trying to do, and so might have difficulty anticipating and preempting assaultive behaviors. This challenge could partially explain why these situations result in assaults rather than successful de-escalations. Other studies have noted that in-hospital assaults can be difficult to predict. Grassi et al.10 reported that the cause of violence was not immediately apparent in 44.4 percent of 116 cases. Hillbrand et al.2 reviewed charts for three days before each of 104 incidents of assault by forensic inpatients and found no prodromal signs in 20 incidents. Papadopoulos et al.,6 reported in their meta-analysis that there was no clear cause for 33 percent of incidents; they are correct to highlight the important role that staff play in identifying cues and intervening to prevent violence from occurring. Tam et al. are likely also correct to warn that “[t]he myth that all violence can be spotted early and dealt with should be dispelled” (Ref. 13, p 87).
Previous studies have reported heightened rates of in-hospital violence among patients with manic symptoms.13 This may represent selection bias, in that patients with this condition who are exhibiting dangerous behavior might be especially likely to receive treatment in a psychiatric emergency room or inpatient unit. It is also possible that patients who exhibit aggressive behavior might be especially likely to receive a diagnosis of mania. These results are also consistent with the possibility, even when clinical staff identify risk factors and implement appropriate interventions for each patient, that these interventions might produce less immediate effect for patients with manic symptoms.
Although most individuals with schizophrenia are not violent, debate does exist over whether schizophrenia is associated with increased risk of violence in the hospital. Many previous studies have reported this association,3,4,17 but some recent studies have noted no such association.2,21,22,30 Importantly, many of these studies used “schizophrenia” as a collective term that included multiple diagnoses, and the publications did not always specify what was included. For instance, Dack et al. grouped patients into three categories: “schizophrenic (including schizoaffective, etc.), affective (depression, mania, etc.) and other (personality disorder, organic brain syndrome, etc.)” (Ref. 4, p 263). Lehman et al.3 used “schizophrenia and other psychoses,” Biancosino et al.17 reported on “schizophrenia and related disorders,” and Sanghani et al.21 separated assaultive patients into a “schizophrenia spectrum” and a “nonschizophrenia spectrum.” Differing definitions likely contribute to heterogeneous results; erroneously identifying schizophrenia as increasing assault risk could increase stigma, promote overly restrictive treatment plans, or divert clinical resources from patients who are actually at increased risk. The finding that patients with schizophrenia, schizoaffective disorder, or bipolar disorder were at heightened risk for assaultive behavior only when manic symptoms were also present, if replicated, might advance discussion by identifying clinical circumstances when these patients might be at increased risk and by emphasizing a treatable symptom.
Multiple studies have reported inpatient nursing staff to be at increased risk of being assaulted, especially nursing assistants, mental health workers, and technicians.20,38 Few studies have addressed risk to security personnel. One analysis of Veterans Health Administration facilities reported slightly higher annual injury rates among security personnel (73.7 injuries per 1,000 employees) than among nursing assistants (71.8 injuries per 1,000 employees).3 A different study at a forensic hospital reported much higher annual injury rates among psychiatric technicians (25.5 per 100 staff) than among facility police officers (5.6 per 100 staff).2 In our study, the fact that security officers were at higher risk in the psychiatric emergency room and mental health workers were at higher risk on inpatient units probably reflects different staffing models. The psychiatric emergency room always has four security officers present and a few mental health workers (i.e., this number varies according to how many patients require 1:1 observation), whereas the inpatient units have multiple mental health workers and typically 0–1 security officers. The person at greatest risk of being assaulted might be whoever is closest to the high-risk patient. This possibility would be consistent with data from the MacArthur Violence Risk Assessment Study, in which discharged patients were followed in the community. Those results indicated that the most common victim of community violence was a close affiliate, such as a spouse, girlfriend, boyfriend, or other friend.27
Several clinical variables were significantly associated with assault risk in bivariate models but not in the logistic regression model. One interpretation is that each bivariate association represents a clinically useful marker of risk, but the variables are too closely related to make independent contributions to the final model due to collinearity (e.g., homelessness, history of violence, substance use, and prior arrest might be measuring similar underlying social factors).
The association between assault risk and recent cannabinoid use invites further study. Associations between marijuana use and violence have been reported occasionally, including among individuals with first-episode psychosis39 and persons who use marijuana after a psychiatric hospitalization,40 but research on this potential relationship is limited.
This study has limitations. Underreporting of incidents is a recognized problem.25 Incident reports and medical records are not comprehensive accounts of events. It is not known if any of these individuals was assaultive outside these three clinical areas, outside the hospital, or outside of this five-year window. While two different inpatient units supplied data, psychiatric emergency room data were limited to one location. Some analyses were limited by low cell counts. Additional factors describing the milieu and staffing factors are likely relevant to specific events but were not obtainable. These findings may not be generalizable to other settings where patients are treated in general emergency rooms without a dedicated space or an interdisciplinary team serving patients with psychiatric emergencies. These findings also do not distinguish between individuals who have one incident versus many incidents.
Another limitation involves the process by which patients in this study were assigned diagnoses. Whereas many diagnoses are defined by time durations lasting weeks or months, patients in the psychiatric emergency room may receive a diagnosis after the psychiatric team has observed the patient only briefly. Many patients had prior visits as well as inpatient and outpatient notes that informed the diagnosis, but other diagnoses were based on one-time assessments. Future studies would benefit greatly if more specific diagnoses could be incorporated, especially if larger sample sizes allowed diagnostic subgroups to be parsed and assessed. For example, a future study with a large sample size could separately assess schizophrenia with agitation, schizoaffective manic episode, and bipolar mania with psychotic features to measure the safety risks associated with each of these symptom states.
The definition of assault used in this study limits direct comparison to other studies that use alternative definitions or primary outcomes. As mentioned in the introduction, other studies of emergency room settings have included verbal altercations29 and fear-inducing behavior31 in their definitions of violence, which likely expands the sample available for analysis but reduces the specificity of the outcome. Unfortunately, the emergency room literature does not include a study comparable with the present analysis, using physical assault as the outcome variable, which is both a limitation of the field and an opportunity for future research. This limitation has been mitigated by assigning MOAS scores to each incident, which helps standardize descriptions of what occurred.
In conclusion, in this study of assault incident reports, incidents in the psychiatric emergency room and on the inpatient units had similar precipitants, means, and clinical interventions, which suggests that much of the broader literature from inpatient psychiatry can be generalized to a psychiatric emergency room setting. Disorganization, manic symptoms, and intellectual disability were potential risk factors that might inform clinicians’ efforts to intervene and use de-escalation techniques before violence occurs. Manic symptoms in particular were strongly associated with assault risk, which presents a treatment opportunity that might decrease risk. Although perfect prediction of assaultive behavior is unlikely to be achieved, there is reason to hope that ongoing education about risk factors and de-escalation techniques can help psychiatric emergency rooms and inpatient units deliver high-quality patient care in an environment that is safe for patients and staff.
Footnote
Disclosures of financial or other potential conflicts of interest: None.
References
1.
Lam JN, McNiel DE, Binder RL: The relationship between patients’ gender and violence leading to staff injuries. Psychiatr Serv 51:1167–1170, 2000
2.
Hillbrand M, Foster HG, Spitz RT: Characteristics and costs of staff injuries in a forensic hospital. Psychiatr Serv 47:1123–1125, 1996
3.
Lehman LS, McCormick RA, Kizer KW: A survey of assaultive behavior in Veterans Health Administration facilities. Psychiatr Serv 50:384–389, 1999
4.
Dack C, Ross J, Papadopoulos C, et al: A review and meta-analysis of the patient factors associated with psychiatric in-patient aggression. Acta Psychiatr Scand 127:255–268, 2013
5.
Ward L: Mental health nursing and stress: maintaining balance. Int J Ment Health Nurs 20:77–85, 2011
6.
Papadopoulos C, Ross J, Stewart D, et al: The antecedents of violence and aggression within psychiatric in-patient settings. Acta Psychiatr Scand 125:425–439, 2012
7.
García I, Kennett C, Quraishi M, Durcan G: Acute Care 2004: A National Survey of Adult Psychiatric Wards in England. London: Sainsbury Centre for Mental Health, 2005
8.
Needham I, Abderhalden C, Halfens RJG, et al: Non-somatic effects of patient aggression on nurses: a systematic review. J Adv Nurs 49:283–296, 2005
9.
Chen SC, Hwu HG, Williams RA: Psychiatric nurses’ anxiety and cognition in managing psychiatric patients’ aggression. Arch Psychiatr Nurs 19:141–149, 2005
10.
Grassi L, Peron L, Marangoni C, et al: Characteristics of violent behaviour in acute psychiatric in-patients: a 5-year Italian study. Acta Psychiatr Scand 104:273–279, 2001
11.
Iozzino L, Ferrari C, Large M, et al: Prevalence and risk factors of violence by psychiatric acute inpatients: a systematic review and meta-analysis. PloS One 10:e0128536, 2015
12.
Amore M, Menchetti M, Tonti C, et al: Predictors of violent behavior among acute psychiatric patients: clinical study. Psychiatry Clin Neurosci 62:247–255, 2008
13.
McNiel DE, Binder RL, Greenfield TK: Predictors of violence in civilly committed acute psychiatric patients. Am J Psychiatry 145:965–970, 1988
14.
Raja M, Azzoni A, Lubich L: Aggressive and violent behavior in a population of psychiatric inpatients. Soc Psychiatry Psychiatr Epidemiol 32:428–434, 1997
15.
Krakowski M, Czobor P: Gender differences in violent behaviors: relationship to clinical symptoms and psychosocial factors. Am J Psychiatry 161:459–465, 2004
16.
George C, Jacob TR, Kumar AV: Pattern and correlates of agitation in an acute psychiatry in-patient setting in a teaching hospital. Asian J Psychiatr 19:68–72, 2016
17.
Biancosino B, Delmonte S, Grassi L, et al: Violent behavior in acute psychiatric inpatient facilities: a national survey in Italy. J Nerv Ment Dis 197:772–782, 2009
18.
Tam E, Engelsmann F, Fugere R: Patterns of violent incidents by patients in a general hospital psychiatric facility. Psychiatr Serv 47:86–88, 1996
19.
Owen C, Tarantello C, Jones M, Tennant C: Repetitively violent patients in psychiatric units. PS 49:1458–61, 1998
20.
Owen C, Tarantello C, Jones M, Tennant C: Violence and aggression in psychiatric units. Psychiatr Serv 49:1452–1457, 1998
21.
Sanghani SN, Marsh AN, John M, et al: Characteristics of patients involved in physical assault in an acute inpatient psychiatric setting. J Psychiatr Pract 23:260–269, 2017
22.
Soliman AE, Reza H: Risk factors and correlates of violence among acutely ill adult psychiatric inpatients. Psychiatr Serv 52:75–80, 2001
23.
Lawrence RE, Perez-Coste MM, Arkow SD, et al: Use of security officers on inpatient psychiatry units. Psychiatr Serv 69:777–783, 2018
24.
Pane GA, Winiarski AM, Salness KA: Aggression directed toward emergency department staff at a university teaching hospital. Ann Emerg Med 20:283–286, 1991
25.
Rose M: A survey of violence toward nursing staff in one large Irish accident and emergency department. J Emerg Nurs 23:214–219, 1997
26.
Newhill CE, Mulvey EP, Lidz CW: Characteristics of violence in the community by female patients seen in a psychiatric emergency service. Psychiatr Serv 46:785–789, 1995
27.
Steadman HJ, Mulvey EP, Monahan J, et al: Violence by people discharged from acute psychiatric inpatient facilities and by others in the same neighborhoods. Arch Gen Psychiatry 55:393–401, 1998
28.
Swanson JW, Holzer CE, Ganju VK, Jono RT: Violence and psychiatric disorder in the community: evidence from the Epidemiologic Catchment Area surveys. Psychiatr Serv 41:761– 770, 1990
29.
Dawson NL, Lachner C, Vadeboncoeur TF, et al: Violent behavior by emergency department patients with an involuntary hold status. Am J Emerg Med 36:392–395, 2018
30.
Lynch DM, Noel HC: Integrating DSM-IV factors to predict violence in high-risk psychiatric patients. J Forensic Sci 55:121–128, 2010
31.
McNiel DE, Myers RS, Zeiner HK, et al: The role of violence in decisions about hospitalization from the psychiatric emergency room. Am J Psychiatry 149:207–212, 1992
32.
Way BB, Evans ME, Banks SM: Factors predicting referral to inpatient or outpatient treatment from psychiatric emergency services. Psychiatr Serv 43:703–708, 1992
33.
Terrell C, Brar K, Nuss S, El-Mallakh RS: Resource utilization with the use of seclusion and restraint in a dedicated emergency psychiatric service. South Med J 111:703–705, 2018
34.
Dietz PE, Rada RT: Battery incidents and batterers in a maximum security hospital. Arch Gen Psychiatry 39:31–34, 1982
35.
Kay SR, Wolkenfeld F, Murrill LM: Profiles of aggression among psychiatric patients. J Nerv Ment Dis 176:539–546, 1988
36.
Swartz MS, Bhattacharya S, Robertson AG, Swanson JW: Involuntary outpatient commitment and the elusive pursuit of violence prevention: a view from the United States. Can J Psychiatry 62:102–108, 2017
37.
McMillan D, Hastings RP, Coldwell J: Clinical and actuarial prediction of physical violence in a forensic intellectual disability hospital: a longitudinal study. J Appl Res Int Dis 17:255–265, 2004
38.
Renwick L, Lavelle M, Brennan G, et al: Physical injury and workplace assault in UK mental health trusts: an analysis of formal reports. Int J Ment Health Nurs 25:355–366, 2016
39.
Rolin SA, Marino LA, Pope LG, et al: Recent violence and legal involvement among young adults with early psychosis enrolled in coordinated specialty care. Early Interv Psychiatry 13:832–840, 2019
40.
Dugre JR, Dellazizzo L, Giguere CE, et al: Persistency of cannabis use predicts violence following acute psychiatric discharge. Front Psychiatry 8:176, 2017
Information & Authors
Information
Published In
History
Published in print: Winter 2023
Published online: 16 January 2023
Keywords
Authors
Competing Interests
Dr. Lawrence is Assistant Professor of Psychiatry, Department of Psychiatry, New York State Psychiatric Institute, New York, NY. Dr. Rolin is Research Fellow, Division of Law, Ethics, and Psychiatry, Department of Psychiatry, New York State Psychiatric Institute, New York, NY. Ms. Looney is Administrator for Psychiatry, Department of Psychiatry, New York Presbyterian Hospital, New York, NY. Dr. Birt is Assistant Professor of Psychiatry, Department of Psychiatry, Columbia University, New York, NY. Dr. Stevenson is Associate Professor of Psychiatry and Director of Psychiatry, Department of Psychiatry, Columbia University, New York, NY. Dr. Dragatsi is Associate Professor of Psychiatry, Columbia University and Associate Clinical Director, Department of Psychiatry, Rockland Psychiatric Center, Orangeburg, NY. Dr. Appelbaum is the Dollard Professor of Psychiatry, Medicine, and Law, and Directory of the Center for Law, Ethics, and Psychiatry, Department of Psychiatry, New York State Psychiatric Institute, New York, NY. Dr. Dixon is the Edna L. Edison Professor of Psychiatry and Director, Division of Behavioral Health Services and Policy Research, Department of Psychiatry, New York State Psychiatric Institute, New York, NY. Address correspondence to: Ryan E. Lawrence, MD, Department of Psychiatry, New York State Psychiatric Institute, Columbia University Medical Center, 1051 Riverside Drive, New York, NY 10032. E-mail: rel2137@cumc.columbia.edu.
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBFigures
FIGURE 1. Staff victims by role and location. Percent of assault incident reports where staff members were identified as victims in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults). No medical students, nurse practitioners, or physician assistants were assaulted in the study time period.a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
FIGURE 2. Incidents by location and time of day. Percent of assault incident reports occurring in each time period in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults).a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
FIGURE 3. Means of assault by location. Percent of incidents for each means of assault in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults).a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
FIGURE 4. Interventions by location. Percent of incidents where each intervention was utilized in a psychiatric emergency room (n=60 assaults) and two inpatient psychiatry units (n=124 assaults). IM, intramuscular.a
a A color version of the figure, as originally published, appears in the online version of this article (focus.psychiatryonline.org).
Tables
Media
References
References
1.
Lam JN, McNiel DE, Binder RL: The relationship between patients’ gender and violence leading to staff injuries. Psychiatr Serv 51:1167–1170, 2000
2.
Hillbrand M, Foster HG, Spitz RT: Characteristics and costs of staff injuries in a forensic hospital. Psychiatr Serv 47:1123–1125, 1996
3.
Lehman LS, McCormick RA, Kizer KW: A survey of assaultive behavior in Veterans Health Administration facilities. Psychiatr Serv 50:384–389, 1999
4.
Dack C, Ross J, Papadopoulos C, et al: A review and meta-analysis of the patient factors associated with psychiatric in-patient aggression. Acta Psychiatr Scand 127:255–268, 2013
5.
Ward L: Mental health nursing and stress: maintaining balance. Int J Ment Health Nurs 20:77–85, 2011
6.
Papadopoulos C, Ross J, Stewart D, et al: The antecedents of violence and aggression within psychiatric in-patient settings. Acta Psychiatr Scand 125:425–439, 2012
7.
García I, Kennett C, Quraishi M, Durcan G: Acute Care 2004: A National Survey of Adult Psychiatric Wards in England. London: Sainsbury Centre for Mental Health, 2005
8.
Needham I, Abderhalden C, Halfens RJG, et al: Non-somatic effects of patient aggression on nurses: a systematic review. J Adv Nurs 49:283–296, 2005
9.
Chen SC, Hwu HG, Williams RA: Psychiatric nurses’ anxiety and cognition in managing psychiatric patients’ aggression. Arch Psychiatr Nurs 19:141–149, 2005
10.
Grassi L, Peron L, Marangoni C, et al: Characteristics of violent behaviour in acute psychiatric in-patients: a 5-year Italian study. Acta Psychiatr Scand 104:273–279, 2001
11.
Iozzino L, Ferrari C, Large M, et al: Prevalence and risk factors of violence by psychiatric acute inpatients: a systematic review and meta-analysis. PloS One 10:e0128536, 2015
12.
Amore M, Menchetti M, Tonti C, et al: Predictors of violent behavior among acute psychiatric patients: clinical study. Psychiatry Clin Neurosci 62:247–255, 2008
13.
McNiel DE, Binder RL, Greenfield TK: Predictors of violence in civilly committed acute psychiatric patients. Am J Psychiatry 145:965–970, 1988
14.
Raja M, Azzoni A, Lubich L: Aggressive and violent behavior in a population of psychiatric inpatients. Soc Psychiatry Psychiatr Epidemiol 32:428–434, 1997
15.
Krakowski M, Czobor P: Gender differences in violent behaviors: relationship to clinical symptoms and psychosocial factors. Am J Psychiatry 161:459–465, 2004
16.
George C, Jacob TR, Kumar AV: Pattern and correlates of agitation in an acute psychiatry in-patient setting in a teaching hospital. Asian J Psychiatr 19:68–72, 2016
17.
Biancosino B, Delmonte S, Grassi L, et al: Violent behavior in acute psychiatric inpatient facilities: a national survey in Italy. J Nerv Ment Dis 197:772–782, 2009
18.
Tam E, Engelsmann F, Fugere R: Patterns of violent incidents by patients in a general hospital psychiatric facility. Psychiatr Serv 47:86–88, 1996
19.
Owen C, Tarantello C, Jones M, Tennant C: Repetitively violent patients in psychiatric units. PS 49:1458–61, 1998
20.
Owen C, Tarantello C, Jones M, Tennant C: Violence and aggression in psychiatric units. Psychiatr Serv 49:1452–1457, 1998
21.
Sanghani SN, Marsh AN, John M, et al: Characteristics of patients involved in physical assault in an acute inpatient psychiatric setting. J Psychiatr Pract 23:260–269, 2017
22.
Soliman AE, Reza H: Risk factors and correlates of violence among acutely ill adult psychiatric inpatients. Psychiatr Serv 52:75–80, 2001
23.
Lawrence RE, Perez-Coste MM, Arkow SD, et al: Use of security officers on inpatient psychiatry units. Psychiatr Serv 69:777–783, 2018
24.
Pane GA, Winiarski AM, Salness KA: Aggression directed toward emergency department staff at a university teaching hospital. Ann Emerg Med 20:283–286, 1991
25.
Rose M: A survey of violence toward nursing staff in one large Irish accident and emergency department. J Emerg Nurs 23:214–219, 1997
26.
Newhill CE, Mulvey EP, Lidz CW: Characteristics of violence in the community by female patients seen in a psychiatric emergency service. Psychiatr Serv 46:785–789, 1995
27.
Steadman HJ, Mulvey EP, Monahan J, et al: Violence by people discharged from acute psychiatric inpatient facilities and by others in the same neighborhoods. Arch Gen Psychiatry 55:393–401, 1998
28.
Swanson JW, Holzer CE, Ganju VK, Jono RT: Violence and psychiatric disorder in the community: evidence from the Epidemiologic Catchment Area surveys. Psychiatr Serv 41:761– 770, 1990
29.
Dawson NL, Lachner C, Vadeboncoeur TF, et al: Violent behavior by emergency department patients with an involuntary hold status. Am J Emerg Med 36:392–395, 2018
30.
Lynch DM, Noel HC: Integrating DSM-IV factors to predict violence in high-risk psychiatric patients. J Forensic Sci 55:121–128, 2010
31.
McNiel DE, Myers RS, Zeiner HK, et al: The role of violence in decisions about hospitalization from the psychiatric emergency room. Am J Psychiatry 149:207–212, 1992
32.
Way BB, Evans ME, Banks SM: Factors predicting referral to inpatient or outpatient treatment from psychiatric emergency services. Psychiatr Serv 43:703–708, 1992
33.
Terrell C, Brar K, Nuss S, El-Mallakh RS: Resource utilization with the use of seclusion and restraint in a dedicated emergency psychiatric service. South Med J 111:703–705, 2018
34.
Dietz PE, Rada RT: Battery incidents and batterers in a maximum security hospital. Arch Gen Psychiatry 39:31–34, 1982
35.
Kay SR, Wolkenfeld F, Murrill LM: Profiles of aggression among psychiatric patients. J Nerv Ment Dis 176:539–546, 1988
36.
Swartz MS, Bhattacharya S, Robertson AG, Swanson JW: Involuntary outpatient commitment and the elusive pursuit of violence prevention: a view from the United States. Can J Psychiatry 62:102–108, 2017
37.
McMillan D, Hastings RP, Coldwell J: Clinical and actuarial prediction of physical violence in a forensic intellectual disability hospital: a longitudinal study. J Appl Res Int Dis 17:255–265, 2004
38.
Renwick L, Lavelle M, Brennan G, et al: Physical injury and workplace assault in UK mental health trusts: an analysis of formal reports. Int J Ment Health Nurs 25:355–366, 2016
39.
Rolin SA, Marino LA, Pope LG, et al: Recent violence and legal involvement among young adults with early psychosis enrolled in coordinated specialty care. Early Interv Psychiatry 13:832–840, 2019
40.
Dugre JR, Dellazizzo L, Giguere CE, et al: Persistency of cannabis use predicts violence following acute psychiatric discharge. Front Psychiatry 8:176, 2017