To the Editor: The association between epilepsy and behavioral symptoms has attracted the attention of neurologists and psychiatrists since the 19th century; however, many aspects of this relationship still remain controversial.
1 We report the case of an 8-year-old girl with temporal lobe epilepsy who presented with ictal coprophenomena (coprolalia and copropraxia), as well as aggressive behaviors and multimodal hallucinations.
At the age of 8 years, “A.B.” was referred to the Department of Pediatrics and Child Neuropsychiatry, Sapienza University of Rome, Italy, for pharmaco-resistant epilepsy. She was born at term after an uneventful pregnancy and delivery. Her family history was significant for chronic rheumatic autoimmune disease, but unremarkable for epilepsy. The patient’s early psychomotor development was normal; however, at the age of 6 years and 4 months, she developed polymorphic seizures, which were mainly characterized by absences and drop attacks. At that time, EEG recording showed generalized 3-Hz spike-and-wave discharges lasting nearly 10 seconds, whereas brain MRI raised the possibility of sclerosis of the right hippocampus. A.B. was started on valproate and ethosuximide, which failed to provide adequate control of her seizures.
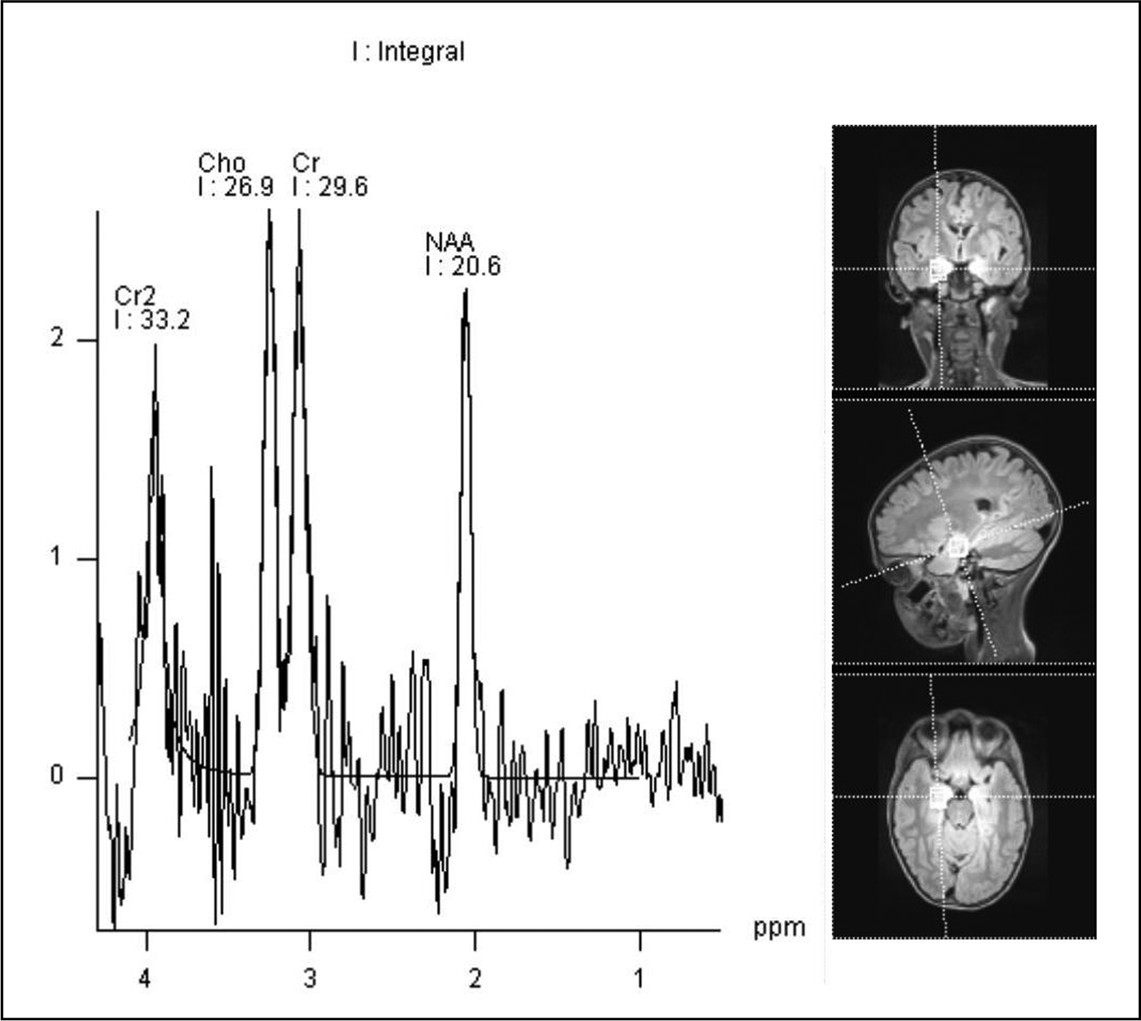
At the age of 7 years and 6 months, A.B.’s epilepsy worsened, with regard to both seizure frequency and severity, as she developed ictal coprophenomena, often associated with prolonged motor manifestations, involving forced touching of objects and aggressive outbursts directed toward herself or other people, in particular, her mother. In addition to perseverative use of abusive language, A.B.’s ictal behavior included repetitive hitting and kicking, plus visual and auditory hallucinations. Repeated EEGs showed epileptiform discharges arising from the temporal area, which spread through the occipital and parietal lobes; moreover, EEG video monitoring documented the association between temporal sharp-waves and ictal coprolalia. Although a further brain MRI scan did not confirm the presence of sclerosis in the right hippocampus, and positron emission tomography (PET) showed normal metabolic activity of both hippocampi, magnetic resonance spectroscopy (MRS) revealed an increase of Cho (Cho/Cr) at the level of both temporal lobes and a peak of the mI in the right temporal lobe, without significant reductions in the concentration of NAA (
Figure 1). A.B.’s antiepileptic medication was reviewed, and she was administered levetiracetam, clonazepam, delorazepam, topiramate, and carbamazepine, without substantial clinical improvement. Her seizures showed a gradual improvement only after the introduction of lamotrigine and, later, with a combination of lamotrigine and vigabatrin.
A.B.’s clinical phenomenology, neurophysiological abnormalities, and metabolite profile alterations (which are consistent with early neuronal damage), suggest an evolving pathological process affecting the mesial aspect of the temporal lobe and resulting in specific epileptic and psychiatric presentations. In addition to alterations of consciousness and psychotic symptoms,
2 our patient displayed coprolalia and copropraxia as ictal phenomena, which have rarely been reported in association with epilepsy in middle childhood.
3 This case highlights shared pathways for the expression of complex partial seizures, ictal alterations of consciousness,
4 and socially inappropriate behaviors, which arguably contribute to the ongoing stigma associated with epilepsy.
5Acknowledgments:
The authors thank Antonio Mittica for his help with the EEG recordings.