Combining two existing therapies for treatment-resistant schizophrenia appears to reduce symptoms effectively, although the duration of the effect remains an open question, according to researchers from Zucker Hillside Hospital in Glen Oaks, N.Y.
When treatment with second-generation antipsychotic medications fails to relieve symptoms of schizophrenia, psychiatrists may turn to clozapine. However, half of such patients may be resistant to clozapine treatment, leaving both physicians and patients with few alternatives.
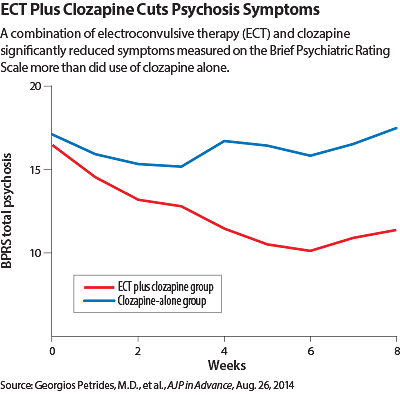
“The treatment of this subgroup of patients remains an enormous challenge, with significant public-health implications,” said Georgios Petrides, M.D., an adjunct associate professor of psychiatry and behavioral sciences at Zucker Hillside, in a study published August 26 in AJP in Advance.
Petrides and colleagues augmented clozapine with electroconvulsive therapy (ECT) in a randomized, single-blind study of 39 patients. All patients continued receiving clozapine, but 20 also received an ECT treatment three times a week for four weeks, then twice a week for another four weeks.
The researchers had conducted pilot studies on several patients and were sufficiently encouraged by the response to move ahead with a clinical trial. ECT was often used to treat people with schizophrenia before the introduction of antipsychotic medications in the 1950s.
The absence of a placebo arm may have helped recruitment, since the study design meant that some patients were randomized to immediate ECT treatment while the others were offered it later, said study co-author Alan Mendelowitz, M.D., an associate professor of psychiatry at Hofstra North Shore-LIJ School of Medicine and unit chief on the resident training research unit at the Zucker Hillside Hospital.
Informed consent in this study population required close attention, Mendelowitz told Psychiatric News. “Every time you do research in a population whose psychosis reduces their capacity to consent, it’s a challenge.”
So they created a questionnaire carefully explaining what the patients were consenting to.
“If they didn’t get it all correct, they did not enter the research protocol,” he said. “Sometimes that ruled out the sickest of the sick.”
Family support was also an important criterion, he said. “You have to find the right patient with the right family, because there is a great burden on them to get the patient to the hospital for treatments and follow-up.”
Response to the combined treatment was defined as a 40 percent reduction in symptoms, twice the standard typically used in medication trials, the researchers noted. Ten of the 20 patients in the clozapine-plus-ECT group achieved that response, compared with none in the clozapine-only cohort. As part of the study’s crossover design, the 19 patients in the control group later received ECT treatment, and nine of them responded.
“These are among the highest response rates ever recorded in this patient population,” Petrides and colleagues said. “The augmentation of clozapine with ECT for the treatment of clozapine-resistant schizophrenia is a safe and effective treatment option.”
The high response rate and blinded rating process used were encouraging and justify looking at this approach in a larger, longer-term study, said William McDonald, M.D., a professor of psychiatry and behavioral sciences and head of the neuromodulation and ECT group at Emory University School of Medicine, in an interview with Psychiatric News.
Several elements of the study’s design enhanced its validity, said McDonald, who was not involved in this study. For instance, the researchers used videotapes from which any spontaneous mention of ECT had been deleted to maintain blinding for the raters.
The researchers included extensive neurocognitive testing throughout the trial to track problems that sometimes crop up with ECT. However, they noted, “Clinically, the degree of cognitive burden shortly after the trial was felt to be consistent with the clinical experience with ECT.”
Significantly, the treatment had no effect on negative symptoms, noted McDonald. “This demonstrates a true response to the schizophrenia and not just to underlying depression.”
Mendelowitz did sound a few cautionary notes at this stage in the research. For example, even with the strong response in this trial, the combination treatment would be hard to replicate in ordinary practice, because in many communities there is no access to ECT and many clinicians do not use clozapine, he said.
Clozapine also requires weekly blood monitoring, and there are significant risks of adverse effects with the medication (see page 21). The initial ECT treatment may require follow-up maintenance sessions, as it does with depression. More significantly, while the researchers have clinically followed some of the patients since the trial ended, they did not receive funding from the National Institute of Mental Health to formally track longer-term outcomes.
“Our clinical impression—and I stress ‘impression’—is that the robust response we saw does not last as long as we had hoped,” said Mendelowitz. “But we are pleased with our findings and hope that this study will lead to further research, and ultimately, to treatment.” ■
“Electroconvulsive Therapy Augmentation in Clozapine-Resistant Schizophrenia: A Prospective, Randomized Study” can be accessed
here.